Download presentation
Presentation is loading. Please wait.

1
Obstructive Jaundice Dr. Alex A. Erasmo De Veyra Dee A. Dela Cruz J. Dela Cruz

2
Jaundice in a 58 year old male 2 months PTA 2 months PTA Progressively icteric sclerae Progressively icteric sclerae Tea-colored urine Tea-colored urine Acholic stool Acholic stool 20% weight loss 20% weight loss Pruritus Pruritus

3
Jaundice in a 58 year old male Past Personal History: Past Personal History: Heavy smoker (3 pack-years) Heavy smoker (3 pack-years) Occasional alcoholic beverage drinker Occasional alcoholic beverage drinker No history of hepatitis No history of hepatitis Hypertensive for 10 years Hypertensive for 10 years Captopril Captopril Metoprolol Metoprolol No history of DM No history of DM
 Heavy smoker (3 pack-years) Occasional alcoholic beverage drinker Occasional alcoholic beverage drinker No history of hepatitis No history of hepatitis Hypertensive for 10 years Hypertensive for 10 years Captopril Captopril Metoprolol Metoprolol No history of DM No history of DM")
4
Jaundice in a 58 year old male BP 150/90 HPN? BP 150/90 HPN? PR 86/min PR 86/min Temp 36.7°C Temp 36.7°C RR 17/min RR 17/min Ht: 5’7”; Wt: 155 lbs BMI: 24.3 Ht: 5’7”; Wt: 155 lbs BMI: 24.3 Skin: yellowish Skin: yellowish Icteric sclerae; no palpable cervical lymph nodes; oral cavity normal Icteric sclerae; no palpable cervical lymph nodes; oral cavity normal H/L: essentially normal H/L: essentially normal

5
Jaundice in a 58 year old male Abdomen: Abdomen: Slightly globularAscites? Slightly globularAscites? Ill-defined ballotable mass at the RUQ, not tender, smooth in surface, moves with respiration; Ill-defined ballotable mass at the RUQ, not tender, smooth in surface, moves with respiration; Liver edge not palpable Liver edge not palpable Rectal exam: Rectal exam: Acholic stools Acholic stools

6
http://www.qub.ac.uk/cm/sur/webpages/FinalYear/Jaundice/jaundice.html http://www.qub.ac.uk/cm/sur/webpages/FinalYear/Jaundice/jaundice.html

