Download presentation
Presentation is loading. Please wait.

1
ANTIBODY MEDIATED REJECTION (HUMORAL REJECTION)
Hadeel Al Mana, MD Consultant Pathologist Department of Pathology and Laboratory Medicine King Faisal Specialist Hospital and Research Centre Riyadh, Kingdom of Saudi Arabia

2
In recent years there has been increasing recognition of the importance of acute antibody- mediated renal allograft rejection There has been a dramatic improvement in the technology of antibody detection. The histologic appearance of acute antibody-mediated rejection (AMR) has been more clearly delineated, following the recognition of the importance of the complement degradation factor C4d as a histologic marker.
 has been more clearly delineated, following the recognition of the importance of the complement degradation factor C4d as a histologic marker.")
3
Protocols incorporating pre- and posttransplant plasmapheresis have shown the feasibility of antibody incompatible transplantation in the setting of ABO blood group mismatch, with satisfactory outcome. protocols have been developed, which permit antibody incompatible (‘positive crossmatch’) kidney transplantation.
 kidney transplantation.")
4
Banff 97 diagnostic categories for renal allograft biopsies – Banff’07 update
1. Normal 2. Antibody-mediated changes (may coincide with categories 3, 4 and 5 and 6) Due to documentation of circulating antidonor antibody, and C4d or allograft pathology C4d deposition without morphologic evidence of active rejection C4d+, presence of circulating antidonor antibodies, no signs of acute or chronic TCMR or ABMR (i.e. g0, cg0, ptc0, no ptc lamination). Cases with simultaneous borderline changes or ATN are considered as indeterminate
 Due to documentation of circulating antidonor antibody, and C4d or allograft pathology. C4d deposition without morphologic evidence of active rejection. C4d+, presence of circulating antidonor antibodies, no signs of acute or chronic TCMR or ABMR (i.e. g0, cg0, ptc0, no ptc lamination). Cases with simultaneous borderline changes or ATN are considered as indeterminate.")
5
Acute antibody-mediated rejection
C4d+, presence of circulating antidonor antibodies, morphologic evidence of acute tissue injury, such as (Type/Grade): I. ATN-like minimal inflammation II. Capillary and or glomerular inflammation (ptc/g > 0) and/or thromboses III. Arterial – v3
: I. ATN-like minimal inflammation. II. Capillary and or glomerular inflammation (ptc/g > 0) and/or thromboses. III. Arterial – v3.")
6
C4d deposition without morphological evidence of active rejection
- Added to the Banff diagnosis under antibody-mediated category. (Banff 07) - The criteria: - presence of C4d in PTC. - lack of histological evidence of acute or chronic rejection ( cellular or humoral). - presence of DSA.
 - The criteria: - presence of C4d in PTC. - lack of histological evidence of acute or chronic rejection ( cellular or humoral). - presence of DSA.")
7
Diagnostic Criteria for Acute Antibody-mediated Rejection (AHR)
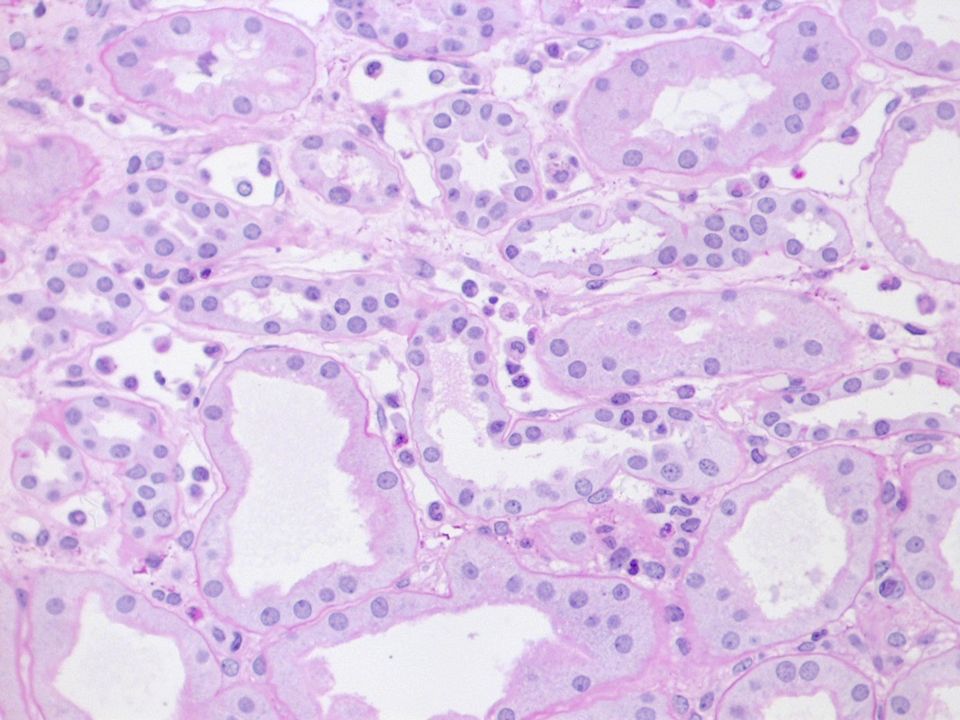
Morphologic evidence of acute tissue injury acute tubular injury neutrophils and/or mononuclear cells in PTC and/or glomeruli and/or capillary thrombosis fibrinoid necrosis/intramural or transmural inflammation in arteries.

