Download presentation
Presentation is loading. Please wait.

1
Preceptor : Dr. Suraj Speaker : Dr. Manik

3
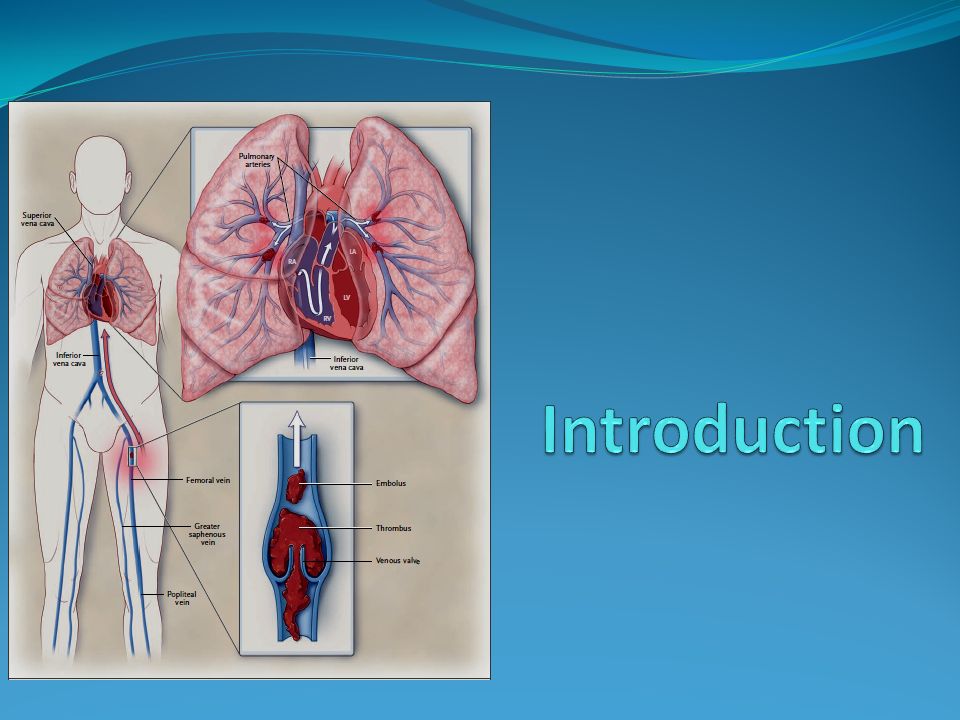
Annual incidence of venous thromboembolism is approximately 0.1 percent, 0.01 percent in early adulthood to nearly 1 % in 60 years old. Venous thromboembolism is responsible for Up to 15% of all in-hospital deaths 20 to 30% of deaths associated with pregnancy and delivery in the United States and Europe. Annual incidence of pulmonary embolism 23 - 69 cases per 100,000 population. Case fatality rate within 2 weeks of diagnosis of approximately 11%

4
The current standard treatment is rapidly acting parenteral anticoagulation for 5 to 7 days followed by at least 3 months of treatment with a vitamin K antagonist. Bates SM et al; N Engl J Med 2004;351:268-77.

