Download presentation
Presentation is loading. Please wait.

1
Block: URIN 313 Physiology of THE URINARY SYSTEM Lecture 2
Dr. Amel Eassawi

2
GLOMERULAR FILTRATION

3
OBJECTIVES The student should be able to:
Understand the forces involved in forming the glomerular ultrafiltrate and the interaction between them. Define RBF, RPF, GFR, and filtration fraction, and give the normal values for each. Describe the effects of changes in afferent and efferent arteriolar resistances on renal blood flow. Understand the mechanisms involved in the autoregulation of RBF and GFR. Compare and contrast the myogenic and tubuloglomerular feedback (TGF) components in the autoregulatory response. Predict the change in RBF and GFR that would occur with an increase in renal sympathetic nerve activity. Understand the contributions of circulating and locally generated substances on the regulation of RBF and GFR. Identify the component of the filtration barrier whose damage would result in hematuria and proteinuria. Define the filtration coefficient at the glomerular capillary and explain its role in determining GFR.
 components in the autoregulatory response. Predict the change in RBF and GFR that would occur with an increase in renal sympathetic nerve activity. Understand the contributions of circulating and locally generated substances on the regulation of RBF and GFR. Identify the component of the filtration barrier whose damage would result in hematuria and proteinuria. Define the filtration coefficient at the glomerular capillary and explain its role in determining GFR.")
4
Glomerular filtration
Is the first step in urine formation. Glomerular filtration is the transfer of fluid and solutes from the glomerular capillaries into Bowman's capsule due to pressure gradient. When blood passes through glomeruli, blood cells (RBC, WBC, Platelet) and plasma protein are not filtered.
 and plasma protein are not filtered.")
5
GLOMERULAR FILTRATION
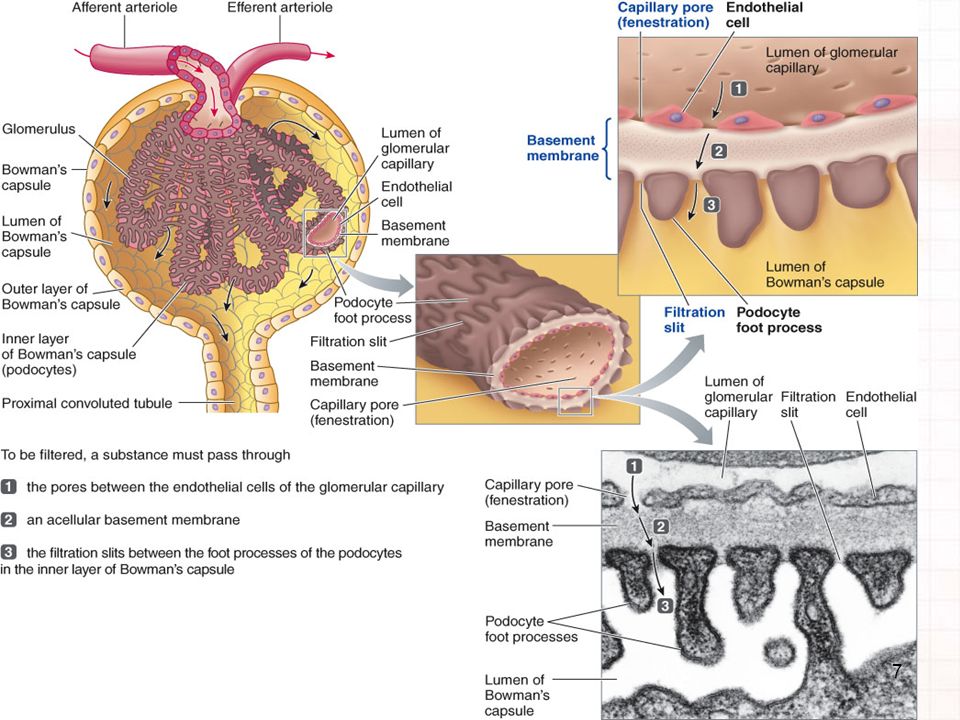
Glomerular Filtration occurs through glomerular membrane. Glomerular membrane has 3 layers: 1. Glomerular capillary endothelial cells 2. Basement membrane 3. Inner layer of Bowman’s capsule – epithelial cells

6
GLOMERULAR FILTRATION
Glomerular membrane is more permeable than capillaries because the glomerular capillary wall has single layer of endothelial cells. It is perforated by many large pores called Fenestrations, that makes it 100 time more permeable to water and solutes than other capillaries in the body. 2. Basement membrane – it does not have cells, but is composed of collagen and glycoprotein. Glycoprotein are negatively charged. 3. Inner layer of Bowman’s capsule – epithelial cells. Epithelial cells are called Podocytes. Each podocyte has foot processes. Narrow silts between adjacent foot processes are known as Filtration silts, they allow the fluid to enter the lumen of Bowman’s capsule.

