Download presentation
Presentation is loading. Please wait.

1
Social Insurance … updated © Allen C. Goodman, 2014

2
Social Insurance Started in Germany, in 1880s. Originally employment-related. United States was dragged in kicking and screaming with the Social Security Act of 1935. Medicare and Medicaid were established in 1965. PPACA in 2010.

3
Particularly good places for data Center for Medicare and Medicaid ServicesCenter for Medicare and Medicaid Services Kaiser Family Foundation They update all of the data in this chapter faster than I can.

4
Medicare

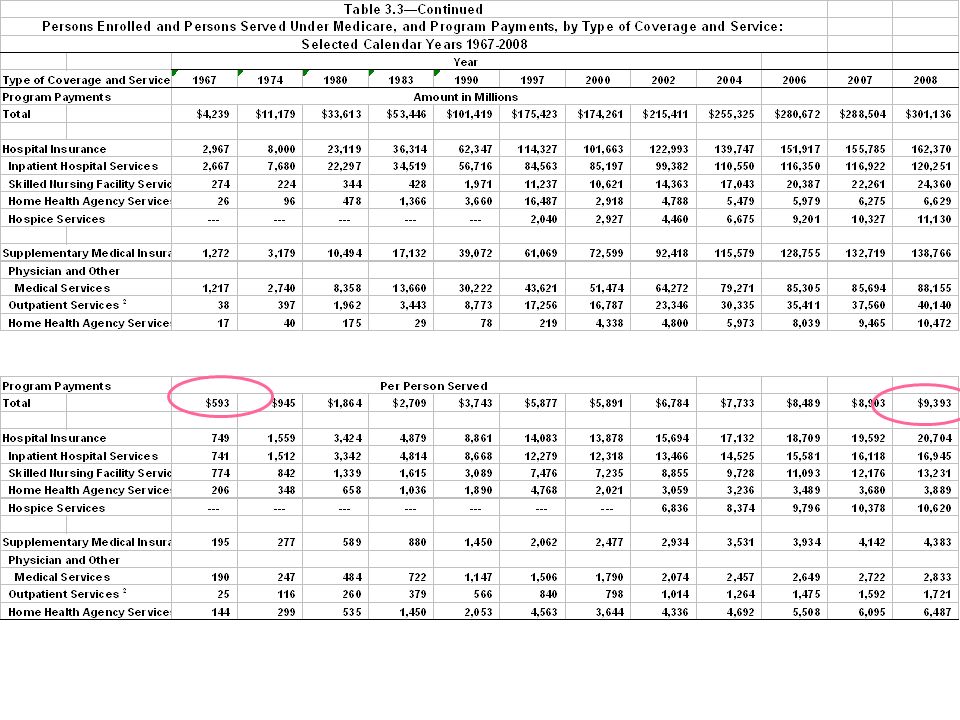
6
Percentage increases

7
Medicare Coverage Part A is generally provided automatically to persons age 65 and over who are entitled to Social Security or Railroad Retirement Board benefits. Medicare’s Part A coverage includes: Inpatient hospital care coverage, requiring an initial deductible payment, plus co-payments for all hospital days following day 60 within a benefit period. Skilled nursing facility (SNF) care, which is generally covered by Part A only if it is within 30 days of a hospitalization of three or more days, and certified as medically necessary. Home Health Agency (HHA) care, including care provided by a home health aide. Hospice, which is provided to those terminally ill persons with a life expectancy of six months or less who elect to forgo standard Medicare benefits, and receive only hospice care.
 care, which is generally covered by Part A only if it is within 30 days of a hospitalization of three or more days, and certified as medically necessary. Home Health Agency (HHA) care, including care provided by a home health aide. Hospice, which is provided to those terminally ill persons with a life expectancy of six months or less who elect to forgo standard Medicare benefits, and receive only hospice care..")
8
Part B Supplementary Medical Insurance (Part B) benefits are available to almost all resident citizens age 65 and over. Part B coverage is optional and requires payment of a monthly premium. Part B covers physician services (in both hospital and non-hospital settings) as well as other services including clinical laboratory tests, diagnostic tests, ambulance services, and blood which was not supplied by Part A.
 as well as other services including clinical laboratory tests, diagnostic tests, ambulance services, and blood which was not supplied by Part A..")
10
Social Security and Medicare Payments – 1990 - 2010 http://www.ssa.gov/OACT/STATS/table4a4.html Part D Drug Coverage