11
Antibody-mediated rejection generally has a worse prognosis and requires a different form of therapy than the usual T cell-mediated acute rejection.

12
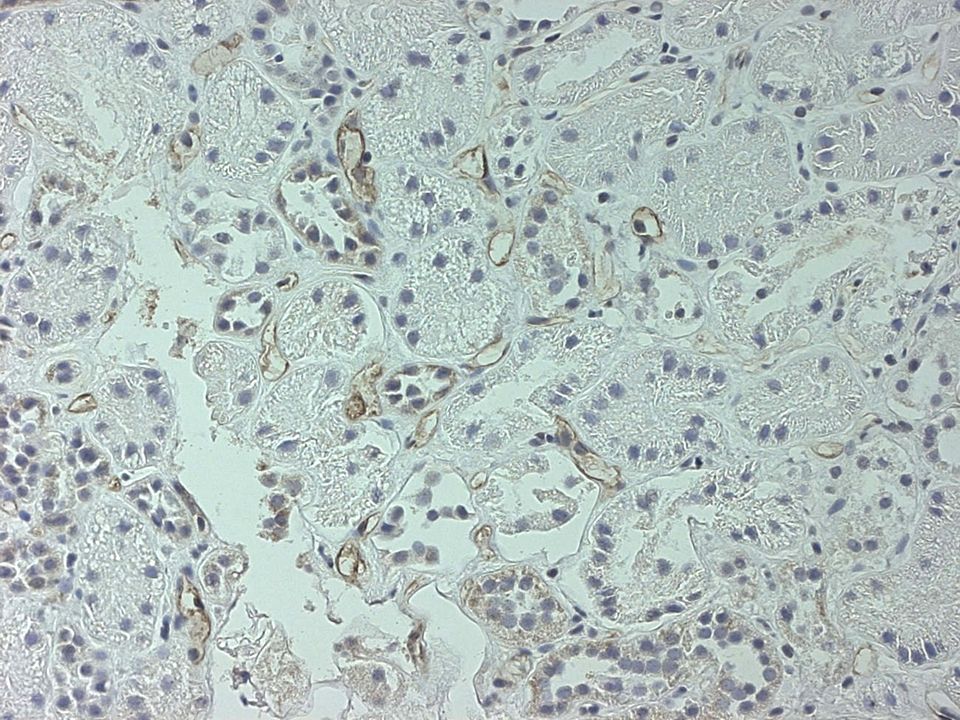
One diagnostic technique (C4d) that permits a definitive diagnosis of antibody-mediated rejection in a renal biopsy. - Peritubular capillary (PTC) C4d deposition in renal transplant biopsies is strongly associated with a poor prognosis and raised the possibility that antibodies were responsible.
 C4d deposition in renal transplant biopsies is strongly associated with a poor prognosis and raised the possibility that antibodies were responsible.")
13
Definition of Positive C4d Staining
The Banff schema defines positive C4d by IF as “widespread, strong linear circumferential PTC staining in cortex or medulla, excluding scar or necrotic areas. (Colvin RB, Nickeleit V: Renal Transplant Pathology. In Heptinstall’s Pathology of the Kidney, 6th Ed., edited by Jennette JC, Olson JL, Schwartz MM, Silva FG, Philadelphia, Lippioncot-Raven, 2006, pp )
")
14
- This pattern has been associated with circulating alloantibodies.
- Many have taken 50% of the capillaries as the threshold.

