Download presentation
Presentation is loading. Please wait.

1
Stroke syndromes of posterior circulations
Done By: Dana Marafie

2
Posterior Circulation

3
Posterior circulation

4
Arteries & structures they supply
PCA: temopral & occipital lobes, parts of thalamus & midbrain SCA: midbrain &superior cerebellum AICA: pons & cerebellum PICA: medulla & cerebellum Basilar: pons , other braches Vertebral: Anterior spinal : upper 2/3 of ant. Surface of spinal cord

5
Specific supply Occipital lobe: PCA
Temporal lobe: MCA (suerpior lateral ) &PCA ( rest) Midbrain: PCA( ant surface), SCA ( post surface) Pons: Basilar ( mainly), AICA Medulla: ant. Spinal , Vertebral & PICA . Small region by ( post spinal) Thalamus: branches from PCA Cerebellum : SCA, AICA & PICA
 &PCA ( rest) Midbrain: PCA( ant surface), SCA ( post surface) Pons: Basilar ( mainly), AICA. Medulla: ant. Spinal , Vertebral & PICA . Small region by ( post spinal) Thalamus: branches from PCA. Cerebellum : SCA, AICA & PICA.")
6
Posterior circulation strokes
Form 20% of all ischemic strokes Mortalility is around 4% except for basilar artery occlusion where it can be up to 90% ! However, outcome is not very good Usually cause bilateral involvement severe headache, vomiting & Nausea are more common in posterior circulation strokes Vertigo, Nystagmus , hemiplagia or quadriplegia, ocular eye movements, ataxia & change in level of consciousness are also seem When to expect Post circulation stroke in a patient? 1- different symptoms & different functions or str. Affected in a way that can not be explained by a cortical region (many tracts or cranial nerves involved)???? 2- when patient is presented with vomiting ,Nystagmus, Nausea, ocular movement disorders or vertigo along with the other symptoms
 2- when patient is presented with vomiting ,Nystagmus, Nausea, ocular movement disorders or vertigo along with the other symptoms.")
7
Arteries & Syndromes! From SUPERIOR TO INFERIOR : PCA Occlusion :
Basilar Artery Occlusion: Locked-in Syndrome Branches; AICA Occlusion : PICA Occlusion : Wallenberg’s Syndrome Vertebral Occlusion : Anterior Spinal Artery Occlusion: These Syndrome can be produced by occlusion of not just mentioned artery but the other arteries as ,long as the same str involved: However, there are commonly seen in case of occlusion of the mentioned artery

8
PCA occlusion Lateral surface Medial surface

9
PCA Occlusion contralateral hemianopia ( with macular sparing)
memory deficit : damage in hippocampal formation (disconnection syndrome ) Bilateral PCA occlusion = Blindness + inability to form new memories
 Bilateral PCA occlusion = Blindness + inability to form new memories.")
10
Left homonymous hemianopia ( with macular sparing)
Picture as seen in Left homonymous hemianopia ( with macular sparing)
")
11
PCA occlusion T1 MRI of PCA infart