11
Program Financing The Medicare Part A program is financed primarily through a mandatory payroll deduction (FICA tax). The FICA tax is 1.45% of earnings (paid by each employee and by the employer for each), as well as 2.90% for self-employed persons. This tax is paid on all covered wages and self-employment income without limit. One-time deductible at the beginning of each benefit period ($1,260 in 2015).
, as well as 2.90% for self-employed persons. This tax is paid on all covered wages and self-employment income without limit. One-time deductible at the beginning of each benefit period ($1,260 in 2015)..")
12
(2) through contributions from general revenue of the U.S. Treasury, Beneficiary premiums are currently set to cover 25% of the average expenditures for aged beneficiaries. This is NOW means- tested. It didn’t used to be this way. (1) Monthly Payments Medicare Part B
 Monthly Payments Medicare Part B.")
13
Beneficiary Payment Liabilities Parts A and B beneficiaries are responsible for charges not covered by Medicare, and for various cost-sharing features of the plans. These liabilities may be paid by the beneficiary, by a third party such as private “medigap” insurance purchased by the beneficiary, or by Medicaid, if the person is eligible. “Medigap” refers to private health insurance that, within limits, pays most of the health care service charges not covered by Parts A or B of Medicare. For hospital care covered under Part A, the beneficiary’s payment share includes a one-time deductible at the beginning of each benefit period ($1,260 in 2015). This covers the beneficiary’s part of the first 60 days of each spell of inpatient hospital care. If continued inpatient care is needed beyond the 60 days, additional coinsurance payments ($315 per day in 2015) are required through the 90th day of a benefit period. Problem! Many people think Medicare pays for everything Problem! Many people think Medicare pays for everything
. This covers the beneficiary’s part of the first 60 days of each spell of inpatient hospital care. If continued inpatient care is needed beyond the 60 days, additional coinsurance payments ($315 per day in 2015) are required through the 90th day of a benefit period. Problem. Many people think Medicare pays for everything Problem. Many people think Medicare pays for everything.")
14
Beneficiary Payment Liabilities For Part B, the beneficiary’s payment share includes one annual deductible (in 2014/5, $147); Monthly premiums = $104.90 and up. Coinsurance payments for Part B services (usually 20% of the medically allowed charges); a deductible for blood; and payment for any services which are not covered by Medicare. For end-stage renal disease (ESRD) patients, Medicare Part B covers kidney dialysis and physician charges incurred by the patient and donor during the transplant and follow-up care. http://www.medicare.gov/your-medicare-costs/costs-at-a-glance/costs-at-glance.html
; a deductible for blood; and payment for any services which are not covered by Medicare. For end-stage renal disease (ESRD) patients, Medicare Part B covers kidney dialysis and physician charges incurred by the patient and donor during the transplant and follow-up care.")
15
Medicaid Overview Medicaid, referring to Title XIX of the Social Security Act, is a federal-state matching entitlement program that pays for medical assistance for certain vulnerable and needy individuals and families with low incomes and resources. This program is the largest source of funding for medical and health-related services for America’s poorest people. In 2007, it provided health care assistance to more than 50.1 million persons on average, with a total of 62.9 million people enrolled for at least one month. Total expenditures (including CHIP) for fiscal year 2009 were $380.6 billion.
 for fiscal year 2009 were $380.6 billion..")
16
Children’s Eligibility – 2009

17
Children’s Eligibility – 2011

18
Children’s Eligibility – 2011 – 2

19
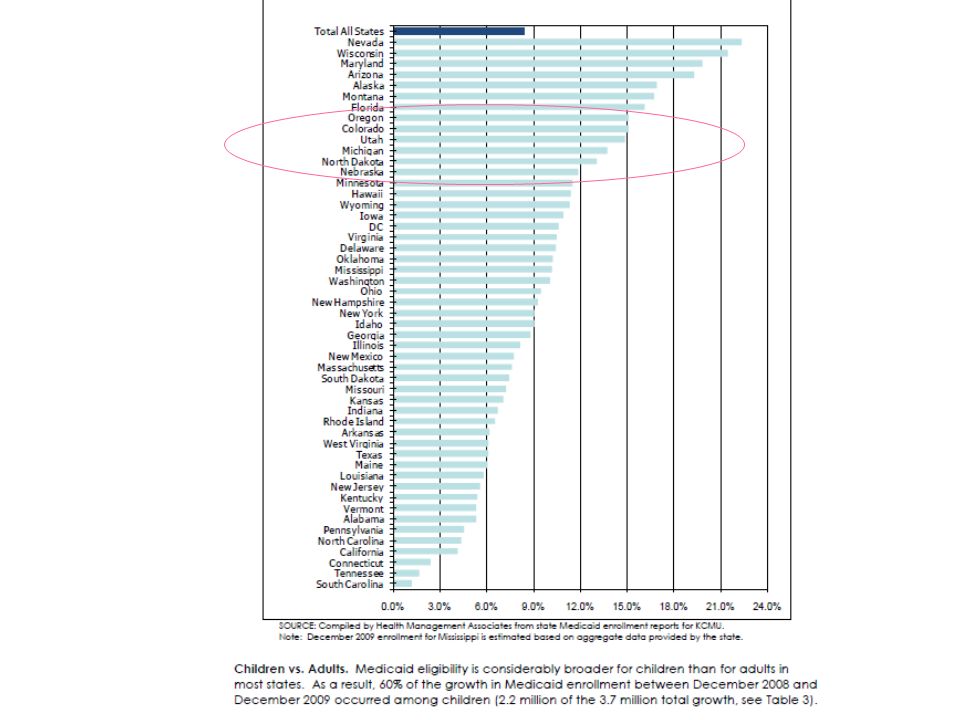
http://www.crcmich.org/column/?p=276 Michigan Chart 1. Total Medicaid Enrollment, Percent Growth from June 2001 through June 2010