8
GLOMERULAR FILTRATION
The glomerular filtrate is nearly protein free and contains most inorganic ions and low-molecular-weight organic solutes in virtually the same concentrations as in the plasma. The major barriers of filtration of macromolecules are: molecular size and electrical charge. Negatively charged macromolecules are filtered to a less extent, and positively charged macromolecules to a greater extent, than neutral molecules. Molecular weights less than 7000 daltons are freely filtered. (eg. glucose, urea amino acids and many hormones). The filtration barrier almost totally excludes plasma albumin (molecular weights of approximately 66,000 daltons). Molecular weight is a reference for size, in reality, it is the molecular radius that is critical. Albumin is not filtered due to its negative charge, it is repel by basement membrane negative charges.
. The filtration barrier almost totally excludes plasma albumin (molecular weights of approximately 66,000 daltons). Molecular weight is a reference for size, in reality, it is the molecular radius that is critical. Albumin is not filtered due to its negative charge, it is repel by basement membrane negative charges.")
9
GLOMERULAR FILTRATION
Proteinuria (protein in urine) occur in kidney disease because negative charge on basement membrane are lost, therefore, albumin is filtered and lost in urine.
 occur in kidney disease because negative charge on basement membrane are lost, therefore, albumin is filtered and lost in urine.")
11
GLOMERULAR FILTRATION
Four Forces are involved in glomerular filtration; 1. Glomerular capillary blood pressure - 55mmHg (Favors filtration) (PGC) 2. Plasma Colloid Osmotic Pressure – 30mmHg (Opposes filtration) (πGC) 3. Bowman’s Capsule Hydrostatic – 15mmHg (Opposes filtration) Pressure (PBS) 4. Bowman’s capsular colloidal osmotic pressure (πBC) is Zero (Favors filtration) Net filtration pressure = PGC - (πGC + PBS) Net filtration pressure = 55 – (30+15) = 10 mmHg
 (PGC) 2. Plasma Colloid Osmotic Pressure – 30mmHg (Opposes filtration) (πGC) 3. Bowman’s Capsule Hydrostatic – 15mmHg (Opposes filtration) Pressure (PBS) 4. Bowman’s capsular colloidal osmotic pressure (πBC) is Zero (Favors filtration) Net filtration pressure = PGC - (πGC + PBS) Net filtration pressure = 55 – (30+15) = 10 mmHg.")
12
Figure Summary of forces causing filtration by the glomerular capillaries. The values shown are estimates for healthy humans.

