Download presentation
Presentation is loading. Please wait.

1
Highlights in the Management of Breast Cancer CINBO Consorzio Interuniversitario Nazionale per la Bio-Oncologia “Taxanes vs Anthra-containing chemotherapy in the treatment of early-BC and the issue of cardiac toxicity” Vincenzo Adamo Oncologia Medica e Terapie Integrate A.O.Universitaria, Policlinico “G. Martino” Messina Rome, May 25-26, 2007

2
from Lancet ‘98 to Oxford 2000

3
CMF and node positive Patients G. Bonadonna, BMJ, Jan 2005 Median Follow up 28.5 yrs RFS HR 0.71, p.005 OS HR 0.79, p.04

4
Crown J. Ed. Book, ASCO 2004

5
To need of adjuvant chemotherapy for early breast cancer A superiority of antrhaciclynes based regimens in adjuvant setting EBCTCG OVERVIEW 2005 AND ISSUE SYSTEMIC CHEMOTHERAPY TO CONFIRM The Lancet Vol 365 May 14, 2005

6
Single-Agent Chemotherapy vs Not and Polychemotherapy vs Not from the EBCTCG (2005)
")
7
Anthra vs other regimens 5 yr of recurrence from the EBCTCG (2005)
")
8
Three-drug regimens CAF > CMF ± Tam (INT 0102) CEF > CMF (NCIC-CTG) Sequential regimen E CMF > CMF (NEAT-SCTBG BR9601) Two-drug regimens AC = CMF TAM (NSABP B-15, B-23) EC and hEC = CMF (Belgian trial) Which Anthracycline-based regimen ?
 CEF > CMF (NCIC-CTG) Sequential regimen E CMF > CMF (NEAT-SCTBG BR9601) Two-drug regimens AC = CMF TAM (NSABP B-15, B-23) EC and hEC = CMF (Belgian trial) Which Anthracycline-based regimen")
10
“Taxanes (Paclitaxel and Docetaxel) with significant antitumoral activity in metastatic disease have been evaluated in the adjuvant setting, and their inclusion can further modify the natural history of the disease by reducing the risk of recurrence and death” ROLE OF TAXANES IN ADJUVANT SETTING Buzdar AU, et al. editorial JCO2007

11
First Generation Trials: 31000 pts –Comparing taxane/anthracycline to non-taxane/anthracycline Sequential (anthra followed by taxane) Combination Second Generation Trials: 25000 pts –Comparing taxanes in both arms Sequential Combination With Herceptin ROLE OF TAXANES IN ADJUVANT SETTING Nowak AK et al. Lancet Oncol 5: 372–80, 2004

12
Randomized Trials of Adjuvant Chemotherapy with Taxanes TrialsTreatmentsN° ptsN+/N- (%) NSABP B28 AC(4) >P 225 (4) AC(4) 3068100/0 CALGB 9344 AC(4) >P 175 (4) AC(4) 3121100/0 E2197 A 60 T 60 (4) A 60 C 600 (4) 295835/65 BCIRG 001 TA 50 C (6) FA 50 C (6) 1491100/0 MDACC 94-002 P 250 (4) >FA 50 C (4) FA 50 C (8) 52462/38 PACS01 FE 100 C (3) >T (3) FE 100 C (6) 1999100/0 ECTO A 75 (4) >CMF (4) A 60 P 200 (4) >CMF (4) PST:A 60 P 200 (4) >CMF (4) 1355 (250 PST) NA/NA
 NSABP B28 AC(4) >P 225 (4) AC(4) /0 CALGB 9344 AC(4) >P 175 (4) AC(4) /0 E2197 A 60 T 60 (4) A 60 C 600 (4) /65 BCIRG 001 TA 50 C (6) FA 50 C (6) /0 MDACC P 250 (4) >FA 50 C (4) FA 50 C (8) 52462/38 PACS01 FE 100 C (3) >T (3) FE 100 C (6) /0 ECTO A 75 (4) >CMF (4) A 60 P 200 (4) >CMF (4) PST:A 60 P 200 (4) >CMF (4) 1355 (250 PST) NA/NA")
13
NSABP B28 N= 3060 N+ pts NONE A 60 mg/m 2 C 600 mg/m 2 P 225mg/m 2 (3 h) Mamounas et al JCO 2005 Recommended TAM if HR(+) with chemoRx Median follow-up 64.8-64.4 months
 Mamounas et al JCO 2005 Recommended TAM if HR(+) with chemoRx Median follow-up months")
14
Main G3 toxicityACAC PTX Neurosensory-15% Neuromotor-7% Arthralgia/myalgia-12% granulocytopenia-3% Feb. neutropenia-3% Thromboembolic -event-1% Hypersensitivity reaction -1% Cardiac *1%0.9% AML/MDS°2 cases6 cases Deaths**5 pts2pts *cardiac dysfunction either during or subsequent to therapy °acute myelogenous leukemia ormyelodysplastic syndrome **AC: pulmonary embolism in one, congestive heart failure in two, sepsis in one, and seizure in one; AC and PTX: coronary artery disease in one, pulmonary embolism in one. NSABP B28: Toxicity