20
Total Medicaid Recipients in Michigan by County, June 2011 http://www.crcmich.org/column/?p=276

21
May not be where you think!

22
Comes from the states Within broad national guidelines established by federal statutes, regulations and policies, each state: (1) establishes its own eligibility standards; (2) determines the type, amount, duration, and scope of services; (3) sets the rate of payment for services; and (4) administers its own program. Medicaid policies for eligibility, services, and payment vary considerably even among similar-sized and/or adjacent states. Thus, a person who is eligible for Medicaid in one state might not be eligible in another state; and the services provided by one state may differ.

23
Medicaid Eligibility Medicaid does not provide medical assistance for all poor persons. Even under the broadest provisions of the federal statute, it does not provide health care services even for very poor persons unless they are in one of the designated groups. Low income is only one test for Medicaid eligibility for those within these groups; their resources also are tested against threshold levels (as determined by each state within federal guidelines). States generally have broad discretion in determining which groups their Medicaid programs will cover and the financial criteria for Medicaid eligibility. To be eligible for federal funds, however, states must provide Medicaid coverage for certain individuals who receive federally assisted income-maintenance payments, as well as for related groups not receiving cash payments. What Michigan Pays For - 2005 More recent version
. States generally have broad discretion in determining which groups their Medicaid programs will cover and the financial criteria for Medicaid eligibility. To be eligible for federal funds, however, states must provide Medicaid coverage for certain individuals who receive federally assisted income-maintenance payments, as well as for related groups not receiving cash payments. What Michigan Pays For More recent version.")
24
Payment for Medicaid Services States may impose nominal deductibles, coinsurance, or copayments on some Medicaid recipients for certain services, but certain Medicaid recipients, including pregnant women and children under age 18, are excluded from cost sharing. All Medicaid recipients must be exempt from copayments for emergency services and family planning services. Medicaid is a cost-sharing partnership between the federal government and the states. The federal government pays a share of the medical assistance expenditures under each state’s Medicaid program. That share, known as the Federal Medical Assistance Percentage (FMAP) is determined annually by a formula that compares the state’s average per capita income level with the national income average. States with higher per capita income levels are reimbursed smaller shares of their costs.
 is determined annually by a formula that compares the state’s average per capita income level with the national income average. States with higher per capita income levels are reimbursed smaller shares of their costs..")
25
Federal Medical Assistance Percentages and Enhanced Federal Medical Assistance Percentages On average, the federal share has been 57% Beginning in 2014, the Affordable Care Act (ACA) established highly enhanced FMAPs for the cost of services to low-income adults with incomes up to 138% of the Federal Poverty Level (FPL) who are not currently covered. http://aspe.hhs.gov/health/reports/2014/FMAP2015/fmap15.cfm

26
How the Medicaid match works … Medicaid provides matching funds. BUT federal mandates of program they cannot simply substitute Federal $ for State $. All else Health for poor A* H* A** H**H mandated In particular, Medicaid has provided universal health insurance for children under age 18, whether states wanted it or not. Probably a good thing. A***

27
Match v. Block Grant Block grant can get you to same level of utility, cheaper. All else Health for poor A* H* A** H**H mandated A*** BUT, if it is important to provide a mandated amount of care, a block grant may not be cheaper. … and it could be more expensive.

28
States’ Decisions States must raise taxes for matches. Some have threatened to leave Medicaid, although they’ve not done it. Others have threatened to reduce covered conditions.