13
GLOMERULAR FILTRATION RATE
GLOMERULAR FILTRATION RATE (GFR) It is the filtrate produced by all the nephrons of both kidneys per minute. Normal young adult male GFR = 125ml/min OR 180 liters/day In female GFR = 115ml/min OR liters/day
 It is the filtrate produced by all the nephrons of both kidneys per minute. Normal young adult male GFR = 125ml/min OR 180 liters/day. In female GFR = 115ml/min OR 160 liters/day.")
14
GLOMERULAR FILTRATION RATE
Glomerular Filtration Rate (GFR) depends on: 1. Filtration Pressure 2. Glomerular Surface Area 3. Permeability of Glomerular Membrane The surface area and permeability are referred to as filtration coefficient (Kf). GFR = Kf × net filtration pressure
 depends on: 1. Filtration Pressure. 2. Glomerular Surface Area. 3. Permeability of Glomerular Membrane. The surface area and permeability are referred to as filtration coefficient (Kf). GFR = Kf × net filtration pressure.")
15
GLOMERULAR FILTRATION RATE
Factors affecting Glomerular Filtration Rate (GFR) 1-Increased Glomerular Capillary Hydrostatic Pressure (PGC) -> increase GFR 2-Increase colloid osmotic Pressure (πGC)-> decrease GFR e.g. Dehydration, Diarrhea 3-Increase Bowman’s capsule Pressure (PBS)->decrease GFR e.g. urinary tract obstruction, enlarged prostrate
 1-Increased Glomerular Capillary Hydrostatic Pressure. (PGC) -> increase GFR. 2-Increase colloid osmotic Pressure (πGC)-> decrease GFR e.g. Dehydration, Diarrhea. 3-Increase Bowman’s capsule Pressure (PBS)->decrease GFR e.g. urinary tract obstruction, enlarged prostrate.")
16
GLOMERULAR FILTRATION RATE
- If afferent arteriole is constricted by epinephrine, norepinephrine, endothelin (increased resistance), blood flow will decrease, therefore, GFR will decrease - If afferent arteriole dilate by Nitric oxide, Prostaglandin(decreased resistance), blood flow will increase, therefore, increase GFR - If efferent arteriole constrict by Angiotensin- II, pressure in glomeruli will increase, therefore, increase GFR
, blood flow will decrease, therefore, GFR will decrease - If afferent arteriole dilate by Nitric oxide, Prostaglandin(decreased resistance), blood flow will increase, therefore, increase GFR - If efferent arteriole constrict by Angiotensin- II, pressure in glomeruli will increase, therefore, increase GFR")
17
Increased blood flow to other organs
Increased resistance in afferent arteriole Decreased resistance in afferent arteriole Decreased capillary blood pressure ( PH) Decreased RBF Decreased GFR (b) ? PH ? GFR ? RBF Afferent arteriole Arterial resistance Efferent arteriole Bowman’s capsule Renal blood flow (RBF) Glomerular filtration rate (GFR) (a) Increased GFR Increased resistance in efferent arteriole (c) Increased PH Glomerulus Flow to other organs
 Decreased RBF. Decreased GFR. (b) PH. GFR. RBF. Afferent arteriole. Arterial resistance. Efferent arteriole. Bowman’s capsule. Renal blood flow (RBF) Glomerular filtration rate (GFR) (a) Increased GFR. Increased resistance in efferent arteriole. (c) Increased PH. Glomerulus. Flow to other organs.")
18
GLOMERULAR FILTRATION RATE
GFR IS AFFECTED BY CHANGES IN FILTRATION COEFFICIENT Filtration coefficient (Kf) depends on glomerulus surface area and permeability of glomerular membrane. Kf can be modified by contractile activity in the glomerular membrane by mesangial cells and Podocytes, foot processes in Bowman capsule (physiological) . Kf can be reduced by pathological process e.g. Diabetes mellitus, Hypertension, Glomerulonephritis If Kf decreased – decreased GFR – in hypertension, diabetes mellitus, GMN, reduced Kf occurs due to increased thickness of glomerular basement membrane and damage to glomeruli.
 depends on glomerulus surface area and permeability of glomerular membrane. Kf can be modified by contractile activity in the glomerular membrane by mesangial cells and Podocytes, foot processes in Bowman capsule (physiological) . Kf can be reduced by pathological process e.g. Diabetes mellitus, Hypertension, Glomerulonephritis. If Kf decreased – decreased GFR – in hypertension, diabetes mellitus, GMN, reduced Kf occurs due to increased thickness of glomerular basement membrane and damage to glomeruli.")
20
Determinants of Renal Blood Flow
Renal blood flow is determined by the pressure gradient across the renal vasculature (the difference between renal artery and renal vein hydrostatic pressures), divided by the total renal vascular resistance: (Renal artery pressure – Renal vein pressure) Total renal vascular resistance Note: Renal artery pressure is about equal to systemic arterial pressure and renal vein pressure averages about 3-4 mmHg under most conditions. A typical Renal blood flow is 1.1 L/min.
, divided by the total renal vascular resistance: (Renal artery pressure – Renal vein pressure) Total renal vascular resistance. Note: Renal artery pressure is about equal to systemic arterial pressure and renal vein pressure averages about 3-4 mmHg under most conditions. A typical Renal blood flow is 1.1 L/min.")
22
RENAL PLASMA FLOW AND FILTRATION FRACTION
Renal blood flow (RBF) is closely related to Renal plasma flow (RPF) which is the volume of blood plasma delivered to the kidneys per unit time. The normal range for RPF is 585 – 605 ml/min. Thus of the 585 – 605 mL of plasma that enters the glomeruli via the afferent arterioles, 125/605, or 20%, filters into Bowman’s space. The remaining 480 mL passes via the efferent arterioles into the peritubular capillaries. This ratio – GFR/RPF – is known as the filtration fraction. Because freely filtered substances are passing into Bowman’s space along with the water, about 20% of all freely filtered substances (eg, sodium) that enter the kidney also move into Bowman’s space.
 is closely related to Renal plasma flow (RPF) which is the volume of blood plasma delivered to the kidneys per unit time. The normal range for RPF is 585 – 605 ml/min. Thus of the 585 – 605 mL of plasma that enters the glomeruli via. the afferent arterioles, 125/605, or 20%, filters into Bowman’s space. The remaining 480 mL passes via the efferent arterioles into the. peritubular capillaries. This ratio – GFR/RPF – is known as the filtration fraction. Because freely filtered substances are passing into Bowman’s space. along with the water, about 20% of all freely filtered substances (eg, sodium) that enter the kidney also move into Bowman’s space.")
23
Figure 19-4 The filtration fraction
>19% of fluid is reabsorbed. Plasma volume entering afferent arteriole = 100% <1% of volume is excreted to external environment. Remainder of nephron Bowman’s capsule Glomerulus >99% of plasma entering kidney returns to systemic circulation. Efferent arteriole Peritubular capillaries Afferent arteriole 20% of volume filters. 80% 1 2 3 4 5