5
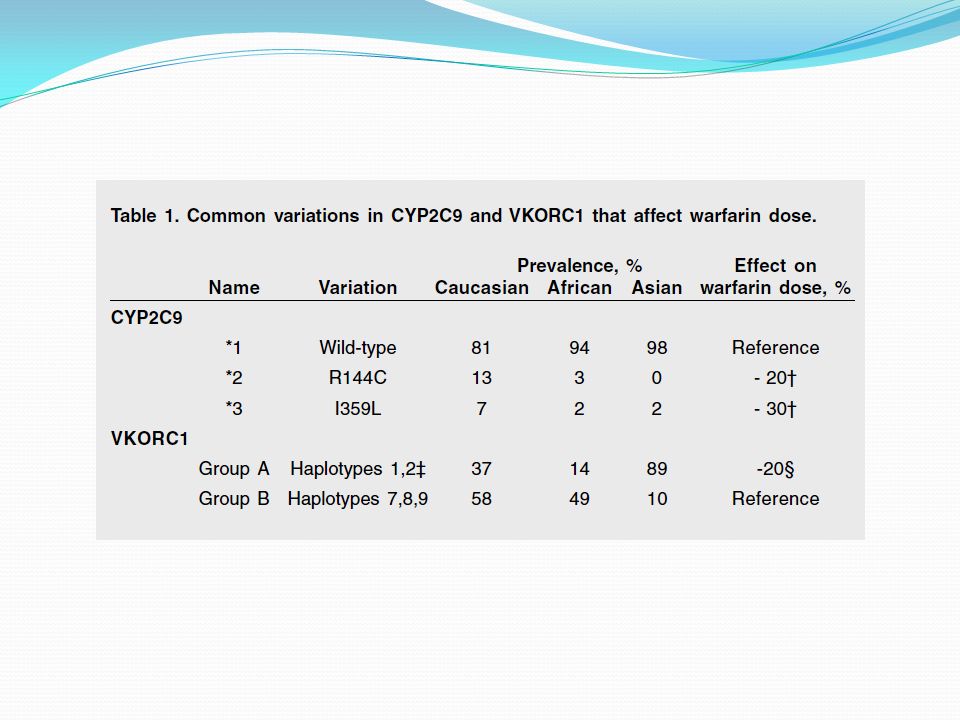
Warfarin is a difficult drug to use Narrow therapeutic margin Delayed onset of action Difficulty with reversal Many interactions with drugs, dietary effects, Wide variation in sensitivity Need for frequent laboratory monitoring.

6
Dabigatran etexilate is direct-acting thrombin inhibitor Prodrug that is rapidly converted by esterases to the active form, dabigatran Absorption is pH sensitive & is decreased by approximately 30% in the presence of proton pump inhibitors. Metabolism is not dependent on cytochrome P- 450 enzymes, reducing the risk of drug interactions. 6 % bioavailability & reaches a peak concentration approximately 2 to 3 hours after ingestion. Terminal plasma half-life is approximately 12 to 17 hours, 80% renal excretion Although dabigatran prolongs the PTT, the effects are not dose dependent with little effect on the PT

