Download presentation
Presentation is loading. Please wait.

1
Assessment of Bowels Grampians Regional Continence Service 102 Ascot Street South Ballarat Health Services – Queen Elizabeth Centre 5320 3795

2
* Bowel action b/w 3/day to 3/week * soft, formed stool * passage of stool without straining * have sensation of rectal fullness and warning prior to passage

3
* Requires several factors: * effective barrier to outflow provided by the internal and external sphincters * a normal rectum that stretches and can hold a good volume of stool and then is able to contract to empty (rectal compliance) * intact anal sensation * bulky and firm (but not hard) stools
 * intact anal sensation * bulky and firm (but not hard) stools")
4
* About 600mls fluid enters colon from small bowel daily, reduced to 150-200 mls of faecal matter * approximate size of a daily bowel action * constant peristaltic action (mixing) * mass movements triggered by reflex (Gastro-Colic Reflex)
 * mass movements triggered by reflex (Gastro-Colic Reflex)")
5
* Stool enters rectum = stretch = sense of fullness & call to stool * When about 150mls in rectum, internal anal sphincter relaxes = passage of stool into anal canal * If not convenient, contract external sphincter (voluntary control) = inhibition of defecation reflex * Stool returns to rectum for later time
 = inhibition of defecation reflex * Stool returns to rectum for later time")
6
* If reflex isn’t inhibited …… * External Sphincter relaxes completely * Pubo-rectalis Muscle relaxes (straightening out ano-rectal angle) * With minimal abdominal effort, rectal contractions expel the stool, aided by gravity
 * With minimal abdominal effort, rectal contractions expel the stool, aided by gravity")
7
* Bowels are an even more difficult and taboo subject than urinary problems * unpleasant for person and staff * People tend to under-estimate the number of bowel movements they have * People have a different definition of constipation to health professionals * Because people use laxatives doesn’t necessarily mean they are constipated

8
* Loss of control of the bowel in an inappropriate time and place * May be leakage of gas, liquid or solid stool

9
* More than the infrequent passage of bowel motions * The definition needs to include: * straining at stool * and/or lumpy or hard stools * and/or feeling of incomplete evacuation * and/or less than 3 bowel movements per week

10
* Prevalence and cost of faecal incontinence * 2010 the number of individuals with urinary or faecal incontinence, living in the community was estimated to be 4,158,101 females (8% of Population) and 1,330,844 Males (3% of population) * In the Residential Aged Care population 70.9% or almost 129,000 residents have urinary or faecal incontinence (or both) * Faecal incontinence is 1 of 3 major causes for admittance to residential aged care * 2010 the total financial cost of incontinence (excluding burden of disease) is estimated to be $42.9 billion, or approx $9,014 per person with incontinence * 2011 Deloitte access economics report
 and 1,330,844 Males (3% of population) * In the Residential Aged Care population 70.9% or almost 129,000 residents have urinary or faecal incontinence (or both) * Faecal incontinence is 1 of 3 major causes for admittance to residential aged care * 2010 the total financial cost of incontinence (excluding burden of disease) is estimated to be $42.9 billion, or approx $9,014 per person with incontinence * 2011 Deloitte access economics report")
11
* The most common digestive problem for GP consultations * Has been shown to decrease quality of life and well-being * Can lead to serious complications such as faecal impaction, incontinence etc

12
* 26% of men and 34% of women over 65 reported constipation * Mostly reported straining, incomplete evacuation, difficulty passing, hard stools * Only 2-3% reported 3 or less BA’s /wk * 30-50% of elderly people regularly use laxatives * >70% of residents used laxatives in BHS study

13
* Individual assessment & management is the key * Initial history is most important part of diagnostic evaluation * Access any past records if appropriate

14
* History & onset of problem * Normal bowel pattern & routines before problem & before admission * How it’s been managed to date * Medical & Surgical History * Medications (including laxatives) * how might the prescribed medicines be likely to affect the bowel?
 * how might the prescribed medicines be likely to affect the bowel")
15
* Functional status * cognition * mobility etc * Dietary and fluid intake * Physical exam by Dr. or R.N. Div 1 * +/- Abdominal X-ray?