15
Scoring of C4d Staining (% of biopsy of 5 high-power fields)
C4d 0: Negative: 0% C4d 1: Minimal C4d stain/detection: <10% C4d 2: Focal C4d stain/positive: 10-50% C4d 3: Diffuse C4d stain/positive: >50% American Journal of Transplantation 2008; 8:

20
- Patients with AHR present with an acute loss of graft function that often arises in the first few weeks after transplantation and cannot be distinguished from cell-mediated rejection on clinical grounds. - AHR can also develop years after transplantation, often triggered by a decrease in immunosuppression

21
- Presensitization is the major risk factor, but most of the patients with AHR had a negative cross-match. - AMR occurred with all immunosuppression regimens, even profoundly depleting therapy

22
What to do with Cases with Focally Positive C4d
- Diffuse C4D (50% of PTC) had high rate of graft loss, 1 year later (65%) than those with focal or no C4d (33% graft loss in both cases) (Transplantation 79: , 2005) - The outcome with diffuse or focal C4d was not distinguishable and was worse than those without C4d. (Nephrol Dial Transplant 21: , 2006)
 had high rate of graft loss, 1 year later (65%) than those with focal or no C4d (33% graft loss in both cases) (Transplantation 79: , 2005) - The outcome with diffuse or focal C4d was not distinguishable and was worse than those without C4d. (Nephrol Dial Transplant 21: , 2006)")
23
C4d staining of 25% of the PTC by IHC was associated with decrease 1 year graft survival
(Transplantation 78: , 2004)
")
24
Comparison of C4d techniques
Fixed tissue has a great advantage over IF Glomerular deposits can be assessed, because the normal mesangium does not stain for C4d in fixed tissue but does in frozen.

25
% biopsy area (cortex and/or medulla)
Significance and interpretation according to technique IF IHC % biopsy area (cortex and/or medulla) C4d0 Negative 0% Neg C4d1 Minimal 1<10% Unknown C4d2 Focal 10-50% ? Pos C4d3 Diffuse >50% Pos
 C4d0. Negative. 0% Neg. C4d1. Minimal. 1<10% Unknown. C4d2. Focal % Pos. C4d3. Diffuse. >50% Pos.")
26
Pitfalls in Interpretation
- False negative C4d staining is found in areas of necrosis. - Medulla is adequate for interpretation, because medullary capillaries also are targets of C4d.

28
- Tubules of the medulla maybe confused with capillaries especially in frozen tissue.
- Arterioles not uncommonly have C4d, even in native kidneys with vascular disease.

29
Differential Diagnosis
- C4d deposition in PTC is found in only a few instances of renal disease in native kidneys. - Lupus nephritis may have bright, granular deposits along the PTC, corresponding to the immune complex deposits. - Acute tubular necrosis does not generally show C4d in PTC. - Microangiopathy is negative for C4d in PTC.

30
- Thrombosis of the major renal vessels can lead to graft pathology that resembles AHR; however, no fibrinoid necrosis of arteries or C4d deposition in capillaries occurs. - Glomerular C4d staining is commonly present in glomerular immune complex disease and is not specific.

31
C4d Deposition without Rejection Correlate with Reduced Early Scarring in ABO-Incompatible Renal Allograft In ABO-incompatible grafts peritubular capillary C4d is often present on protocol biopsies lacking histologic features of AMR; the significance of C4d in this setting remains unclear. Data from 33 patients who received ABO-incompatible renal allografts (after desensitization) were retrospectively reviewed. Protocol biopsies were performed at 1 and/or 3 and 6 mo after transplantation in each recipient and at 12 mo in 28 recipients.
 were retrospectively reviewed. Protocol biopsies were performed at 1 and/or 3 and 6 mo after transplantation in each recipient and at 12 mo in 28 recipients.")
32
Twenty-one patients (group A) had strong, diffuse peritubular capillary C4d staining without histologic evidence of AMR or cellular rejection on their initial protocol biopsies. The remaining 12 patients (group B) had negative or weak, focal peritubular capillary C4d staining. Serum creatinine levels were similar in the two groups at 6 and 12 mo after transplantation and at last follow-up.
 had negative or weak, focal peritubular capillary C4d staining. Serum creatinine levels were similar in the two groups at 6 and 12 mo after transplantation and at last follow-up..")
33
Recipients in group A developed significantly fewer overall chronic changes, as scored by the sum of Banff chronic indices, than group B during the first year after transplantation. These results suggest that diffuse peritubular capillary C4d deposition without rejection is associated with a lower risk for scarring in ABO-incompatible renal allografts; the generalizability of these results to conventional allografts remains unknown. J Am Soc Nephrol Jan;20(1):
:")
35
Pathogenesis of AMR AMR results from the interaction of anti-donor antibodies with the allograft vascular endothelium.