7
Randomized, double-blind study, 2076 patients undergoing total knee replacement received dabigatran etexilate, 150 mg or 220 mg once-daily, starting with a half- dose 1–4 h after surgery, or subcutaneous enoxaparin 40 mg once-daily, starting the evening before surgery, for 6–10 days. Patients were followed up for 3 months. Primary efficacy outcome : total VTE (venographic or symptomatic) and mortality during treatment Primary safety outcome : incidence of bleeding events. Both doses were non-inferior to enoxaparin in terms of efficacy or safety. Eriksson BI et al; J Thromb Haemost 2007; 5: 2178–85
 and mortality during treatment Primary safety outcome : incidence of bleeding events. Both doses were non-inferior to enoxaparin in terms of efficacy or safety. Eriksson BI et al; J Thromb Haemost 2007; 5: 2178–85.")
8
Meta-analysis of three head-to-head, phase III, multi- arm, randomized, double-blind, controlled, noninferiority trials (RE-NOVATE, RE-MODEL and RE-MOBILIZE). Dabigatran at a dose of 220 mg once daily was not inferior to the comparator enoxaparin (at either 40 mg once daily or 30 mg twice daily) in reducing levels of total VTE and all-cause mortality among patients undergoing total hip replacement and total knee replacement. Holmes M et al; Health Technology Assessment 2009; Vol. 13: Suppl. 2
 in reducing levels of total VTE and all-cause mortality among patients undergoing total hip replacement and total knee replacement. Holmes M et al; Health Technology Assessment 2009; Vol. 13: Suppl. 2.")
9
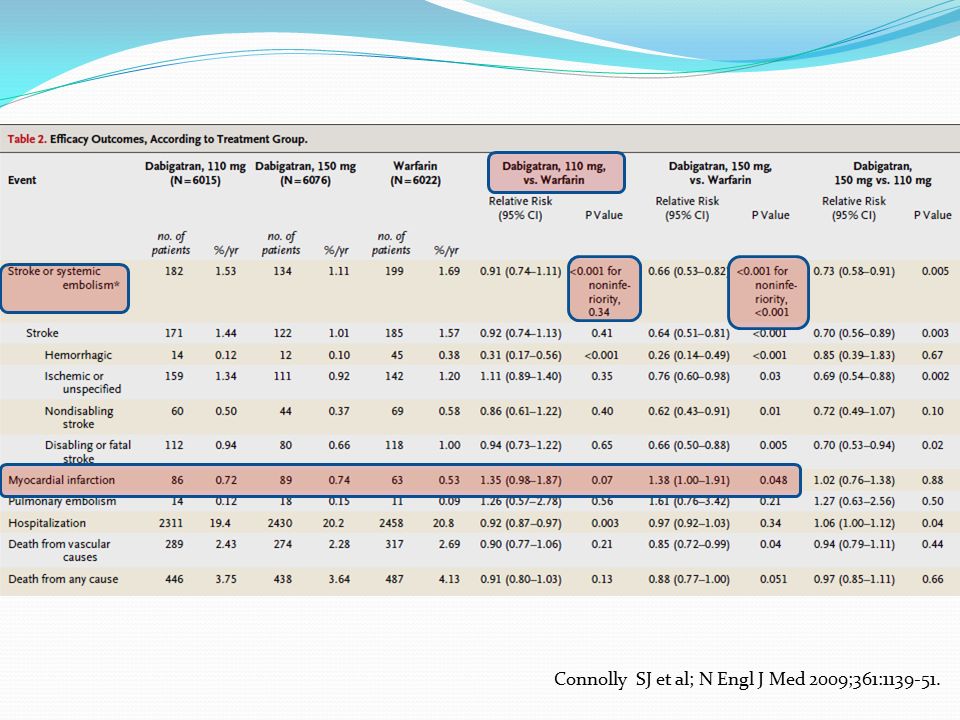
The Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) Randomized trial of 18,113 patients who had atrial fibrillation and a risk of stroke Blinded fixed doses of dabigatran 110 mg or 150 mg twice daily or unblinded adjusted-dose warfarin. Median duration of the follow-up period was 2.0 years. The primary outcome was stroke or systemic embolism. Connolly SJ et al; N Engl J Med 2009;361:1139-51.