12
PCA ( al level of branches to midbrain) (Weber’s syndrome)
at level of midbrain , specifically the BASE X

13
PCA ( al level of branches to midbrain) (Weber’s syndrome)
Manifestations: : at level of midbrain Motor Weakness – contralateral hemiplegia (upper and lower extremity) : Corticospinal tract corticobulbar fibers in the cerebral peduncle Ipsilateral Lateral gaze weakness & diplopia :CN 3 fibers (LMN) PE eye movements: patient is inable to move eye up,down, or medially in the epsilateral side pupillary dilitation: if Edinger-Westphal nucleus are involved
 : Corticospinal tract. corticobulbar fibers in the cerebral peduncle. Ipsilateral Lateral gaze weakness & diplopia :CN 3 fibers (LMN) PE eye movements: patient is inable to move eye up,down, or medially in the epsilateral side. pupillary dilitation: if Edinger-Westphal nucleus are involved.")
14
CASE! A 55 year old African woman had abdominal surgery 2 weeks before suddenly remarking to her husband that she was seeing double. She also felt a weakness in her left arm and leg. Her husband noticed that her right eyelid was drooping. PE: Her general physical condition was good. EYES: : right eyelid does not open fully. right eye was deviated to the right (laterally). When asked to converge the eyes only the left eye adducted showed pupillary constriction ( right is dilated). MOTOR SYSTEM: Motor strength was normal on the right but was reduced on the left, especially in the arm where there was an increased biceps reflex and resistance to passive stretch.
. When asked to converge the eyes only the left eye adducted showed pupillary constriction ( right is dilated). MOTOR SYSTEM: Motor strength was normal on the right but was reduced on the left, especially in the arm where there was an increased biceps reflex and resistance to passive stretch.")
15
Basilar artery occlusion (Locked-in Syndrome)
")
16
Basilar artery occlusion (Locked-in Syndrome)
Manifestation :at the Level of the Pons Weakness of both upper and lower extremity (Quadriplegia): bilateral cortical spinal tracts Weakness of face - entire side :Bilateral corticobulbar tracts If lesion is big,Horizonal gaze weakness: Bilateral fascicles of CN VI ( ONLY vertical gaze is possible!) Dysarthria: Bilateral corticobulbar tracts Death from respiratory failure is common PATEINT are alert, conscoius with normal cognitive fuction IF VERY SEVERE, the only way to communication may be blinking Patient is LOCKED-IN their bodies : Quadriplegic, with dysarthria& facial weekness!
: bilateral cortical spinal tracts. Weakness of face - entire side :Bilateral corticobulbar tracts. If lesion is big,Horizonal gaze weakness: Bilateral fascicles of CN VI ( ONLY vertical gaze is possible!) Dysarthria: Bilateral corticobulbar tracts. Death from respiratory failure is common. PATEINT are alert, conscoius with normal cognitive fuction. IF VERY SEVERE, the only way to communication may be blinking Patient is LOCKED-IN their bodies : Quadriplegic, with dysarthria& facial weekness!")
17
MRI after 19 days in hospital MRA after 19 days in hospital
Locked-in Syndome A 62-year old woman with a history of hypertension for 35 years developed left-sided hemiparesis. One week later she became tetraplegic and unable to speak. However, she was able to communicate by blinking. She died three months after the onset of her neurological symptoms. MRI after 19 days in hospital MRA after 19 days in hospital After autopsy

18
locked-in syndrome A quadriplegic patient with locked-in syndrome who managed to survive ( less severe case)
")
19
Labyrinthine Artery Syndrome
labyrinthine or internal auditory artery usually takes its origin from AICA, but it can also take origin from PICA or the basilar artery. It supplies the inner ear Occlusion of this artery can lead to sudden tinnitus, vertigo or even unilateral ipsilateral deafness !!! Labrinthine Artery

20
PICA Occlusion (Lateral Medullary syndrome Of Wallenberg )
At the level of dorso-lateral part of medulla & Cerebellum

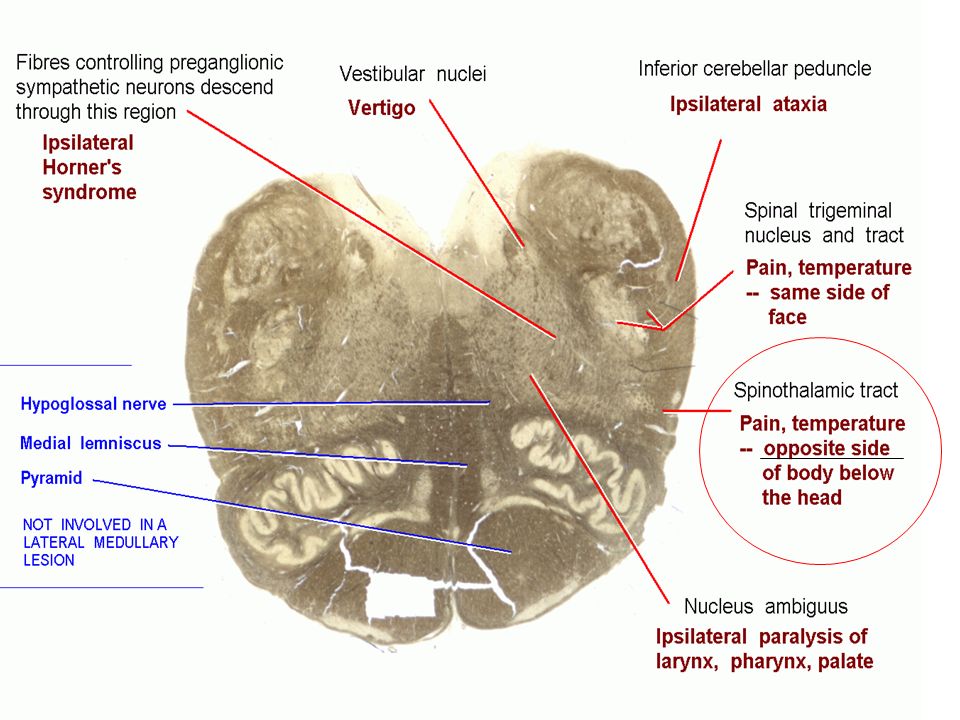
21
PICA Occlusion (Lateral Medullary syndrome Of Wallenberg )
The commonest of brainstem strokes! Manifestation: At the level of dorso-lateral medulla & Cerebellum Ipsilateral Sensory loss of face - pain and Temperature CN 5 spinal N Ipsilateral Facial pain CN 5 spinal N Ipsilateral Ataxia - arm and l Restiform body, Ipsilateral cerebellum Ipsilateral Gait ataxia Restiform body, cerebellum Ipsilateral Nystagmus Vestibular nucleus Ipsilateral Nausea / vomiting Vestibular nucleus Ipsilateral Vertigo Vestibular nucleus Ipsilateral Horseness Nucleus ambiguus Ipsilateral Dysphagia Nucleus ambiguus Ipsilateral Horner syndrome-Descending sympathetics Contralateral Hemisensory loss - pain and Temperature Spinothalamic tract Hiccups ( whatever you do, it does not go !!!) Prognosis is generally quite good with full or near full recovery expected at 6 months.
 Prognosis is generally quite good with full or near full recovery expected at 6 months.")
23
CTscan showing lesion in Medulla & Cerebellum in Wallenberg Syndrome