36
- AMR results from the interaction of anti-donor antibodies with the allograft vascular endothelium. Under normal circumstances this endothelium plays an important role in maintenance of proper renal function. - Endothelial cells are a major component of the interface between the intravascular and extravascular compartments. Traffic of macromolecules, solutes, plasma proteins and cells between these compartments is tightly regulated, and depends on the integrity of the endothelial cell layer. - The interaction of endothelial cells with high levels of DSA results in complement activation, causing cell death, loss of vascular integrity and subsequent ischemic injury -

37
The intact endothelial surface is negatively charged, in part due to expression of electronegative molecules such as heparan sulfate. This electronegativity serves to repel negatively charged plasma proteins, including albumin and coagulation factors. Exposure to subcytotoxic levels of DSA may result in complement-mediated allograft injury due to endothelial cell activation inducing the formation of intercellular ‘gaps’, shedding of heparan sulfate molecules with loss of cell-surface electronegativity, exposing subendothelial matrix to plasma coagulation factors and platelets and resulting in vascular thrombosis.

38
. In addition to complement-mediated allograft injury, exposure to MHC class I antibodies is capable of inducing apoptosis of vascular endothelium, visible in ultrastructural studies of human allografts experiencing acute AMR. Thus, variable levels of DSA activity may result in allograft injury through a variety of mechanisms, including both complement-dependent and independent pathways resulting in necrosis as well as endothelial cell apoptosis.

39
CHRONIC HUMORAL REJECTION (CHR)
")
40
Diagnostic Criteria for Chronic Antibody-Mediated Rejection (CHR)
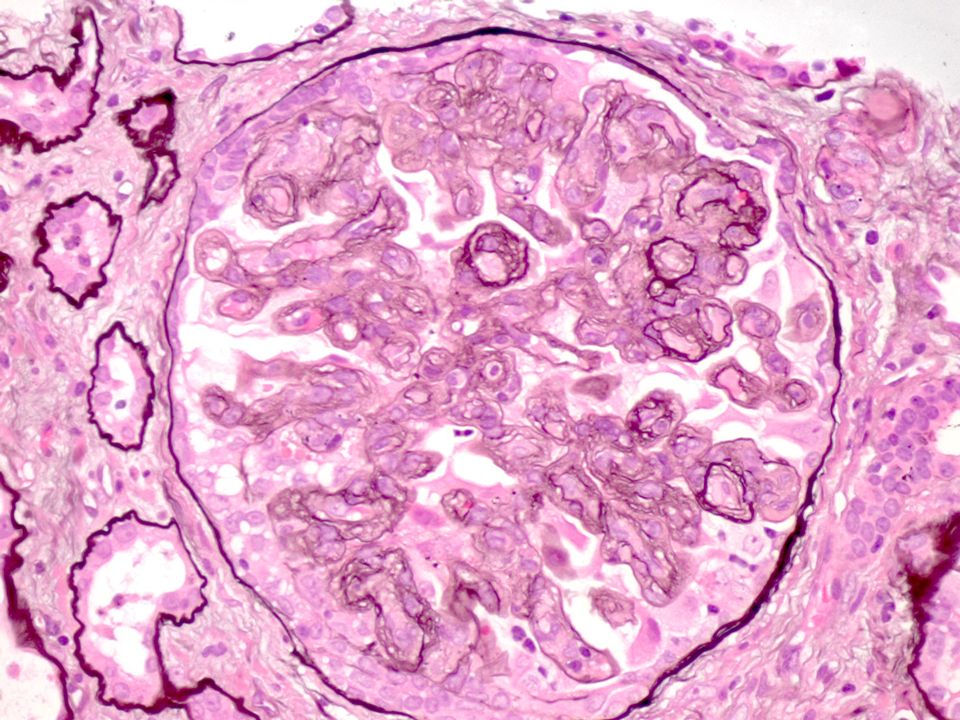
1. Histologic evidence of chronic injury (need 2 of 4) Arterial antimal fibrosis without elastosis. Duplication of glomerular basement membrane Multilaminated PTC basement membrane Interstitial fibrosis with tubular atrophy. 2. Evidence for antibody action/deposition in tissue (e.g. C4d in PTC) 3. Serologic evidence of anti-HLA or other anti-donor antibody
 Arterial antimal fibrosis without elastosis. Duplication of glomerular basement membrane. Multilaminated PTC basement membrane. Interstitial fibrosis with tubular atrophy. 2. Evidence for antibody action/deposition in tissue (e.g. C4d in PTC) 3. Serologic evidence of anti-HLA or other anti-donor antibody.")
41
Association with Circulating DSA
- Several studies agree that C4d is highly sensitive for predicting circulating anti-donor HLA antibodies (88–95%). - Negative DSA results in C4d cases are probably due to absorption in the graft. Non-HLA antibodies and activation of C4 via the lectin pathway may rarely be responsible. - In contrast, circulating DSA is found without detectable C4d deposition in the graft in a more substantial fraction of the cases, ranging from 25 to 50%. In this setting it is possible that the DSA does not fix complement or that the endothelium has become resistant to complement activation by antibody by enhanced complement regulatory proteins or decreased HLA antigen expression.
. - Negative DSA results in C4d cases are probably due to absorption in the graft. Non-HLA antibodies and activation of C4 via the lectin pathway may rarely be responsible. - In contrast, circulating DSA is found without detectable C4d deposition in the graft in a more substantial fraction of the cases, ranging from 25 to 50%. In this setting it is possible that the DSA does not fix complement or that the endothelium has become resistant to complement activation by antibody by enhanced complement regulatory proteins or decreased HLA antigen expression.")
42
- In any case, C4d deposition in peritubular capillaries is specific for acute and chronic rejection, and is not found in other conditions that may affect the allograft, including polyomavirus, calcineurin inhibitor toxicity, thrombotic microangiopathy, recurrent glomerular disease or delayed graft function/acute tubular injury.

