Download presentation
Presentation is loading. Please wait.

2
MARS-RERC Machines Assisting Recovery from Stroke Rehabiliation Engineering Research Center on Rehabilitation Robotics & Telemanipulation Funded by:Hosted at: R1: Evaluating Error Augmentation For Neurorehabilitation James Patton, Robert Kenyon, Derek Kamper, Sarah Housman, Ian Sharp, Mark Kovic, Ross Bogey, Borko Jovanovic

3
R1: Evaluating Error Augmentation For Neurorehabilitation Aim 1: Therapist-Driven Trajectories –Therapist specifies the trajectory in real-time –Allows therapist to customize approach, focusing on what is critical for a particular patient’s recovery Aim 2: Patient-Driven Trajectories –Allow subject to provide own desired trajectory –Sensor mounted on healthy limb (bimanual training)
")
4
V irtual R eality R obotics & O ptical O perations M achine

5
Models of learning Hebbian, reinforc-ment, supervised Post- movement adaptation Feedback error learning

6
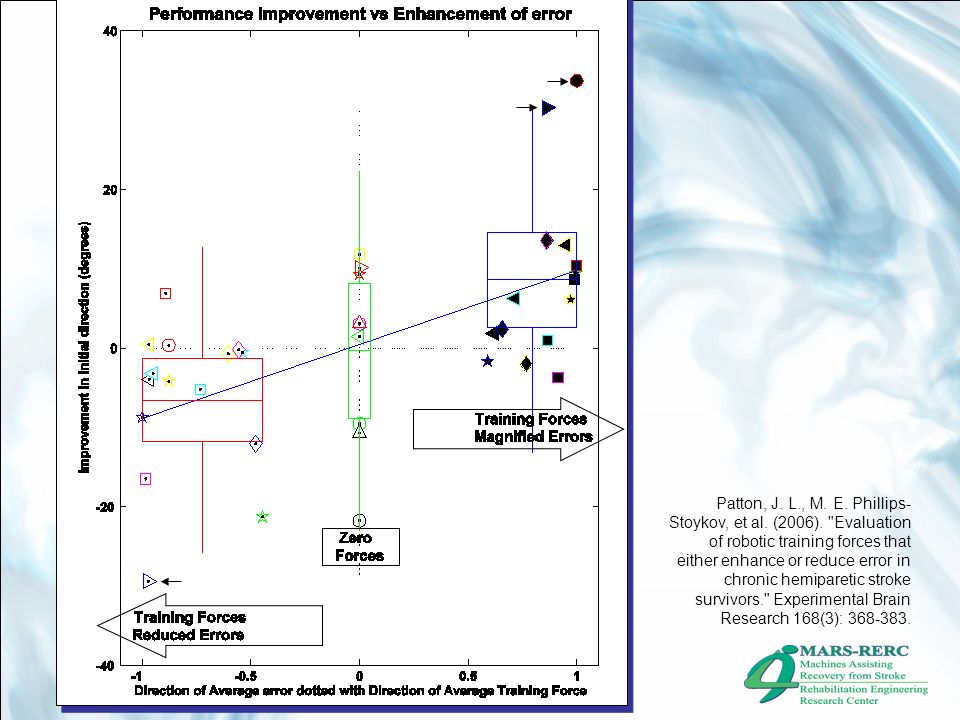
Patton, J. L., M. E. Phillips-Stoykov, et al. (2006). "Evaluation of robotic training forces that either enhance or reduce error in chronic hemiparetic stroke survivors." Experimental Brain Research 168(3): 368-383.
:")
9
EA works in stroke & healthy We have the tools for big study Light forces are all that’s needed For EA, we need to know the “desired” or “intended” location What if the therapist or the patient themselves provide the cue? Visual or force EA? Coupling between hands Background & Motivation

10
Integrate several systems: –Robot –Wrist Clamp –WREX –Hand opening device Software –H3D environment Assessment –Inclusion and exclusion criteria –Clinical tests –Exist questionnaire software Development ``` ` ` ` ` ` ` ` ` `