24
GLOMERULAR FILTRATION RATE
Controlled adjustments in GFR Glomerular capillary blood pressure can be controlled to adjust GFR to suit the body’s needs Two major control mechanisms Autoregulation (aimed at preventing spontaneous changes in GFR) Myogenic mechanism Tubuloglomerular feedback (TGF) Extrinsic sympathetic control (aimed at long-term regulation of arterial blood pressure) Mediated by sympathetic nervous system input to afferent arterioles Baroreceptor reflex
 Myogenic mechanism. Tubuloglomerular feedback (TGF) Extrinsic sympathetic control (aimed at long-term regulation of arterial blood pressure) Mediated by sympathetic nervous system input to afferent arterioles. Baroreceptor reflex.")
25
The major function of auto-regulation in the kidneys is to maintain a
Auto regulation of GFR and Renal Blood Flow The major function of auto-regulation in the kidneys is to maintain a relatively constant GFR and to allow precise control of renal excretion of water and solutes. The GFR normally remains auto-regulated, despite considerable arterial pressure fluctuations that occur during usual activities. In general, renal blood flow is auto-regulated in parallel with GFR, but GFR is more efficiently auto-regulated under certain conditions.

26
Myogenic Autoregulation of Renal Blood Flow and GFR
The ability of individual blood vessels to resist stretching during increased arterial pressure. Stretch of the vascular wall allows increased movement of calcium ions from the extracellular fluid into the cells causing them to contract. The contraction prevents over distension of the vessel and at the same time, by raising vascular resistance, helps prevent excessive increases in renal blood flow and GFR when arterial pressure increases.

27
Adjustments of Afferent
Arteriole Caliber to Alter The GFR

28
Figure Autoregulation of renal blood flow and glomerular filtration rate but lack of autoregulation of urine flow during changes in renal arterial pressure. Downloaded from: StudentConsult (on 14 January :45 PM) © 2005 Elsevier
 © 2005 Elsevier.")
29
Tubuloglomerular Feedback Mechanism
Figure Macula densa feedback mechanism for autoregulation of glomerular hydrostatic pressure and glomerular filtration rate (GFR) during decreased renal arterial pressure.
 during decreased renal arterial pressure.")
30
Autoregulation Figure Structure of the juxtaglomerular apparatus, demonstrating its possible feedback role in the control of nephron function. Downloaded from: StudentConsult (on 14 January :45 PM) © 2005 Elsevier
 © 2005 Elsevier.")
31
Baroreceptor Reflex: Influence on the GFR in
Long-term Regulation of Arterial Blood Pressure

32
Other Factors That Increase Renal Blood Flow and GFR: High Protein
Intake and Increased Blood Glucose A high protein meal increases the release of amino acids into the blood, which are reabsorbed in the proximal tubule. Increased amino acid reabsorption also stimulates sodium reabsorption in the proximal tubule. The decrease in sodium delivery to the macula densa. Glucose, like some of the amino acids, is also reabsorbed along with sodium in the proximal tubule, increased glucose delivery to the tubules causes them to reabsorb excess sodium along with glucose.

33
MEASUREMENT OF GLOMERULAR FILTRATION RATE
Renal clearance means that the substance is removed from the blood and excreted in the urine. Substances used to measure GFR 1. Inulin – polymer of fructose, it is filtered, but not reabsorbed, not secreted by renal tubule. 2. Creatinine – it is little secreted, therefore, not so accurate as inulin. Inspite of this clearance of endogenous creatinine is frequently used to measure GFR.

35
REFERENCES Human physiology by Lauralee Sherwood, seventh edition
Text book physiology by Guyton &Hall,11th edition Text book of physiology by Linda .s contanzo, third edition

Similar presentations
















 System>")