43
Circulating Donor Specific Antibodies
DSA pos C4d neg Circulating Donor Specific Antibodies DSA pos C4d pos C4d positivity DSA neg C4d pos

44
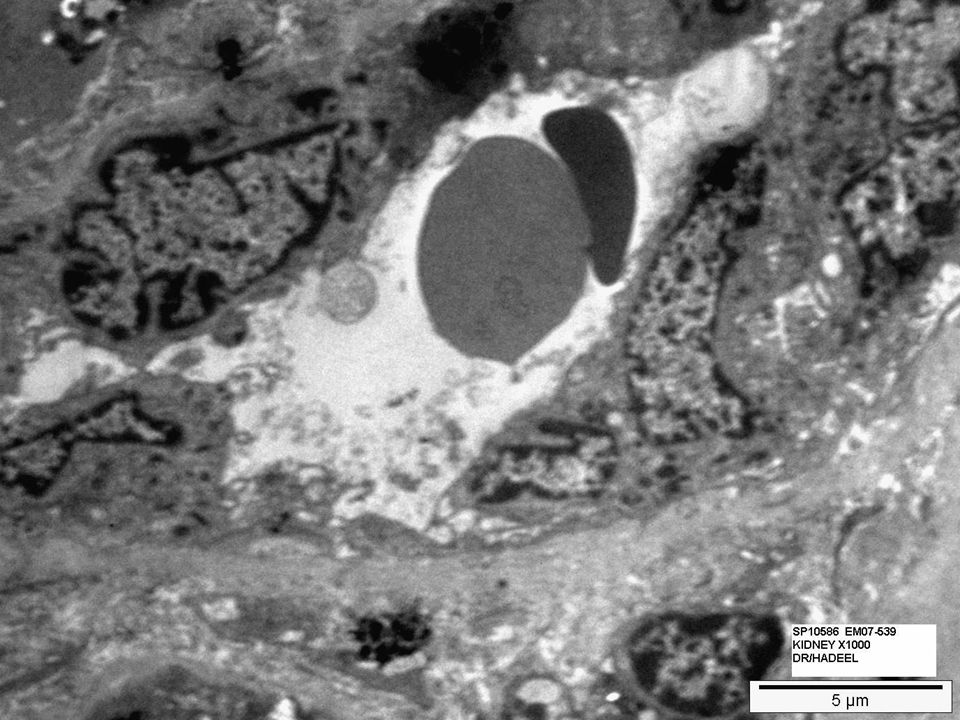
Histology of TG Early clinico-pathologic studies suggested that TG represents the final manifestations of capillary injury. Prior to the GBM remodeling, evidence of acute endothelial cell (EC) injury could be detected, including capillary EC swelling and glomerular hypercellularity. Studies provided evidence of physiologic alterations in glomerular EC in TG that was not present in patients with chronic allograft nephropathy