7
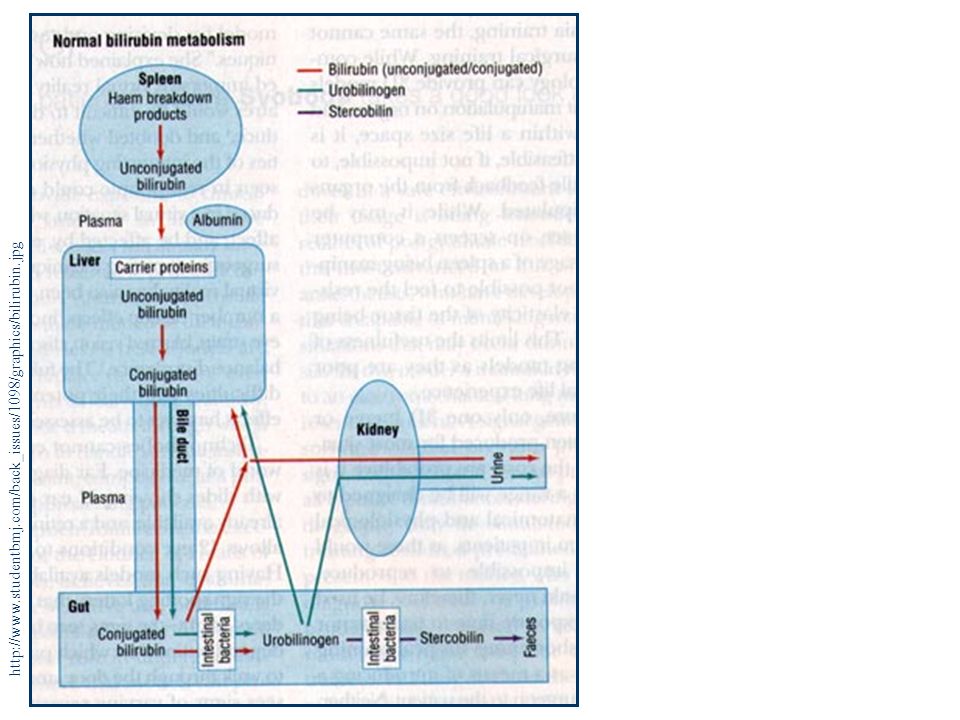
http://www.studentbmj.com/back_issues/1098/graphics/bilirubin.jpg
8
Lab Work-up Hgb: 110 grams Hgb: 110 grams Hct: 35 Hct: 35 WBC: 8000; normal differential count WBC: 8000; normal differential count Platelet: 350,000 Platelet: 350,000 Serum Crea: 1.2 mg Serum Crea: 1.2 mg Total bil: 10 mg; B1(unconj): 2 mg B2 (conj): 8 mg Total bil: 10 mg; B1(unconj): 2 mg B2 (conj): 8 mg Alkaline phosphatase: 500 U/L Alkaline phosphatase: 500 U/L CA 19-9: 350 units/ml CA 19-9: 350 units/ml Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5 Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5
: 2 mg B2 (conj): 8 mg Total bil: 10 mg; B1(unconj): 2 mg B2 (conj): 8 mg Alkaline phosphatase: 500 U/L Alkaline phosphatase: 500 U/L CA 19-9: 350 units/ml CA 19-9: 350 units/ml Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5 Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5")
9
Lab Work-up Hgb: 110 grams Hgb: 110 grams Hct: 35 Hct: 35 WBC: 8000; normal differential count WBC: 8000; normal differential count Platelet: 350,000 Platelet: 350,000 Serum Crea: 1.2 mg Serum Crea: 1.2 mg Total bil: 10 mg; B1(unconj): 2 mg B2 (conj): 8 mg Total bil: 10 mg; B1(unconj): 2 mg B2 (conj): 8 mg Alkaline phosphatase: 500 U/L Alkaline phosphatase: 500 U/L CA 19-9: 350 units/ml CA 19-9: 350 units/ml Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5 Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5
: 2 mg B2 (conj): 8 mg Total bil: 10 mg; B1(unconj): 2 mg B2 (conj): 8 mg Alkaline phosphatase: 500 U/L Alkaline phosphatase: 500 U/L CA 19-9: 350 units/ml CA 19-9: 350 units/ml Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5 Total protein: 6.5 grams; albumin: 3.5; globulin: 2.5")
10
Lab Work-up Significant Elevation of: NV Total Bilirubin 10 mg 0.3 – 1.0 mg/dL B1 2 mg < 0.2 mg/dL B2 8 mg < 0.8 mg/dL Alkaline phosphatase 500 U/L 20-70 U/L CA 19-9 350 U/mL < 37 U/mL

11
Differentiating Jaundice Pre-hepaticIntrahepaticObstructive Plasma Bilirubin B1 B1 both B2 Urine bilirubin Often absent Stercobilin & fecal color , dark /N, pale/N , pale Plasma Alkaline Phosphatase N

12
Differentiating Jaundice Pre-hepaticIntrahepaticObstructive Plasma Bilirubin B1 B1 both B2 Urine bilirubin Often absent Stercobilin & fecal color , dark /N, pale/N , pale Plasma Alkaline Phosphatase N

13
Lab Work-up Others: Others: Prothrombin time Prolonged Prothrombin time Prolonged Serum amylaseElevated Serum amylaseElevated TransaminasesElevated TransaminasesElevated

14
Obstructive Jaundice Gradual obstruction of CBD (weeks or months) JaundicePruritus Without assoc. Sx of biliary colic or cholangitis

15
Differential Diagnosis Painless Jaundice Choledocholithiasis Biliary Obstruction 2 o to malignancy Periampullary Tumors Hilar Cholangiocarcinom a

16
Choledocholithiasis Clinical Picture May be silent May be silent Often discovered incidentally Often discovered incidentally May cause obstruction May cause obstruction Complete Complete Incomplete Incomplete May manifest with cholangitis or gall bladder pancreatitis May manifest with cholangitis or gall bladder pancreatitis

17
PE: may be normal PE: may be normal Mild epigastric or RUQ pain Mild epigastric or RUQ pain Jaundice Jaundice Completely impacted stones: Completely impacted stones: Severe progressive jaundice Severe progressive jaundice Lab Workup Lab Workup serum bilirubin serum bilirubin alkaline phosphatase alkaline phosphatase transaminases transaminases Choledocholithiasis