15
CALGB 9344 N= 3121 N+ pts NONE A 60= 75= 90 mg/m 2 C 600 mg/m 2 P 175 mg/m 2 (3 h) Recommended TAM if HR(+) after chemoRx Henderson et al JCO 2003 RR:death 18% RR: recurrence 17% RR: death 18% Median follow-up 69.0 months
 Recommended TAM if HR(+) after chemoRx Henderson et al JCO 2003 RR:death 18% RR: recurrence 17% RR: death 18% Median follow-up 69.0 months")
16
CALGB 9344: Toxicity Main toxicityAC(60 mg/mq)AC PTX Granulocytopenia G462%16% Infection17%11% Nausea G2-3-432%3% Vomiting G2-3-427%1% stomatitis G2-3-410%1% Sensory neurotoxicity G3-3% Paresthesias G2-15% Hypersensitivity reaction-6% AML/MDS°9 cases8 cases Deaths1 pts2 pts There was no difference in incidence of cardiotoxicity between those who did and those who did not receive paclitaxel. CHF was observed during active protocol therapy in four (<1%) and six (<1%) pts and during post treatment follow-up in 23 (1%) and 27 (2%) pts randomly assigned to CA alone and CA plus paclitaxel, respectively. °including high dose of Doxorubicin
 and six (<1%) pts and during post treatment follow-up in 23 (1%) and 27 (2%) pts randomly assigned to CA alone and CA plus paclitaxel, respectively. °including high dose of Doxorubicin.")
17
E2197 Trial Goldstein L, PASCO ’05 abs 512

18
E2197: Results I Goldstein L, PASCO ’05 abs 512

19
E2197: Results II Goldstein L, PASCO ’05 abs 512

20
E2197: Toxicity TOXICITYACAT Febrile neutr.6%19% deaths-3 cases AML/MDS7cases Cardiacnr Goldstein L, PASCO ’05 abs 512

21
Adaptated 26° SABCS 2003 BCIRG001

22
BCIRG001: post Chemotherapy Treatment Adaptated 26° SABCS 2003

23
BCIRG001: characteristics of the pts and the tumors Martin M et al N Engl J Med 352; 22, 2, 2005

24
Analysis of Survival Rates in the two Study Groups Martin M et al N Engl J Med 352; 22, 2, 2005

25
Risk Reduction for Disease-free Survival in the Main Subgroups Martin M et al N Engl J Med 352; 22, 2, 2005

26
BCIRG001: toxicity Martin M et al N Engl J Med 352; 22, 2, 2005

27
MDACC TRIAL Buzdar AU, et al. Clinical Cancer Research 2002

28
MDACC TRIAL: Results Buzdar AU et al, Clinical Cancer Research 2002 RFS all pts ER- pts ER+ pts

29
MDACC TRIAL: toxicity Buzdar AU, et al. Clinical Cancer Research 2002

30
PACS-01 SURGERYSURGERY R 6 FEC-100: ARM A Fluorouracil 500 mg/m² d1 Epirubicin 100 mg/m² d1 Cyclophosphamide 500 mg/m² d1 6 cycles every 21 days 3 FEC-100/3 Docetaxel: ARM B 3 cycles of FEC 100 every 21 days followed by 3 cycles of Docetaxel 100 mg/m² d1 every 21 days Radiotherapy delivered within 4 weeks after the last chemotherapy cycle Tamoxifen 20 mg/day for 5 years prescribed in hormone-receptor positive post-menopausal women after chemotherapy Stratified on: Center Age: < or 50 N: 1-3; 4

31
PACS-01:characteristics of pts and tumors Roché H et al J Clin Oncol 2006

32
PACS-01: RESULTS DFSOS Roché H et al J Clin Oncol 2006

33
PACS-01: DFS in different subgroups (Forest plot analysis) Roché H et al J Clin Oncol 2006
 Roché H et al J Clin Oncol 2006")
34
PACS-01: Toxicity Roché H et al J Clin Oncol 2006