11
Experiment 1.1 Therapist-Driven Trajectories –Therapist specifies the trajectory in real-time –Allows therapist to customize approach, focusing on what is critical for a particular patient’s recovery 18 subjects, random order of 2 groups : 1.EA therapy 2.Non-EA therapy 4 weeks of treatment Each treatment Lasts 2 weeks Each visit is ~45 min 4 groups EA with visual distortion EA with haptic forces EA with visual distortion and haptics No EA

12
AIM 2 Experiments All Patient-Driven Trajectories Experiment 2.1: Same as Experiment 1, except –Patient-Driven Experiment 2.2: –3 groups Reach simultaneously-bimanually Reach sequentially Control (Free reaching without cues from healthy limb) Experiment 2.3 –3 groups Reach in parallel Reach in mirror Control (Free reaching without cues from healthy limb)
 Experiment 2.3 –3 groups Reach in parallel Reach in mirror Control (Free reaching without cues from healthy limb)")
14
Blinded Rater Assessments pre and post each tx. –“Reach and retrieve” (rag on a stick) –Functional workspace when reaching towards 9 targets on periphery –Wolf Motor Function Test –Box and Blocks –Fugl-Meyer Assessments Figure 3: Schematic example of the directions and layers of the functional workspace determined in the workspace parts of the experiment. x y Theoretical workspace boundary Targets Exten of reaching to targets at different levels
 –Functional workspace when reaching towards 9 targets on periphery –Wolf Motor Function Test –Box and Blocks –Fugl-Meyer Assessments Figure 3: Schematic example of the directions and layers of the functional workspace determined in the workspace parts of the experiment. x y Theoretical workspace boundary Targets Exten of reaching to targets at different levels.")
15
EA haptic forces Figure 11: The double exponential function governing the error-augmentation (dashed line defined in Equation 1. Force F Error F sat sat

16
Secondary assessments: How much time (tx vs. setup)? how long did it take to achieve therapeutically meaningful effect? Which treatment engaged / frustrated patient Therapist opinion

17
Inclusion Criteria Chronic Stroke (8+ mos post) (Changed to 6+ mos in NW IRB) Available medical records/radiographic info Ischemic infarct in MCA (not included in NW IRB) Primary Motor Cortex Involvement (not included in NW IRB) Some degree of shoulder and elbow mvmt. AMFM 40-50 (Changed to 25-50 in NW IRB)
.")
18
Exclusion Criteria Bilateral paresis Severe sensory deficits Severe spasticity (MAS = 4) Severe contracture (added to NW IRB) Aphasia, cognitive impairment or affective dysfunction that would influence the ability to perform experiment Severe concurrent medical problems Diffuse/multiple lesion sites or multiple stroke events Hemispatial neglect/inattention or field cut that would influence the ability to perform experiment Ataxia (added in NW IRB) Significant pain (greater than 5/10) in UE (added in NW IRB) Botox injection in previous 3 months (added in NW IRB) Participation in other UE research projects (added in NW IRB)
 Severe contracture (added to NW IRB) Aphasia, cognitive impairment or affective dysfunction that would influence the ability to perform experiment Severe concurrent medical problems Diffuse/multiple lesion sites or multiple stroke events Hemispatial neglect/inattention or field cut that would influence the ability to perform experiment Ataxia (added in NW IRB) Significant pain (greater than 5/10) in UE (added in NW IRB) Botox injection in previous 3 months (added in NW IRB) Participation in other UE research projects (added in NW IRB)")
19
Statistics Randomized Mixed effects model –Trend affecting the hypothesis on treatment type? –Period-by treatment interaction –Carry over effect –Patient-by-treatment interaction Bayesian? –Early results –Alternative to testing

20
Electronic Visualization Lab at UIC Northwestern University Rehabilitation Institute of Chicago Sensory Motor Performance Program (SMPP) Time Constant of learning (# movements) Error Augmentation speeds up & increases learning in healthy individuals Error Improvement (m) 0.3 0 0.2 0.1 Control *2 *3.1Offset ?
 Time Constant of learning (# movements) Error Augmentation speeds up & increases learning in healthy individuals Error Improvement (m) Control *2 *3.1Offset")
Similar presentations






 Brad Holley, O.T.Reg. (N.B.)>")






>")








 Italy.>")