18
Assoc. with chronic calculous cholecystitis PAIN Assoc. with chronic calculous cholecystitis PAIN Absence of a palpable GB Absence of a palpable GB Courvoisier’s Law Courvoisier’s Law Presence of a palpably enlarged GB suggests biliary obstruction secondary to an underlying malignancy rather than a calculous disease. Presence of a palpably enlarged GB suggests biliary obstruction secondary to an underlying malignancy rather than a calculous disease. Choledocholithiasis

19
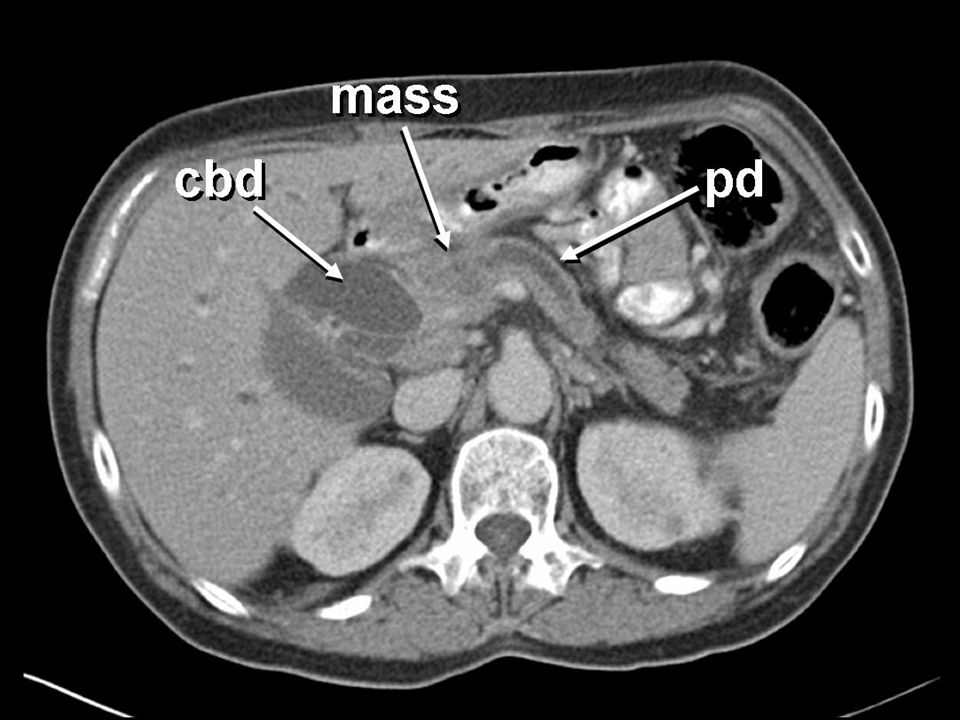
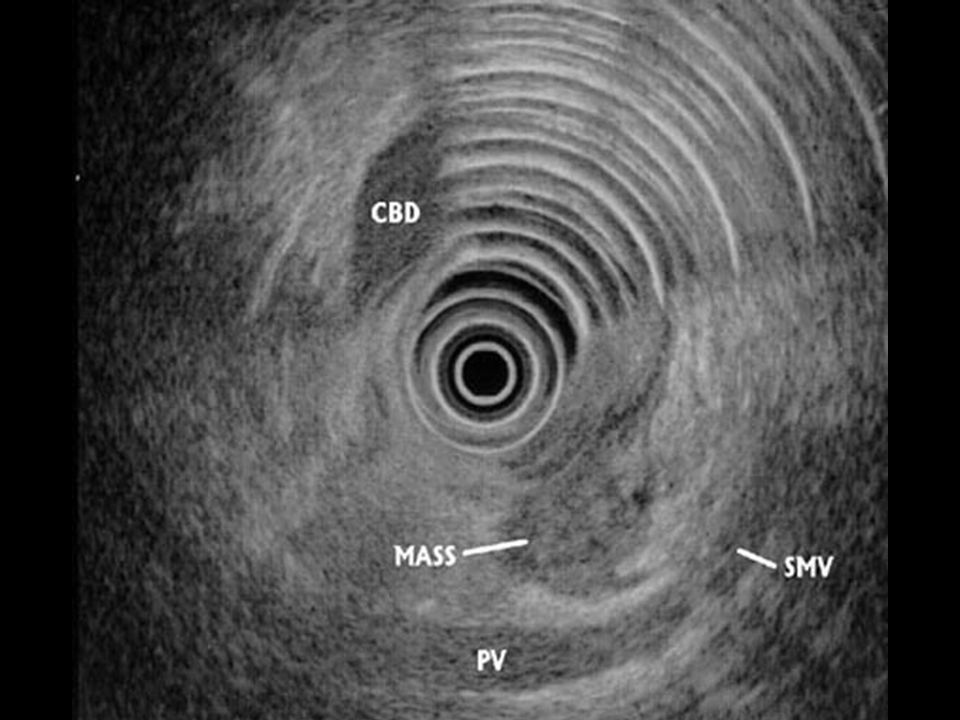
Choledocholithiasis Imaging Studies