35
ECTO Study Gianni L, et al, Clin Cancer Res 2005

36
Patient characteristics and results Gianni L, et al. Clin Cancer Res 2005

37
Main toxicities Gianni L, et al. Clin Cancer Res 2005

38
NCIC CTG MA.21 q 3 w q 2 w q 3 w Burnell M et al. Breast Cancer Res Treat. Abs 53, 2006 Primary end point: relapse free survival (RFS) Secondary end-points: overall survival, toxicity and QoL Pts N+ or N- HRisk
 Secondary end-points: overall survival, toxicity and QoL Pts N+ or N- HRisk.")
39
Regimen courses Schedule Anthracycline TaxaneCyclophosphamide5-FU x cycleTotal CEF 6 q3w 60 mg/m 2 iv D1- D8 720 mgN/A75 mg/m 2 by mouth D1-14 500 mg/m 2 D1 - D8 AC-T 4+4 q3w 60 mg/m 2 iv D1 240 mg 175 mg/m 2 iv D1 600 mg/m 2 iv D1 N/A EC-T(DD) 6+4 q2w 120 mg/m 2 iv D1 720 mg 175 mg/m 2 iv D1 830 mg/m 2 iv D1 N/A CEF = oral cyclophosphamide/epirubicin/5-fluorouracil; AC-T =doxorubicin/cyclophosphamide and paclitaxel; EC-T = epirubicin/cyclophosphamide and paclitaxel; NCIC CTG MA.21: Schedules from medscape : Update on Adjuvant Chemotherapy in BC H McArthur & C Hudis, 2007
 6+4 q2w 120 mg/m 2 iv D1 720 mg 175 mg/m 2 iv D1 830 mg/m 2 iv D1 N/A CEF = oral cyclophosphamide/epirubicin/5-fluorouracil; AC-T =doxorubicin/cyclophosphamide and paclitaxel; EC-T = epirubicin/cyclophosphamide and paclitaxel; NCIC CTG MA.21: Schedules from medscape : Update on Adjuvant Chemotherapy in BC H McArthur & C Hudis, 2007")
40
RegimenHazard Ratio (95% CI)P Value EC-T to CEF0.89 (0.64, 1.22).46 AC-T to CEF1.49 (1.12, 1.99).005 AC-T to EC-T1.68 (1.25, 2.27).0006 NCIC CTG MA.21: Results 2104 patients enrolled Dec-2000-April 2005 RegimenRecurrence free survivalFw-up CEF90.1 %3 years AC-T89.5%3 years EC-T85.0%3 years global test of significance
P Value EC-T to CEF0.89 (0.64, 1.22).46 AC-T to CEF1.49 (1.12, 1.99).005 AC-T to EC-T1.68 (1.25, 2.27).0006 NCIC CTG MA.21: Results 2104 patients enrolled Dec-2000-April 2005 RegimenRecurrence free survivalFw-up CEF90.1 %3 years AC-T89.5%3 years EC-T85.0%3 years global test of significance")
41
NCIC CTG MA.21 However, both the CEF and dose-dense EC-T regimens were associated with increased rates of febrile neutropenia,TVE, and delayed cardiotoxicity compared with AC-T. Toxicity Febrile Neutropenia Cardiac disfunction CEF22.9%36.9% EC-T16.7%28.7% AC-T4.8%21.9%

42
Randomized Trials of Adjuvant Chemotherapy with Taxanes TrialsTreatmentsN° ptsN+/N- (%) 5Y-DFS (%) 5Y-OS (%) NSABP B28 AC(4) >P 225 (4) AC(4) 3068100/076/72 p=0.006 85/85 p=0.46 CALGB 9344 AC(4) >P 175 (4) AC(4) 3121100/070/65 P=0.0023 80/77 P=0.0064 E2197 A 60 T 60 (4) A 60 C 600 (4) 295835/6587/87 p=0.70* 94/93 p=0.49* BCIRG 001 TA 50 C (6) FA 50 C (6) 1491100/075/68 p=0.001 87/81 p=0.008 MDACC 94-002 P 250 (4) >FA 50 C (4) FA 50 C (8) 52462/3886/83 p=0.09* NA PACS01 FE 100 C (3) >T (3) FE 100 C (6) 1999100/078.3/73.2 p=0.041 90.7/86.7 p=0.05 ECTO A 75 (4) >CMF (4) A 60 P 200 (4) >CMF (4) PST:A 60 P 200 (4)>CMF(4) 1355 (250 PST) NA/NAHR=0.66 p=0.012*NSD * parameter after 4 years of follow up
 5Y-DFS (%) 5Y-OS (%) NSABP B28 AC(4) >P 225 (4) AC(4) /076/72 p= /85 p=0.46 CALGB 9344 AC(4) >P 175 (4) AC(4) /070/65 P= /77 P= E2197 A 60 T 60 (4) A 60 C 600 (4) /6587/87 p=0.70* 94/93 p=0.49* BCIRG 001 TA 50 C (6) FA 50 C (6) /075/68 p= /81 p=0.008 MDACC P 250 (4) >FA 50 C (4) FA 50 C (8) 52462/3886/83 p=0.09* NA PACS01 FE 100 C (3) >T (3) FE 100 C (6) /078.3/73.2 p= /86.7 p=0.05 ECTO A 75 (4) >CMF (4) A 60 P 200 (4) >CMF (4) PST:A 60 P 200 (4)>CMF(4) 1355 (250 PST) NA/NAHR=0.66 p=0.012*NSD * parameter after 4 years of follow up")
43
Cardiac Toxicity TrialsTreatmentsCardiac toxicity NSABP B28 AC(4) >P 225 (4) AC(4) Cardiac disfunction G3 (during and posttreatment) 0.9% 1% CALGB 9344 AC(4) >P 175 (4) AC(4) CHF <1% (during treat.); 2% (posttreat.) <1% (during treat.); 1% (posttreat.) E2197 A 60 T 60 (4) vs A 60 C 600 (4) NR BCIRG 001 TA 50 C (6) FA 50 C (6) Mild to severe CHF G3-4 1.6% 0.1% 0.7% 0.1% MDACC 94-002 P 250 (4) >FA 50 C (4) FA 50 C (8) Transient arrhyt. CHF 3% 0% 5% 1% PACS 01 FE 100 C (3) >T (3) FE 100 C (6) Any events CHF LEVF>20% end CT LEVF>20% \ after 1y 0.4% 0% 6.5% 7.8% 1.3% 0.4% 7.0% 10% ECTO A 75 (4) >CMF (4) A 60 P 200 (4) >CMF (4) PST:A 60 P 200 (4)>CMF(4) CTC 1 CTC 2 CTC 3 LEVF 20% 67.8% 13.6% 0.5% 8.0% 5.6% 70.8% 11.1% 0.4% 5.7% 5.4% P=0.09P=1.0 P=.03P=.63P=.09 During and posttreat
 >T (3) FE 100 C (6) Any events CHF LEVF>20% end CT LEVF>20% \ after 1y 0.4% 0% 6.5% 7.8% 1.3% 0.4% 7.0% 10% ECTO A 75 (4) >CMF (4) A 60 P 200 (4) >CMF (4) PST:A 60 P 200 (4)>CMF(4) CTC 1 CTC 2 CTC 3 LEVF 20% 67.8% 13.6% 0.5% 8.0% 5.6% 70.8% 11.1% 0.4% 5.7% 5.4% P=0.09P=1.0 P=.03P=.63P=.09 During and posttreat.")
44
Comments Cardiac toxicity data are controversial: most of the trials don’t include a careful cardiac monitoring before, during and after the treatments Many trials demostrate that Anthracyclines and Taxanes are the most active cytotoxic drugs for the treatment of breast cancer also as adjuvant chemotherapy. However the advantages obtained by this combination must be carefully balanced against potential risks, particularly in the adjuvant setting.