13
Randomized, double-blind, noninferiority trial of 2489 patients with acute venous thromboembolism 6 months of treatment with either oral ximelagatran, 36 mg twice daily, or subcutaneous enoxaparin, 1 mg/kg twice daily, for 5 to 20 days followed by warfarin adjusted to maintain INR of 2.0 - 3.0. Thrombin Inhibitor in Venous Thromboembolism [THRIVE] Trial Fiessinger JN et al; JAMA. 2005;293(6):681-689
:")
14
6-month treatment with ximelagatran was generally well tolerated except for the development of increased levels of ALT in about 10% of patients, leading to more frequent discontinuation of study drug in the ximelagatran group Fiessinger JN et al; JAMA. 2005;293(6):681-689
:")
15
A Phase III, Randomised, Double Blind, Parallel- Group Study of the Efficacy and Safety of Oral Dabigatran Etexilate (150 mg Bid) Compared to Warfarin (INR 2.0-3.0) for 6 Month Treatment of Acute Symptomatic Venous Thromboembolism, Following Initial Treatment (5-10 Days) With a Parenteral Anticoagulant Approved for This Indication (RE-COVER™)
 Compared to Warfarin (INR ) for 6 Month Treatment of Acute Symptomatic Venous Thromboembolism, Following Initial Treatment (5-10 Days) With a Parenteral Anticoagulant Approved for This Indication (RE-COVER™)")
16
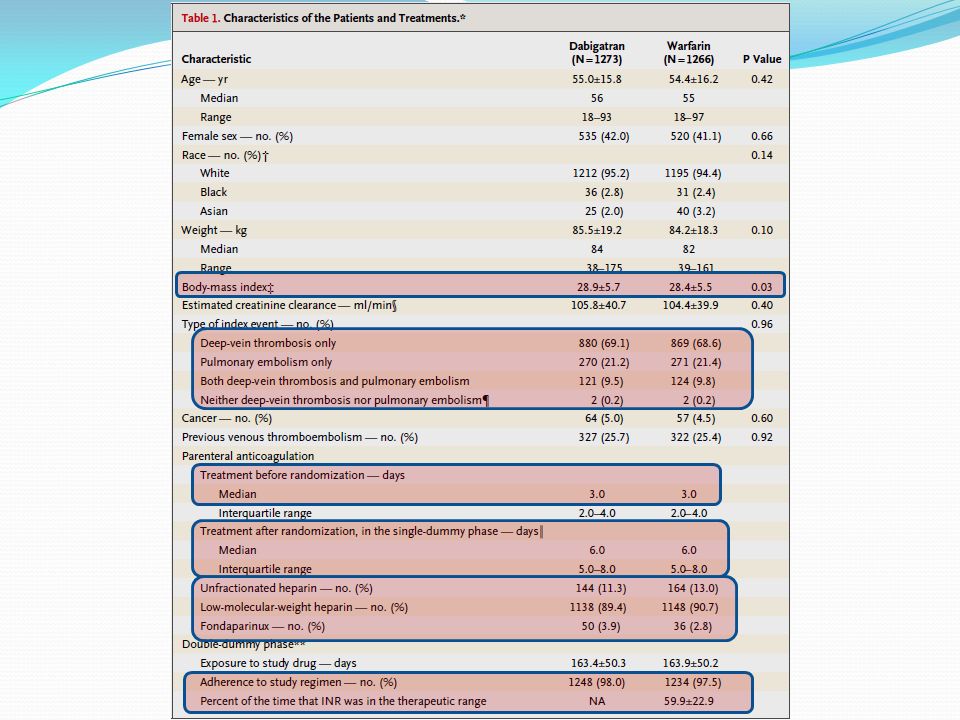
Comparison of 6 months of treatment with dabigatran, at a fixed dose of 150 mg twice daily, with dose-adjusted warfarin therapy, after initial parenteral anticoagulation Double-blind, double-dummy, randomized multicenter trial 228 clinical centers in 29 countries. Study was approved by ethics committees at all participating centers

17
Inclusion criteria Patients 18 years of age or older Acute, symptomatic, objectively verified proximal deep- vein thrombosis of the legs or pulmonary embolism 6 months of anticoagulant therapy was considered to be an appropriate treatment

18
Exclusion criteria Duration of symptoms > 14 days. Pulmonary embolism with hemodynamic instability or requiring thrombolytic therapy. Another indication for warfarin therapy. Recent unstable cardiovascular disease. High risk of bleeding. Liver disease with an aminotransferase level > 2 times the local upper limit of the normal range. Estimated creatinine clearance of < 30 ml /minute. Life expectancy < 6 months. Contraindication to heparin or to radiographic contrast material Pregnancy or risk of becoming pregnant. Requirement for long-term antiplatelet therapy (≤100 mg of acetylsalicylic acid daily was acceptable).
..")
19
Before randomization, the diagnosis of venous thromboembolism was established Compression ultrasonography Venography of leg veins Ventilation–perfusion lung scanning Angiography Spiral computed tomography of pulmonary arteries. Additional baseline examination was performed within 72 hours after randomization. Computer-generated randomization scheme with variable block sizes, stratified according to Presentation : pulmonary embolism or DVT without symptomatic pulmonary embolism. Presence or absence of active cancer.