20
Differential Diagnosis

21
Ampulla of Vater Ampulla of Vater Distal common bile duct Distal common bile duct Duodenum Duodenum Head of the Pancreas Head of the Pancreas Periampullary Tumors

22
Clinical Picture Painless progressive jaundice Painless progressive jaundice Pruritus Pruritus Acholic stool Acholic stool Tea-colored urine Tea-colored urine Weight loss (Average 10 kg) Weight loss (Average 10 kg) Mild RUQ pain Mild RUQ pain Anorexia Anorexia Fatigue Fatigue
 Weight loss (Average 10 kg) Mild RUQ pain Mild RUQ pain Anorexia Anorexia Fatigue Fatigue")
23
PE is usually normal PE is usually normal Palpable GB (Courvoisier’s Law) Palpable GB (Courvoisier’s Law) Lab Workup Lab Workup alkaline phosphatase alkaline phosphatase total bilirubin & B2 total bilirubin & B2 Periampullary Tumors
 Palpable GB (Courvoisier’s Law) Lab Workup Lab Workup alkaline phosphatase alkaline phosphatase total bilirubin & B2 total bilirubin & B2 Periampullary Tumors")
24
Hilar Cholangiocarcinoma Klatskin’s tumor Klatskin’s tumor Clinical Picture: Painless jaundice Painless jaundice Pruritus Pruritus Mild RUQ pain Mild RUQ pain Anorexia Anorexia Weight loss Weight loss Acholic stools Acholic stools

25
PE is usually normal PE is usually normal Hepatomegaly Hepatomegaly Collapsed GB Collapsed GB Lab Workup Lab Workup alkaline phosphatase alkaline phosphatase gammaglutaryltransferase gammaglutaryltransferase Hilar Cholangiocarcinoma

32
Resectable? YesNo Good risk Poor risk Whipple’s PPPD Endoscopic drainage Bypass Cholecystojejunostomy with Gastrojejunostomy Hepaticojejunostomy with Gastrojejunostomy ERCP Treatment

33
Outcomes in Pancreaticoduodenectomy 1-year mortality rate57% 1-year mortality rate57% 3-year mortality rate26% 3-year mortality rate26% 5-year mortality rate21% 5-year mortality rate21% Median survival rate: 15 months Median survival rate: 15 months 11 5-year survivors 11 5-year survivors 7 6-year survivors 7 6-year survivors 1 15-year survivor 1 15-year survivor

34
Outcomes in Pancreaticoduodenectomy Strongest independent predictors of favorable outcome Strongest independent predictors of favorable outcome Tumor DNA content, Tumor DNA content, Tumor diameter, Tumor diameter, Status of resected lymph nodes, Status of resected lymph nodes, Margin status Margin status Use of postoperative combined modality chemoradiation therapy Use of postoperative combined modality chemoradiation therapy