45
Mechanisms and types of Cardiotoxicity Associated with different therapeutic modalities by Brian R, et al, Ed Boock ASCO 2007

46
Who need Adjuvant Chemotherapy ?

47
Adjuvant Chemotherapy Options Trastuzumab if HER-2 positive adapted from Piccart et al. (2005)
")
48
Anthracyclines may not be necessary in adjuvant therapy of breast cancer ?

49
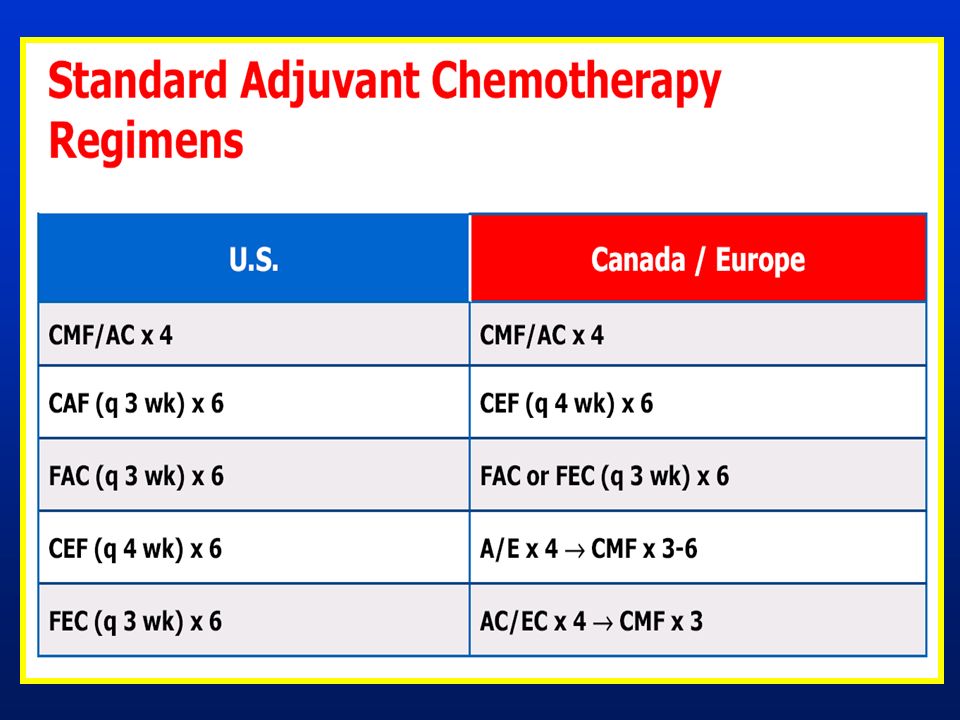
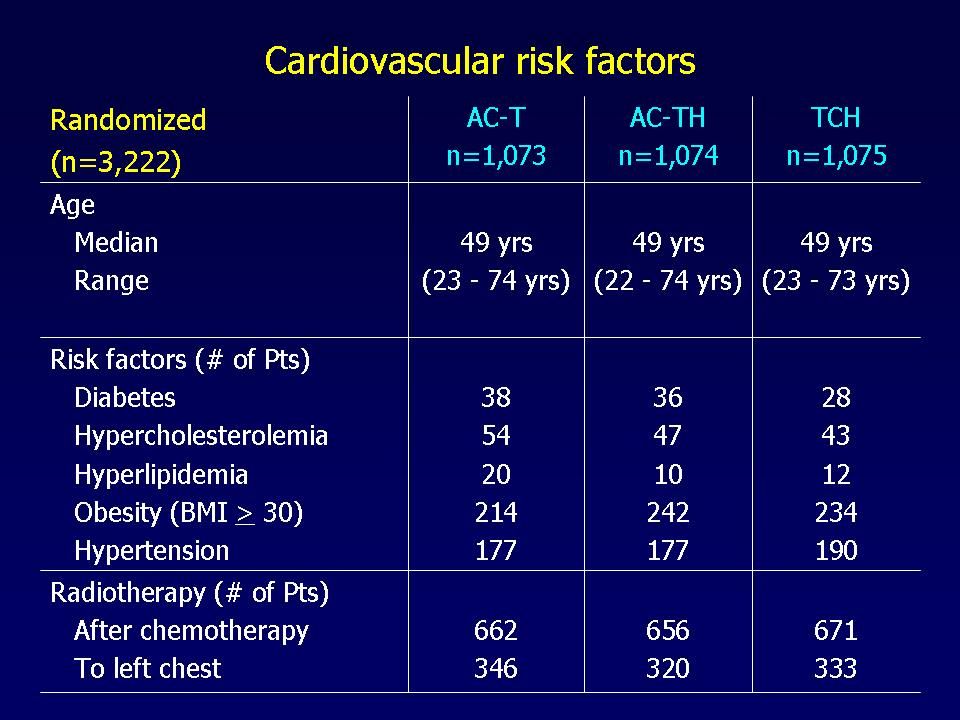
Slamon SABCS 2006