20
Initial treatment with i.v UFH or s.c LMWH was usually started before random assignment. Assigned in a 1:1 ratio to fixed dose of dabigatran (150 mg BD taken orally) or warfarin. Warfarin or a identical placebo was started on the day of random assignment to achieve an INR of 2.0 to 3.0 on a point-of-care coagulometer that was programmed, in conjunction with the randomization schedule, to yield either a true INR or a sham INR (“single-dummy phase”). Dabigatran or a identical placebo was initiated, and the parenteral anticoagulant was stopped after at least 5 days of treatment and the true or sham INR was ≥ 2 on 2 consecutive days. The first dose of dabigatran was given within 2 hours before the time that the next dose of initial parenteral therapy or at the time of discontinuation of intravenous unfractionated heparin. Active dabigatran and warfarin-like placebo or active warfarin and dabigatran-like placebo were then given for 6 months (“double-dummy phase”).
 or warfarin. Warfarin or a identical placebo was started on the day of random assignment to achieve an INR of 2.0 to 3.0 on a point-of-care coagulometer that was programmed, in conjunction with the randomization schedule, to yield either a true INR or a sham INR ( single-dummy phase ). Dabigatran or a identical placebo was initiated, and the parenteral anticoagulant was stopped after at least 5 days of treatment and the true or sham INR was ≥ 2 on 2 consecutive days. The first dose of dabigatran was given within 2 hours before the time that the next dose of initial parenteral therapy or at the time of discontinuation of intravenous unfractionated heparin. Active dabigatran and warfarin-like placebo or active warfarin and dabigatran-like placebo were then given for 6 months ( double-dummy phase )..")
21
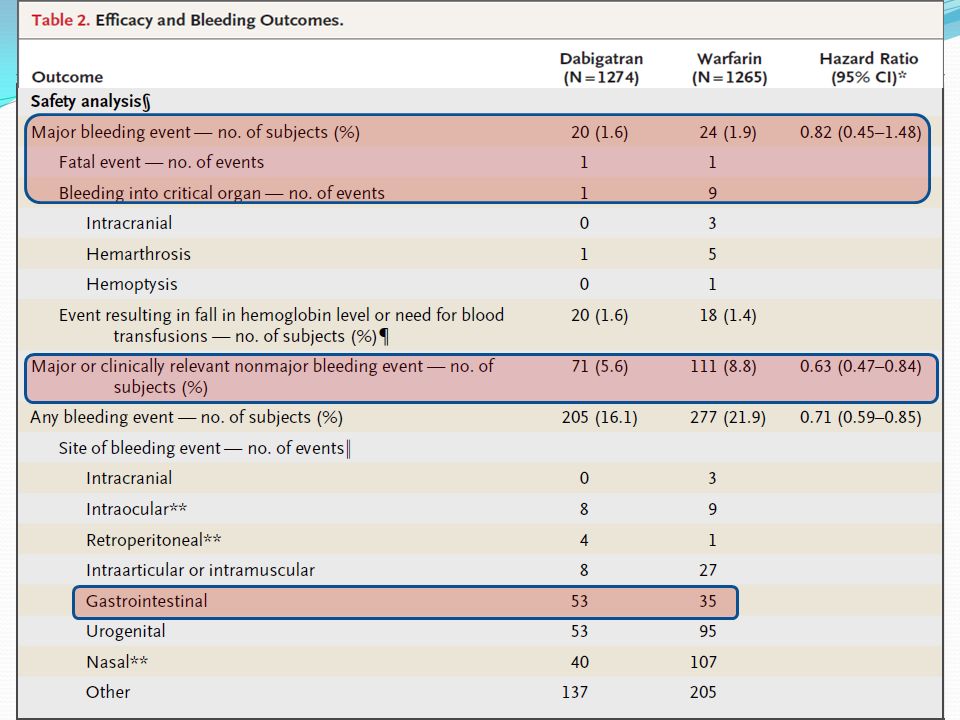
Patients were assessed at 7 days and then monthly until 6 months and were told to contact their study site immediately if symptoms of venous thromboembolism or bleeding. Additional follow-up visit was scheduled for 30 days after completion of the study, unless the patient had discontinued the study drug before 6 months, had started open-label anticoagulant therapy, or had been enrolled in another trial. Symptoms of recurrent venous thromboembolism were evaluated with the use of the same diagnostic methods that had been used for the initial diagnosis. Bleeding was defined as major if it was Clinically overt and if it was associated with a fall in the hemoglobin level of at least 20 g per liter, Need for transfusion of 2 or more units of red cells Involved a critical site Fatal