 injury could be detected, including capillary EC swelling and glomerular hypercellularity. Studies provided evidence of physiologic alterations in glomerular EC in TG that was not present in patients with chronic allograft nephropathy.")
48
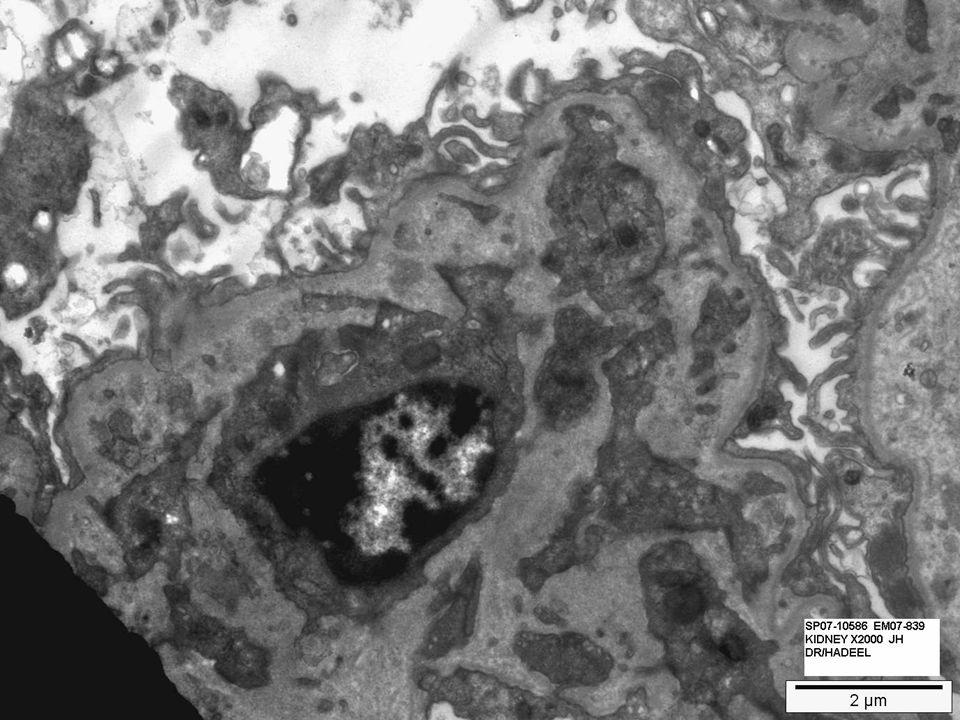
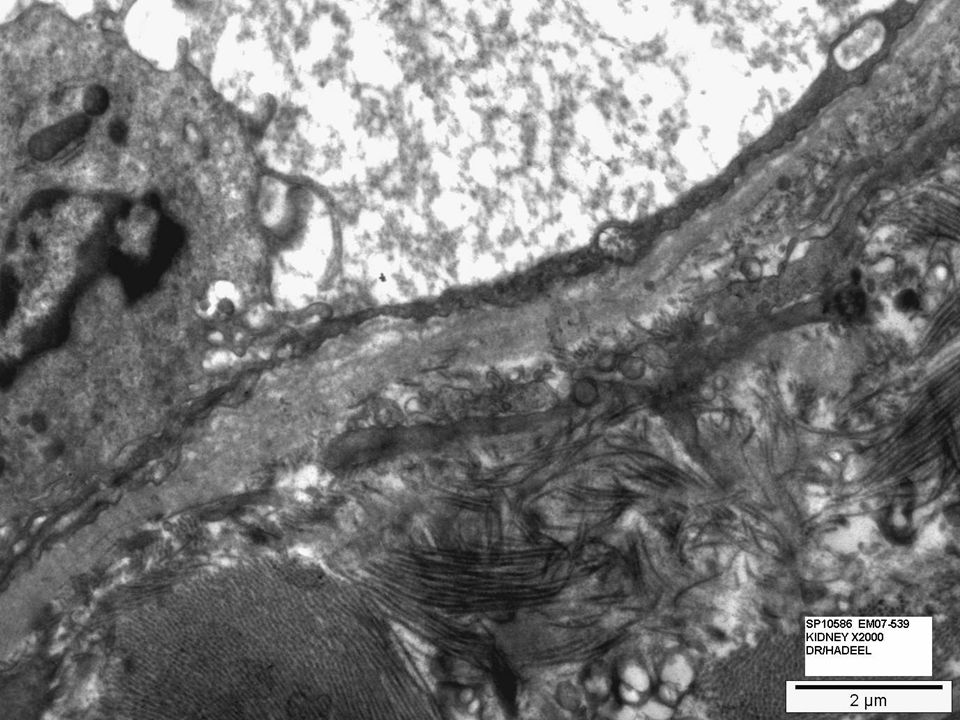
- Electron microscopic (EM) studies demonstrated that the abnormalities of TG are not limited to glomerular capillaries, but also affect peritubular capillaries that show multiple layers of basement membrane . Recent studies showed that this multilamination is present in more than 90% of cases of TG, indicating that this disease is a pancapillaritis of the renal allograft. Am J Transplant 2007; 7: 1743–1752.