50
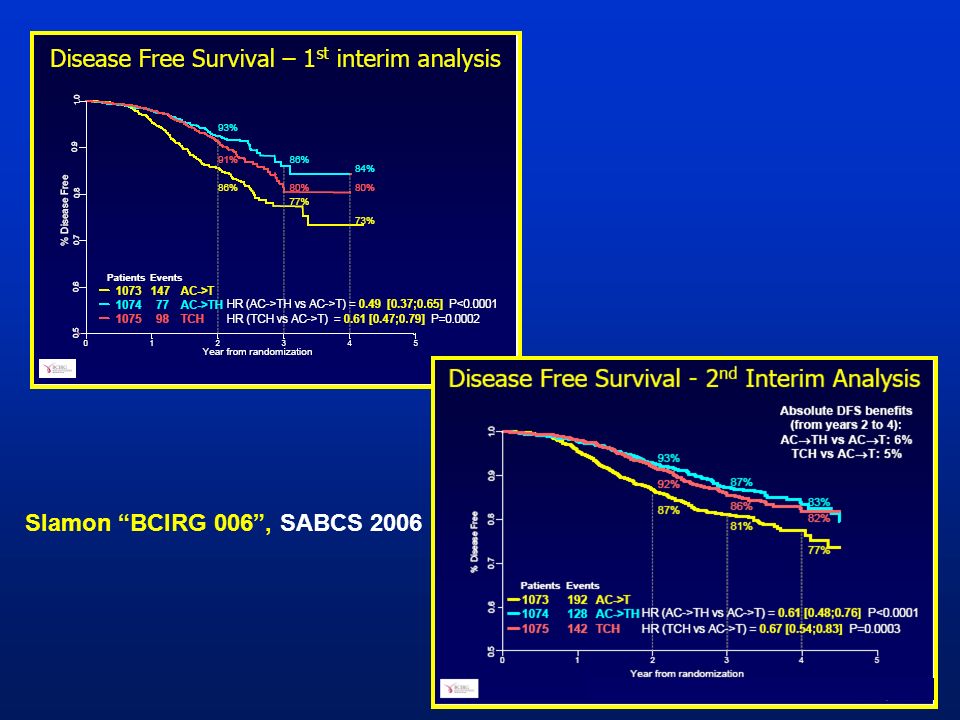
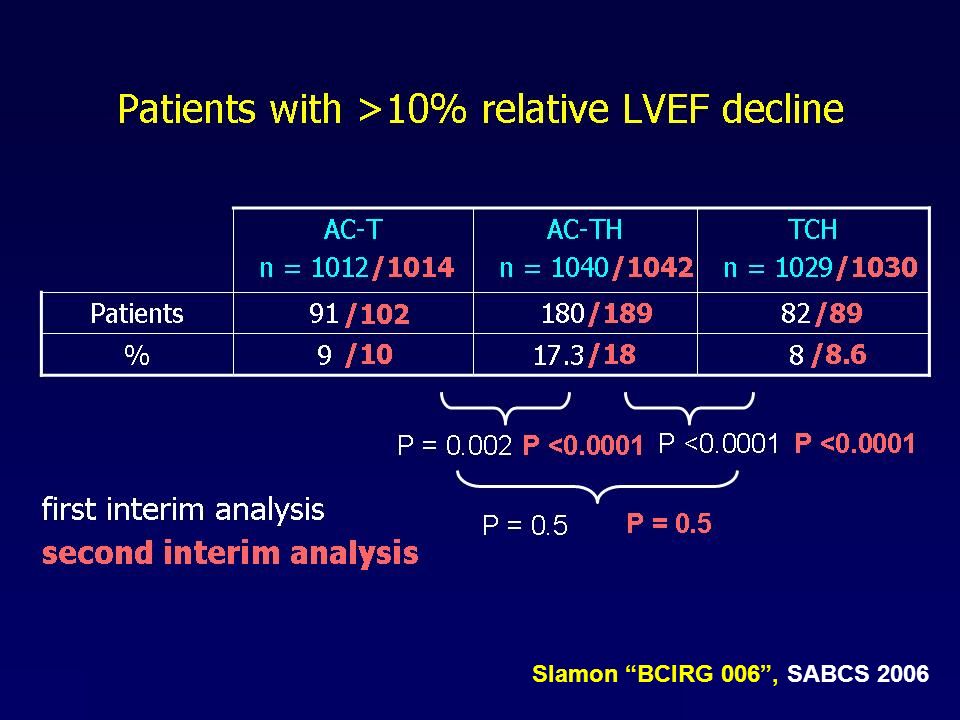
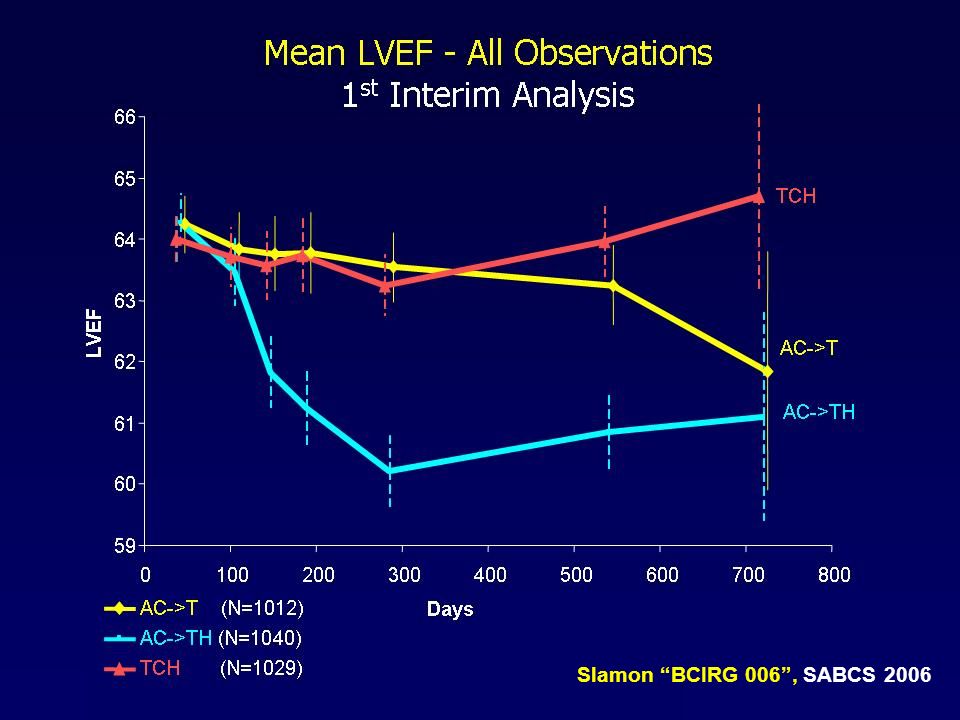