16
* Specific Bowel Symptoms * timing of bowel motions * awareness of call to stool/urgency etc * ease of evacuations * stool characteristics * continence status * need to use position or digitally assist emptying * sense of complete or incomplete emptying

17
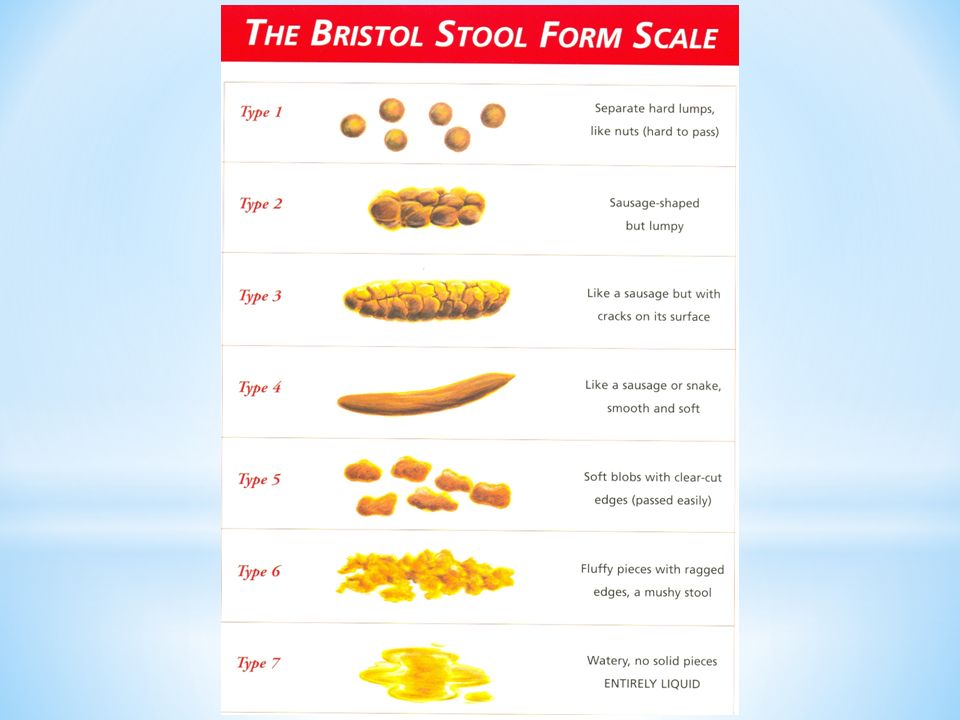
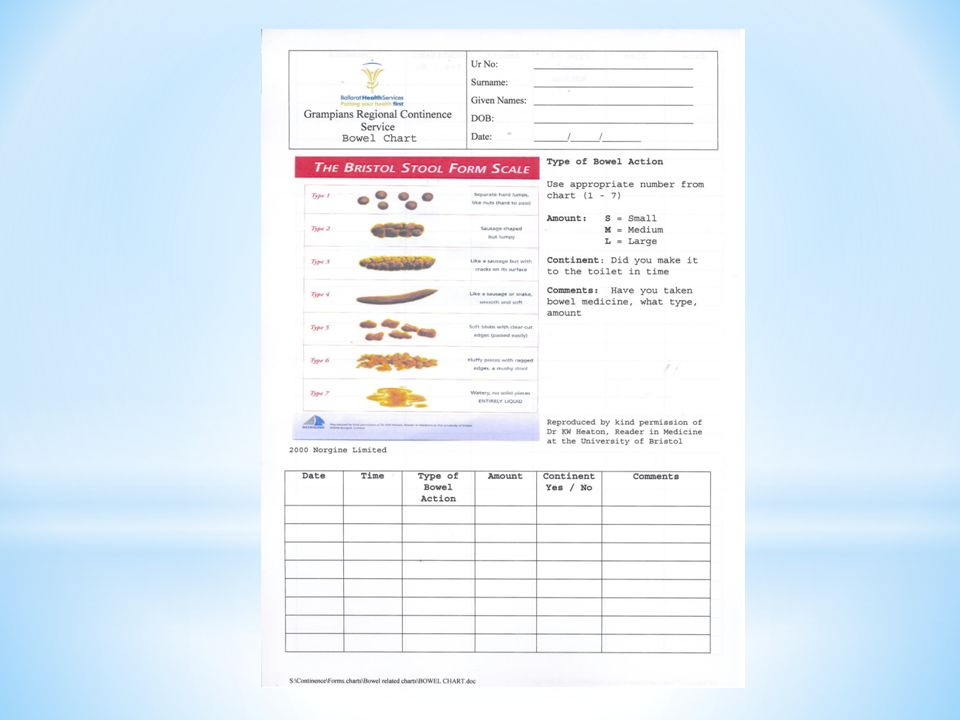
Bowel charting needs to include * Timing of bowel motion * Stool consistency and size * any incontinence - when, what, how much, warning or awareness? * room for comment or observation of factors such as straining, pain, mucous, blood, specific toileting habits * record of anything taken for the bowels

20
* A continuous bowel chart is required if the client is in care * When a problem is identified * an actual constipation or incontinence problem * a person is considered to be at high risk? * When a bowel pattern changes/deteriorates & management needs to be evaluated

21
Thank you. Grampian Regional Continence Service 5320 3795.

Similar presentations






 Adequate, but not excessive, fibre intake.>")







,MRCGP,MRCPE.>")