52
Until recently, histologic classifications of kidney allograft pathology did not separate TG from ‘chronic allograft nephropathy’. Recent investigations showed that TG, particularly in its early stages, might develop independently from interstitial fibrosis, tubular atrophy and/or transplant arteriopathy. TG is associated with interstitial, peritubular capillary and glomerular inflammation. It is important to note that glomerular inflammation coexists with TG and, in fact, becomes more common and severe as the duplication of the GBM progresses suggesting that TG and its progression is associated with persistent capillaritis. AmJ Transplant 2007; 9: 2124–2132.

53
Antibodies and TG There is strong association between anti-HLA class II antibodies and TG. In several recent studies, it was shown that the presence of anti-HLA antibodies, particularly anti-class II, was associated with poor allograft outcome. Am J Transplant 2007; 7: 864–871, Am J Transplant 2006; 6: 2316–2320. A study showed 26% of patients with pretransplant anti-HLA class II antibodies developed TG compared to 8% of patients without these antibodies. Conversely, of the 55 patients who developed TG, 68% had anti-HLA class II antibodies pretransplant. Furthermore, the risk of TG was also increased in patients with a history of AMR. Thus, approximately 45% of patients with AMR develop TG. Am J Transplant 2007; 7: 1743–1752.

54
Two types of TG: C4d-positive, antibody-mediated and C4d-negative, antibody-independent.
First, it is possible that after an acute antibody-mediated injury, the progression of capillary lesions does not involve complement activation. J Am Soc Nephrol 2002; 13: 2371–2380. The interactions between antibodies and the endothelium are episodic and not continuous, making C4d an inconstant marker. there is evidence that immunoperoxidation is less sensitive than immunofluorescence to detect C4d. J Am Soc Nephrol 2007; 18: 1046–1056.

55
Pathogenesis of TG Anti-HLA (class II) antibodies bind to endothelial cells Antibody (direct) Complement TMA Inflammatory cells Coagulation Changes in endothelial cell phenotype Pan capillaritis/ injury Interstitial inflammation Progressive glomeular injury, capillary obliteration, interstitial fibrosis and tubular atrophy

56
Transplant Capillariopathy
- Studies shown that peritubular capillary basement membranes often show multilamination by electron microscopy, a feature that was later linked rather tightly to C4d deposition. J Am Soc Nephrol 2002;13: 2371. - Graft rejection was manifested by a loss of peritubular capillaries, as judged by loss of class II MHC staining. Transplantation 1989; 48:408–414. - The density of peritubular capillaries (CD34 capillaries/mm2) is highly negatively correlated with renal graft function (fewer capillaries accompany higher the serum creatinine) in late graft biopsies with fibrosis. Transplant Proc 2005;37:981–983.
 is. highly negatively correlated with renal graft function (fewer capillaries accompany higher the serum creatinine) in late graft biopsies with fibrosis. Transplant Proc 2005;37:981–983.")
57
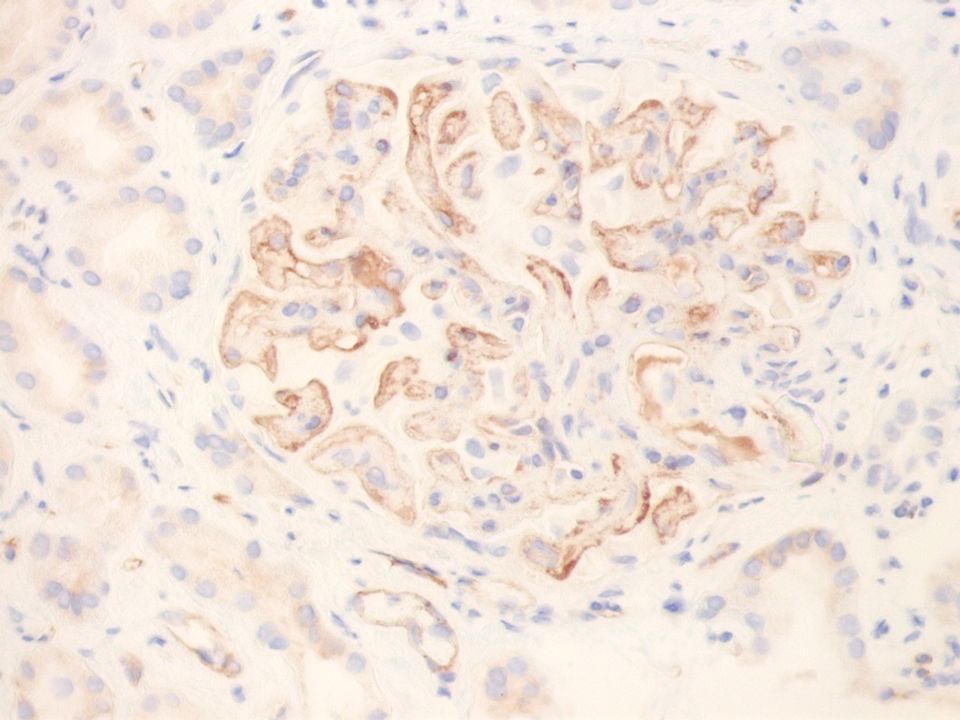
Quantitative studies showed that 43% of the CD34 capillaries were C4d, and the range was 1–89%, with no clear threshold . Am J Transplant 2008;86(suppl):188–189. For CHR, the criteria for C4d need to be lowered, to focal (10–50% of PTC, C4d2) or even perhaps to minimal levels (10% of PTC). In those cases with minimal or no PTC C4d, the glomerular staining may be helpful.
 or even perhaps to minimal levels (10% of PTC). In those cases with minimal or no PTC C4d, the glomerular staining may be helpful.")
58
Transplant Arteriopathy
Transplant arteriopathy in kidney has been less consistently associated with C4d deposition than glomerulopathy . The likely explanation is that antibody plays a less prevalent role in the former than the latter. Indeed, in mouse studies three independent immunologic pathways to arteriopathy have been reported: T cells, NK cells, and antibodies. Thus, both antibody and T-cell-mediated mechanisms can be pathogenic, a possible explanation of why C4d and DSA correlate imperfectly with transplant arteriopathy in humans. Am J Transplant 2007;7:57–65.