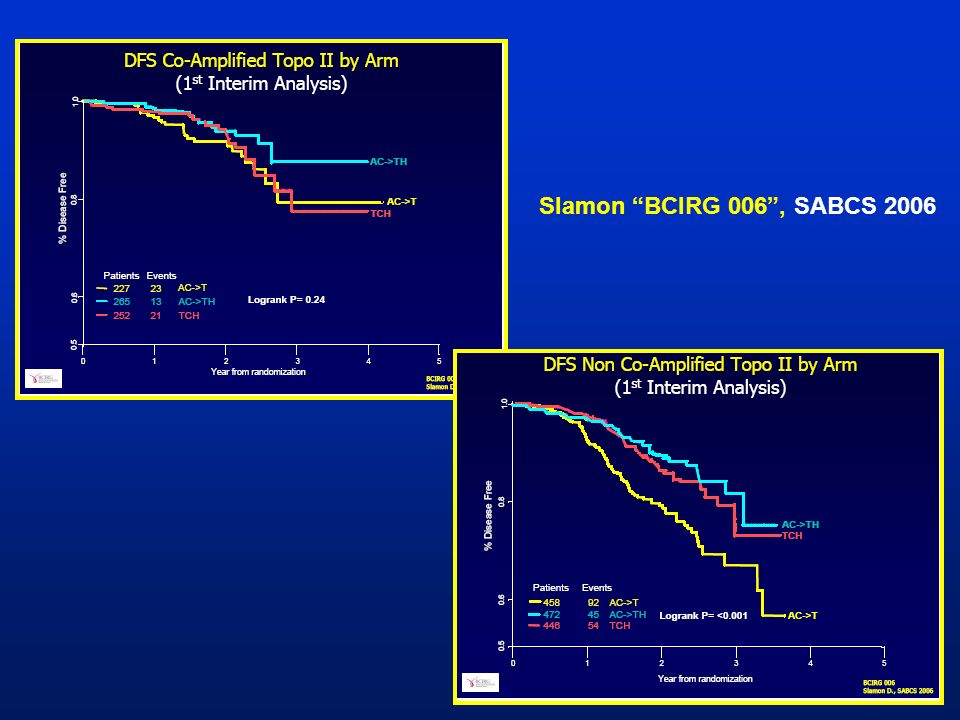
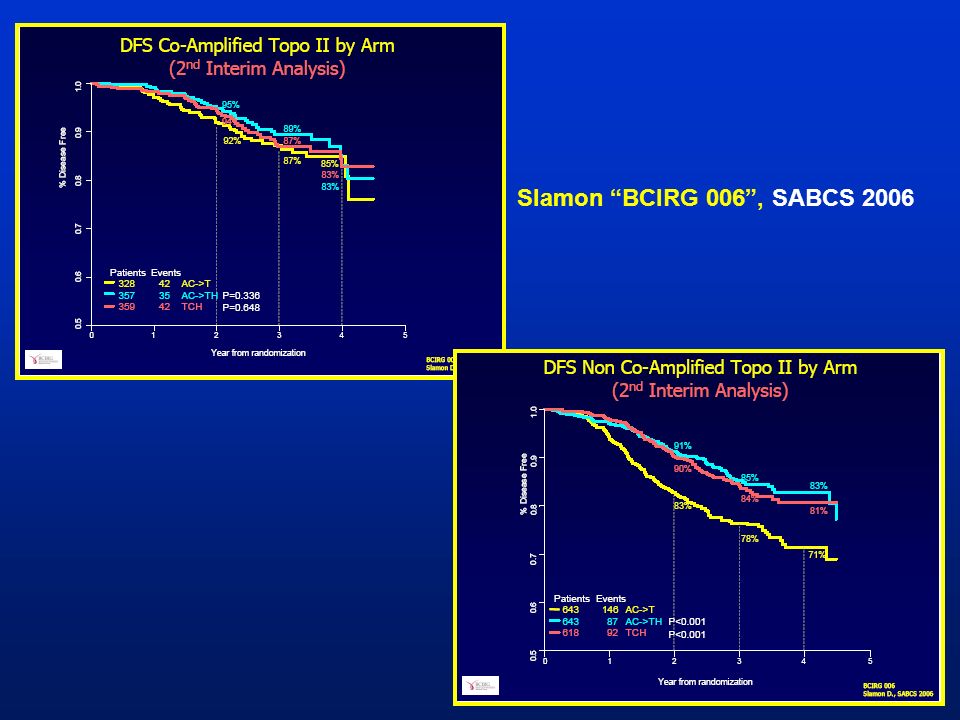
Slamon “BCIRG 006”, SABCS 2006