35
References Brunicardi et. al. Schwartz's Principles of Surgery, 8/e. McGraw-Hill Professional. 2004. Brunicardi et. al. Schwartz's Principles of Surgery, 8/e. McGraw-Hill Professional. 2004. Sabiston et. al. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. W.B. Saunders Co. 2001. Sabiston et. al. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. W.B. Saunders Co. 2001. Greenfield, et. al. Essentials of Surgery: Scientific Principles & Practice. Lippincott-Raven Publishers. 1997 Greenfield, et. al. Essentials of Surgery: Scientific Principles & Practice. Lippincott-Raven Publishers. 1997 American Cancer Society. http://www.cancer.org American Cancer Society. http://www.cancer.org Sosa et. al. Importance of hospital volume in the overall management of pancreatic cancer. Ann Surg. 1998 Sep;228(3):429-38. Sosa et. al. Importance of hospital volume in the overall management of pancreatic cancer. Ann Surg. 1998 Sep;228(3):429-38. Gordon et. al. Statewide regionalization of pancreaticoduodenectomy and its effect on in-hospital mortality. Ann Surg. 1998 Jul;228(1):71-8. Gordon et. al. Statewide regionalization of pancreaticoduodenectomy and its effect on in-hospital mortality. Ann Surg. 1998 Jul;228(1):71-8.
: Sosa et. al. Importance of hospital volume in the overall management of pancreatic cancer. Ann Surg Sep;228(3): Gordon et. al. Statewide regionalization of pancreaticoduodenectomy and its effect on in-hospital mortality. Ann Surg Jul;228(1):71-8. Gordon et. al. Statewide regionalization of pancreaticoduodenectomy and its effect on in-hospital mortality. Ann Surg Jul;228(1):")
36
Body Mass Index (BMI) BMI Weight Status < 18.5 Underweight 18.5 – 24.9 Normal 25.0 – 29.9 Overweight > 30.0 Obese
 BMI Weight Status < 18.5 Underweight 18.5 – 24.9 Normal 25.0 – 29.9 Overweight > 30.0 Obese")
37
Sites of Metastasis in Pancreatic CA (Head) Regional Lymph Nodes 80% Regional Lymph Nodes 80% Juxtaregional Lymph Nodes49% Juxtaregional Lymph Nodes49% Liver75% Liver75% Lungs & Pleura27% Lungs & Pleura27% Adrenals & Stomach14% Adrenals & Stomach14% No metastasis14% No metastasis14%
 Regional Lymph Nodes 80% Regional Lymph Nodes 80% Juxtaregional Lymph Nodes49% Juxtaregional Lymph Nodes49% Liver75% Liver75% Lungs & Pleura27% Lungs & Pleura27% Adrenals & Stomach14% Adrenals & Stomach14% No metastasis14% No metastasis14%")
38
TNM Classification for Staging of Pancreatic CA T Categories of Cancer of the Pancreas T Categories of Cancer of the Pancreas T1: The cancer has not spread beyond the pancreas and is smaller than 2 cm (about ¾ inch). T1: The cancer has not spread beyond the pancreas and is smaller than 2 cm (about ¾ inch). T2: The cancer has not spread beyond the pancreas but is larger than 2 cm (about ¾ inch). T2: The cancer has not spread beyond the pancreas but is larger than 2 cm (about ¾ inch). T3: The cancer has spread from the pancreas to surrounding tissues near the pancreas but not blood vessels. T3: The cancer has spread from the pancreas to surrounding tissues near the pancreas but not blood vessels. T4: The cancer has extended further beyond the pancreas into nearby large blood vessels. T4: The cancer has extended further beyond the pancreas into nearby large blood vessels.
. T2: The cancer has not spread beyond the pancreas but is larger than 2 cm (about ¾ inch). T2: The cancer has not spread beyond the pancreas but is larger than 2 cm (about ¾ inch). T3: The cancer has spread from the pancreas to surrounding tissues near the pancreas but not blood vessels. T3: The cancer has spread from the pancreas to surrounding tissues near the pancreas but not blood vessels. T4: The cancer has extended further beyond the pancreas into nearby large blood vessels. T4: The cancer has extended further beyond the pancreas into nearby large blood vessels..")
39
TNM Classification for Staging of Pancreatic CA N Categories of Cancer of the Pancreas N Categories of Cancer of the Pancreas N0: Regional lymph nodes (lymph nodes near the pancreas) are not involved. N0: Regional lymph nodes (lymph nodes near the pancreas) are not involved. N1: Cancer has spread to regional lymph nodes. N1: Cancer has spread to regional lymph nodes. M Categories of Cancer of the Pancreas M Categories of Cancer of the Pancreas M1: Distant metastasis is present. M1: Distant metastasis is present.
 are not involved. N1: Cancer has spread to regional lymph nodes. N1: Cancer has spread to regional lymph nodes. M Categories of Cancer of the Pancreas M Categories of Cancer of the Pancreas M1: Distant metastasis is present. M1: Distant metastasis is present..")