22
Bleeding was defined as minor if it was Spontaneous skin hematoma of at least 25 cm 2 Spontaneous epistaxis of > 5 minutes Macroscopic hematuria, spontaneous or associated with an intervention, Lasting more than 24 hours Spontaneous rectal bleeding (more than spotting on toilet paper) Gingival bleeding > 5 minutes Bleeding leading to hospitalization &/or requiring surgical treatment Bleeding leading to a transfusion of less than 2 units of whole blood or red cells Any other bleeding event considered clinically relevant by the investigator
 Gingival bleeding > 5 minutes Bleeding leading to hospitalization &/or requiring surgical treatment Bleeding leading to a transfusion of less than 2 units of whole blood or red cells Any other bleeding event considered clinically relevant by the investigator")
23
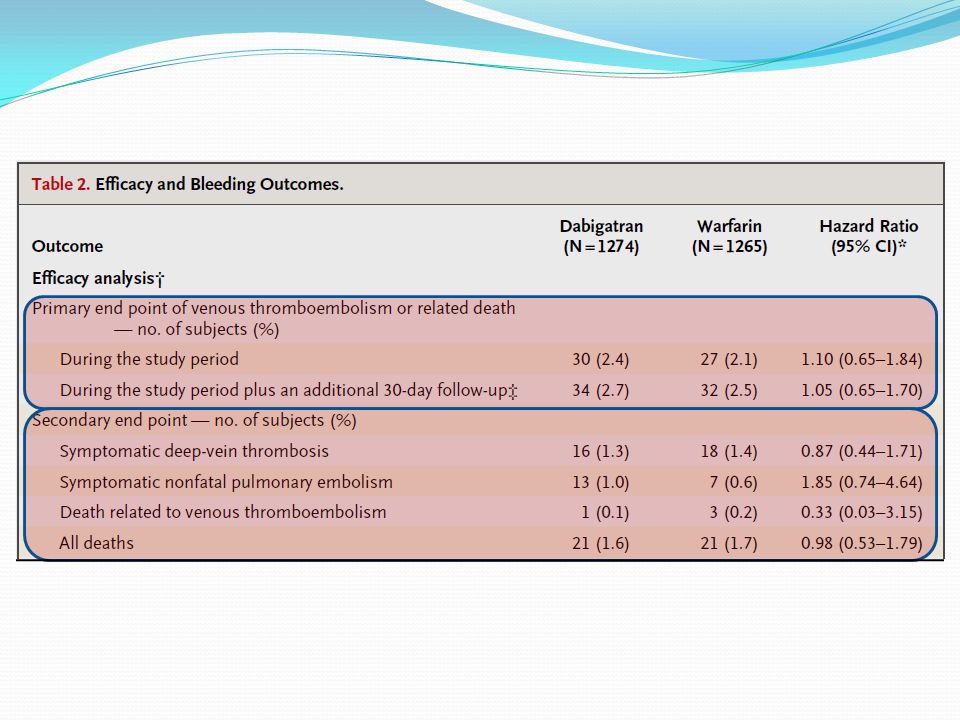
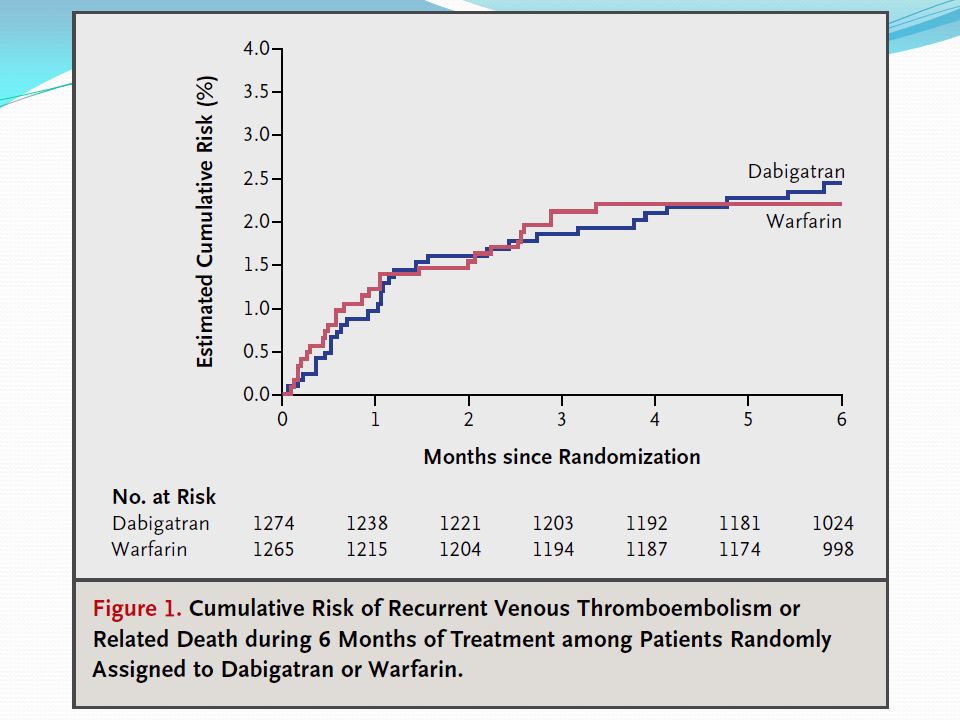
Statistical analysis Non-inferiority trial for efficacy & safety. Efficacy analysis Primary end point Venous thromboembolism or related death Secondary end point — no. of subjects Symptomatic DVT Symptomatic nonfatal pulmonary embolism Death related to venous thromboembolism Safety analysis Major bleeding event Major or clinically relevant nonmajor bleeding event Any bleeding event