24
Vertebral artery occlusion
Can also give Wallenberg’s syndrome

25
Thalamic infarction (Dejerine-Roussy syndrome or central pain synrome)
PCA Pentrating branches to thalamus Very sad syndrome Manifestation : pure sensory loss without weakness : due to lesion of (CONTRLATERAL: WHY? Crossing below thalamus) - Hemilateral sensory loss of all modalities - Hemilateral pain ( hypersensitivity) : if you touch their affected side, they will shout ! PCA
 - Hemilateral sensory loss of all modalities. - Hemilateral pain. ( hypersensitivity) : if you touch their affected side, they will shout ! PCA.")
26
MRI of the patient I day after MRI of the patient I day after
After death, autopsy

27
Anterior Spinal Artery Occlusion ( Anterior Spinal Artery syndrome)
Complete sensory & motor loss below the level of occlusion except for proprioception

28
Anterior Spinal Artery syndrome
Manifestations: Loss of motor function below level of damage : due to damage of corticospinal tracts ( ant & post) Bilateral anesthesia ( loss of sensation below the level of damage ) : damage of spinothalamic Loss of bladder & bowel control : damage of descending autonomic tracts; Proprioception is intact due to sparing of dorsal system motor & sensory function in face can be intact
 Bilateral anesthesia ( loss of sensation below the level of damage ) : damage of spinothalamic. Loss of bladder & bowel control : damage of descending autonomic tracts; Proprioception is intact due to sparing of dorsal system. motor & sensory function in face can be intact.")
29
Note Keep in mind that these are not the only syndromes we see in posterior circulation There are many other syndrome that are seen in infartions affecting other regions of brain stem EG of other syndromes of : Midbain :Claude, Benedict ,Nothnagel,Parinaud Syndromes Pons: Millard-Gubler and Raymond-Foville Medulla: Medial medullary syndrome

30
Quiz ! Alia :Overall mortality for posterior circulation strokes is: a. 5% b. 20% c. 40% d. 70% e. 90%

31
Wadha : 1- Locked-in Syndrome consists of: a. Coma with quadriplegia b. Bilateral upper extremity weakness greater than lower extremity weakness c. Quadriplegia, bilateral facial and oropharyngeal palsy but preservation of cortical function and vertical gaze d. Cranial nerve findings contralateral to motor and sensory findings

32
Lastly, Sulaiman :In Weber Syndome:
a .Ipsilatral 3rd nerve palsy & hemiplgia b. Ipsilateral hearing loss c. vertigo, vomiting , ipsilateral ataxia & facial sensory loss & contralateral sensery loss of limbs d.Ipsilatral 3rd nerve palsy & crossed hemiplgia

Similar presentations








 Is it a stroke? (2) What part of the brain is affected? (3) What caused this stroke? Is it a haemorrhage or an infarct? Can.>")
>")

 contains three components: fiber bundles of the corticospinal tracts, pontine nuclei.>")