40
TNM Classification for Staging of Pancreatic CA Stage Grouping for Cancer of the Pancreas Stage Grouping for Cancer of the Pancreas Stage IA (T1, N0, M0): The tumor is confined to the pancreas and is less than 2 cm in size. It has not spread to nearby lymph nodes or distant sites. Stage IA (T1, N0, M0): The tumor is confined to the pancreas and is less than 2 cm in size. It has not spread to nearby lymph nodes or distant sites. Stage IB (T2, N0, M0): The tumor is confined to the pancreas and is larger than 2 cm in size. It has not spread to nearby lymph nodes or distant sites. Stage IB (T2, N0, M0): The tumor is confined to the pancreas and is larger than 2 cm in size. It has not spread to nearby lymph nodes or distant sites. Stage IIA (T3, N0, M0): The tumor is growing outside the pancreas but not into large blood vessels. It has not spread to nearby lymph nodes or distant sites. Stage IIA (T3, N0, M0): The tumor is growing outside the pancreas but not into large blood vessels. It has not spread to nearby lymph nodes or distant sites.
: The tumor is confined to the pancreas and is less than 2 cm in size. It has not spread to nearby lymph nodes or distant sites. Stage IB (T2, N0, M0): The tumor is confined to the pancreas and is larger than 2 cm in size. It has not spread to nearby lymph nodes or distant sites. Stage IB (T2, N0, M0): The tumor is confined to the pancreas and is larger than 2 cm in size. It has not spread to nearby lymph nodes or distant sites. Stage IIA (T3, N0, M0): The tumor is growing outside the pancreas but not into large blood vessels. It has not spread to nearby lymph nodes or distant sites. Stage IIA (T3, N0, M0): The tumor is growing outside the pancreas but not into large blood vessels. It has not spread to nearby lymph nodes or distant sites..")
41
TNM Classification for Staging of Pancreatic CA Stage Grouping for Cancer of the Pancreas Stage Grouping for Cancer of the Pancreas Stage IIB (T1-3, N1, M0): The tumor is either confined to the pancreas or growing outside the pancreas but not into large blood vessels. It has spread to nearby lymph nodes but not distant sites. Stage IIB (T1-3, N1, M0): The tumor is either confined to the pancreas or growing outside the pancreas but not into large blood vessels. It has spread to nearby lymph nodes but not distant sites. Stage III (T4, Any N, M0): The tumor is growing outside the pancreas into large blood vessels. It may or may not have spread to nearby lymph nodes. It has not spread to distant sites. Stage III (T4, Any N, M0): The tumor is growing outside the pancreas into large blood vessels. It may or may not have spread to nearby lymph nodes. It has not spread to distant sites. Stage IV (Any T, Any N, M1): The cancer has spread to distant sites. Stage IV (Any T, Any N, M1): The cancer has spread to distant sites.
: The tumor is either confined to the pancreas or growing outside the pancreas but not into large blood vessels. It has spread to nearby lymph nodes but not distant sites. Stage III (T4, Any N, M0): The tumor is growing outside the pancreas into large blood vessels. It may or may not have spread to nearby lymph nodes. It has not spread to distant sites. Stage III (T4, Any N, M0): The tumor is growing outside the pancreas into large blood vessels. It may or may not have spread to nearby lymph nodes. It has not spread to distant sites. Stage IV (Any T, Any N, M1): The cancer has spread to distant sites. Stage IV (Any T, Any N, M1): The cancer has spread to distant sites..")
42
Symptoms of Pancreatic CA (Head) Weight Loss92% Weight Loss92% Jaundice82% Jaundice82% Pain72% Pain72% Anorexia64% Anorexia64% Dark Urine63% Dark Urine63% Light Stools62% Light Stools62% Nausea45% Nausea45% Vomiting37% Vomiting37% Pruritus24% Pruritus24%
 Weight Loss92% Weight Loss92% Jaundice82% Jaundice82% Pain72% Pain72% Anorexia64% Anorexia64% Dark Urine63% Dark Urine63% Light Stools62% Light Stools62% Nausea45% Nausea45% Vomiting37% Vomiting37% Pruritus24% Pruritus24%")
43
Signs of Pancreatic CA (Head) Jaundice87% Jaundice87% Palpable Liver83% Palpable Liver83% Palpable Gallbladder29% Palpable Gallbladder29% Tenderness26% Tenderness26% Ascites14% Ascites14% Abdominal Mass13% Abdominal Mass13%
 Jaundice87% Jaundice87% Palpable Liver83% Palpable Liver83% Palpable Gallbladder29% Palpable Gallbladder29% Tenderness26% Tenderness26% Ascites14% Ascites14% Abdominal Mass13% Abdominal Mass13%")
Similar presentations
















 FRCS (Glasg) FAMS FACS DNB FICS FAIS.>")