60
“BCIRG 006”, SABCS 2006

61
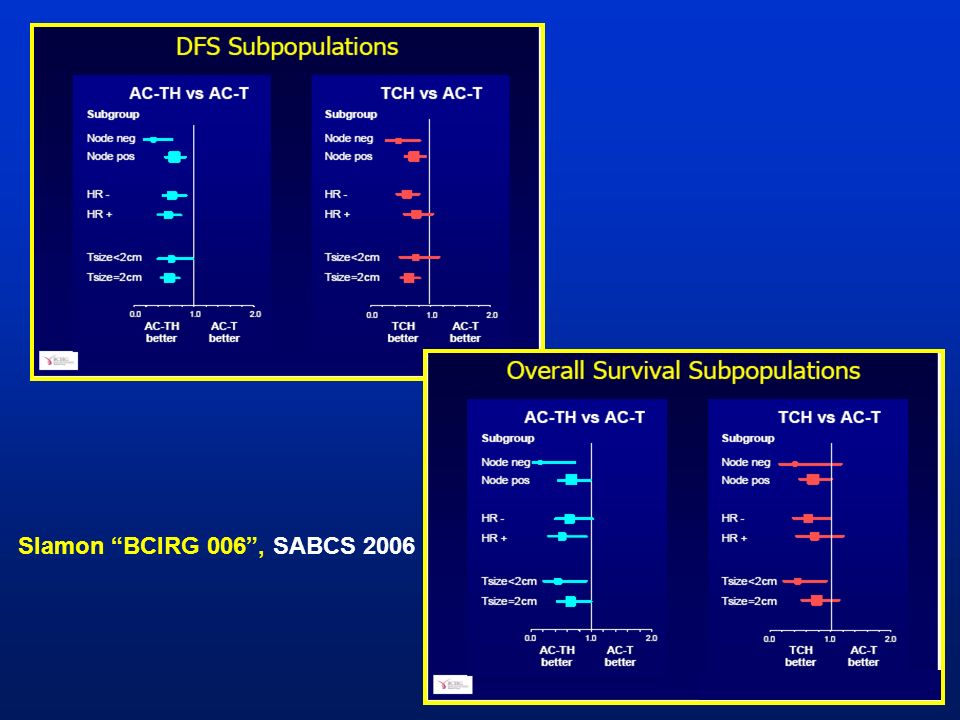
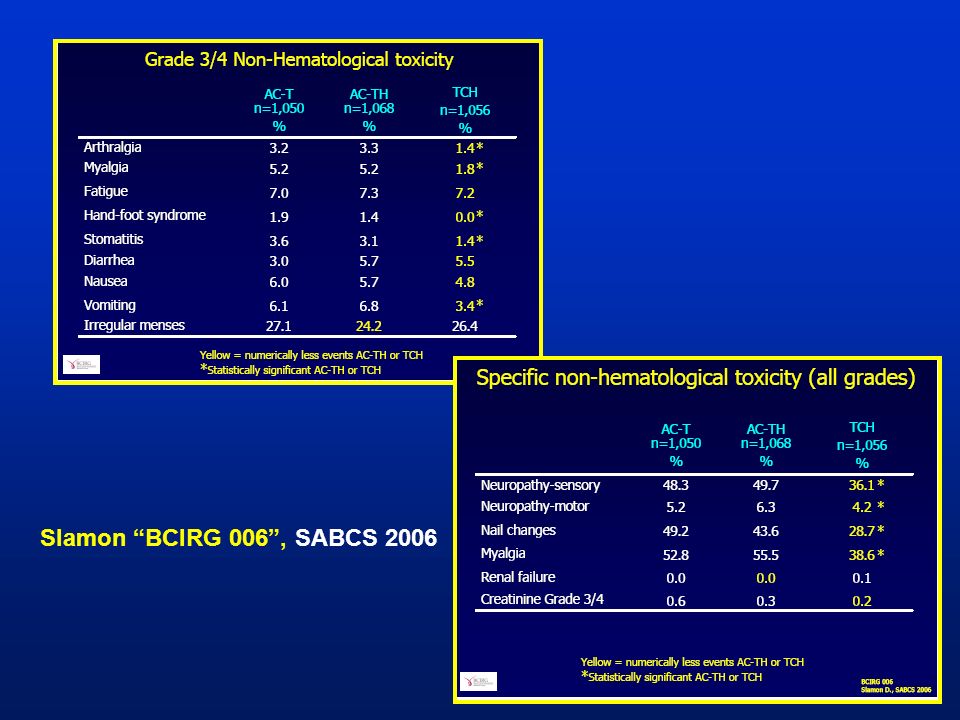
Slamon “BCIRG 006”, SABCS 2006