59
Time Course and Prognosis CHR
- CHR develops over months to years with typically a slow evolution. Not all features may be seen at any given point, but rather the pathology is cumulative, at least that which is not reversible, such as the basement membrane multilamination. - Stages of CHR in monkey renal allografts in a minority of recipients on a mixed-chimerism tolerance induction protocol, in which all immunosuppression is withdrawn 1 month after transplantation. A minority of these recipients develop DSA and later show C4d in protocol biopsies, followed by interstitial fibrosis and tubular atrophy. These changes may be seen before graft dysfunction is evident. It is quite possible, and indeed a few examples have been observed, in which the antibody and/or the C4d disappears during this course.

60
- Thus the more irreversible features of CHR may be seen (glomerulopathy, fibrosis, PTC lamination) in the absence of the more transient features (C4d, DSA). The monkey studies show a wide variability in the rate of progression from a few months to a few years. All of the monkeys who survived at least a year after the appearance of DSA or C4d deposition developed glomerulopathy, arguing that accommodation to antibodies is not stable. Am J Transplant 2008;8:1662–1672, Am J Transplant 2006;6:1790–1798.

61
Variants of CHR - Cases with interstitial fibrosis and tubular atrophy with C4d deposition, transplant glomerulopathy is not identified. - transplant glomerulopathy with C4d deposition in the glomerulus and not in the peritubular capillaries. - De novo membranous glomerulonephritis.

62
De novo membranous glomerulonephritis is a common form of late posttransplant found in 1–9% of renal allograft biopsies . Studies demonstrate that de novo MGN can arise due to non-MHC antigens in the glomerulus, by showing that renal allografts between MHC identical rat strains developed de novo MGN in the graft but not the native kidney. A study of 17 cases of de novo MGN, 41% had C4d deposition in the peritubular capillaries, a much higher frequency than in other forms of de novo glomerular disease. Peritubular capillary C4d was not detected in any cases of de novo focal glomerulosclerosis or IgA nephropathy. Since de novo MGN is known to arise in MHC matched kidneys, it is likely that this also represents a form of humoral rejection to non-MHC glomerular antigens. The association with C4d may reflect a propensity to form alloantibodies of any type or promotion of an immune response to glomerular antigens secondary to injury mediated by HLA antibodies. This study supports a previously unrecognized relationship between chronic antibody-mediated rejection and de novo MGN. Am J Transplant 2008;86(suppl):35.
:35.")
63
Clinical: graft dysfunction
Chronic Humoral Rejection postulated stages of humoral rejection Clinical: graft dysfunction Graft: pathology Graft: C4d Blood: de novo antibodies Transplant Acommodation Rejection C4d − C4d ₊ subclinical clinical Clinical

64
Pure T cell poor antibody mediated rejection
Cellular rejection Sclerosing rejection Pure T cell poor antibody mediated rejection Capillary transplant vasculopathy Other changes ,e.g. calcineurin inhibitor toxicity etc Normal histology

65
Thank you

Similar presentations















 Histopathologic findings Immunopathologic findings Immunohistochemistry on paraffin sections.>")