24
The sample size was determined on the basis of Expected rate of the primary efficacy outcome of 2% at 6 months in each group. 90% power to exclude a hazard ratio of 2.75 and an absolute increase in risk of 3.6 percentage points for the primary outcome with dabigatran One-sided alpha level of 0.025. Data loss of 20% A sample size of 2550 patients, with 1275 in each group, and an expected total of 46 events No formal interim analyses were planned or performed.

25
Efficacy was analyzed according to a modified intention-to- treat principle Hazard ratio was calculated with the use of the Cox model and the difference in risk calculated with the use of Kaplan–Meier estimates. Statistics were adjusted for the initial presentation (i.e., pulmonary embolism or deep-vein thrombosis) and for the presence or absence of active cancer at baseline If noninferiority was established by both criteria, testing for superiority of dabigatran was to be performed.
 and for the presence or absence of active cancer at baseline If noninferiority was established by both criteria, testing for superiority of dabigatran was to be performed..")
28
Study drug was stopped before 6 months 204 patients (16.0%) in the dabigatran group 126 adverse event 21 non-adherence 9 loss to follow-up 39 withdrawal of consent 9 for other reasons 183 patients (14.5%) in the warfarin group 102 adverse event, 35 no- adherence, 6 loss to follow-up, 36 withdrawal of consent, and 4 for other reasons.
 in the dabigatran group 126 adverse event 21 non-adherence 9 loss to follow-up 39 withdrawal of consent 9 for other reasons 183 patients (14.5%) in the warfarin group 102 adverse event, 35 no- adherence, 6 loss to follow-up, 36 withdrawal of consent, and 4 for other reasons.")
36
Discussions Dabigatran was as effective as warfarin therapy, which achieved INR values within the therapeutic INR range 60% of the time — a rate that is consistent with good- quality management of warfarin dosing. The rates of bleeding with dabigatran were similar to or lower than those with warfarin and there were fewer episodes of non-major bleeding with dabigatran than with warfarin. No evidence of hepatotoxic events associated with dabigatran in contrast with ximelagatran.

37
Limitations Actual sample size was slightly smaller than calculated sample size Dabigtran was given only after initial parenteral anticoagulation therapy had been administered for a median of 9 days. No data to support the use of dabigatran monotherapy for acute venous thromboembolism. Median total duration of parenteral therapy of 9 days is longer than the typical duration; however, the duration of heparin therapy (5 days as compared with 10 days) has not been shown to influence the efficacy of long-term anticoagulation Efficacy & safety of Dabigatran in > 6 months duration is not established. Potential conflicts of interest.
 has not been shown to influence the efficacy of long-term anticoagulation Efficacy & safety of Dabigatran in > 6 months duration is not established. Potential conflicts of interest..")
38
Thank you

Similar presentations