29
Medicaid Summary Most Medicaid recipients require relatively small average expenditures per person each year. The 2009 data indicate that Medicaid payments for non-disabled children averaged about $2,848 per child. Per capita spending for non-disabled children ($2,848) and adults ($4,123) was much lower than that for aged ($15,678) and disabled beneficiaries ($16,563). This reflects the differing health status and use of services by the members of these groups. In 2008 Medicaid paid for 40.6% of the total cost of nursing facility care and 34.7% of or home health services care. With the elderly or disabled percentage of the population increasing faster than the younger groups, the need for long-term care is expected to increase.
 and adults ($4,123) was much lower than that for aged ($15,678) and disabled beneficiaries ($16,563). This reflects the differing health status and use of services by the members of these groups. In 2008 Medicaid paid for 40.6% of the total cost of nursing facility care and 34.7% of or home health services care. With the elderly or disabled percentage of the population increasing faster than the younger groups, the need for long-term care is expected to increase..")
30
The Medicaid — Medicare Relationship The Medicare and Medicaid programs work jointly for many beneficiaries. Medicare beneficiaries who have low incomes and limited resources may also receive help from the Medicaid program. For those eligible for full Medicaid coverage, the Medicare health care coverage is supplemented by services that are available under their state’s Medicaid program, according to eligibility category. These additional services may include, for example, nursing facility care beyond the 100 day limit covered by Medicare, prescription drugs, eyeglasses, and hearing aids. For persons enrolled in both programs, any services that are covered by Medicare are paid for by the Medicare program before any payments are made by the Medicaid program, since Medicaid is always “payer of last resort.”

31
CMS estimates that Medicaid provided some supplemental health coverage for at least 8.8 million persons who were Medicare beneficiaries. Medicare prescription drug benefit, started in 2006, includes all who previously received coverage from Medicaid. The Medicaid — Medicare Relationship

32
Conflicting Incentives Either Medicare or Medicaid may have the incentive to shift costs to the other. Medicare is the primary payer for dual eligibles’ hospital, physician, and other acute medical care; Medicaid (according to the states’ discretions) can choose to pay the often considerable Medicare copayments for the dual eligibles. If the states seek to reduce their Medicaid expenditures, they may restrict their cost-sharing paying. This may result in less access and less treatment for beneficiaries in states with more restrictive policies. The adverse incentives can also go in the other direction. Most analysts believe that Medicare’s 1983 adoption of the prospective payment system with DRGs for hospital care, led to patients being discharged “sicker and quicker.” This change in payment contributed to the growth in Medicare-covered post-acute nursing home care in the years following prospective payment.
 can choose to pay the often considerable Medicare copayments for the dual eligibles. If the states seek to reduce their Medicaid expenditures, they may restrict their cost-sharing paying. This may result in less access and less treatment for beneficiaries in states with more restrictive policies. The adverse incentives can also go in the other direction. Most analysts believe that Medicare’s 1983 adoption of the prospective payment system with DRGs for hospital care, led to patients being discharged sicker and quicker. This change in payment contributed to the growth in Medicare-covered post-acute nursing home care in the years following prospective payment..")
33
Conflicting Incentives – What to Do? One possibility is to try to coordinate the two programs. Second possibility – Shift financial responsibility of dual eligibles to federal government. Either Medicare, or some new program. PPACA creates “office of the duals” to look at this.office of the duals

34
“Take-up” and “Crowd-out” What are the net impacts of social insurance program implementation? Are people now insured, who were previously uninsured (take-up), or are the new programs simply crowding out other forms of insurance?
, or are the new programs simply crowding out other forms of insurance .")
35
Improvement Target Population Increased Eligibility Impacts of improving coverage

36
Improvement Target Population Increased Eligibility Previously Uninsured Previously Insured Take-up Crowd- out Crowd- out Additional Coverage Impacts of improving coverage

37
Additional Utilization Additional Coverage Access Impacts of improving coverage

38
Additional Utilization Better Health Outcomes Additional Coverage Access Cost- Effectiveness CE = Cost/ Outcome Incremental Program Costs Impacts of improving coverage

39
Economic Analysis Some value insurance more (D), some less (E). Other Goods Health Insurance VmVm VlVl Some may not even value it at all at current prices (C). This is called a corner solution. D E C
. This is called a corner solution. D E C.")
40
Some may take it who were not insured. Some may take it who were previously insured. Economic Analysis Suppose that the government introduces free public insurance with generosity M. Other Goods Health Insurance VmVm VlVl Some may stay with previous insurance. D E C M

41
Impacts Cutler and Gruber estimate that under Medicaid expansions, about ½ of increase in eligibility has been associated with a reduction in private insurance coverage (crowd-out), and about ½ with take-up.
, and about ½ with take-up.")
42
Supplemental

43
Medicaid Enrollment

Similar presentations


















 MinnesotaCare General Assistance Medical Care (GAMC) Minnesota Comprehensive.>")

 Yale Forman, MD Brown University.>")