64
TC vs AC

65
Jones S. et al. JCO 2006 TC vs AC

66
TC vs AC: results I Jones S. et al. JCO 2006

67
TC vs AC: results II

68
Jones S. et al. JCO 2006 TC vs AC: toxicity

69
Conclusion: Thirty-one years ago, the original AC regimen was reported. Now, there is a superior nonanthracycline regimen, TC. At 5 years, TC was associated with a superior DFS and a different toxicity profile compared with AC. Jones S. et al. JCO 2006

70
High Risk Patient provocative new scenarious HR negative Node neg/pos HER2 negative Topo II positive HR negative Node neg/pos HER2 positive Topo II negative HR negative Node neg/pos HER2 positive Topo II positive HR negative Node neg/pos HER2 negative Topo II negative FEC FEC docetaxel Taxanes(carbo) + Trastuzumab FC(caelyx)C + Trastustumab Taxanes + Cyclophosphamide
 + Trastuzumab FC(caelyx)C + Trastustumab Taxanes + Cyclophosphamide")
71
The End Stop Here

72
AnthacyclinesTaxanes Haematologic GastrointestinalNeurological CardiacHipersensivity reaction Dermatological Cardiac MAIN TOXICITY ????????

73
When should we offer a Taxane-regimen ? Which Taxane: Paclitaxel ? Docetaxel ? Which Regimen:Sequential A(C) T, Combined AT ? Which Antracycline regimen:(CEF ?) Which Schedule:3 Weekly, Weekly ? Which Patients ?:Role of Predictive Factors Best Use of Taxanes / Anthracyclines
 T, Combined AT . Which Antracycline regimen:(CEF ) Which Schedule:3 Weekly, Weekly . Which Patients :Role of Predictive Factors Best Use of Taxanes / Anthracyclines.")
74
Adjuvant Taxanes : which data from randomized trials Adjuvant taxanes improve DFS (Level 1 evidence ?) 2 positive trials (CALGB 9344, BCIRG 001) 1 negative trial ( NSABP B-28), but: TAM concomitant to chemotherapy TAM to all pt >50 years old Adjuvant Taxanes do not improved OS: longer follow-up waiting for ongoing trials results Adjuvant taxanes increase toxicity
 2 positive trials (CALGB 9344, BCIRG 001) 1 negative trial ( NSABP B-28), but: TAM concomitant to chemotherapy TAM to all pt >50 years old Adjuvant Taxanes do not improved OS: longer follow-up waiting for ongoing trials results Adjuvant taxanes increase toxicity")
75
Slamon “BCIRG 006”, SABCS 2006 Togliere ???

76
Slamon “BCIRG 006”, SABCS 2006 ?????

77
Adjuvant Chemotherapy Options Trastuzumab if HER-2 positive CMF ? TAXANES ? adapted from Piccart et al. (2005)
.")
Similar presentations






 Phase III trial comparing AC (x4)taxane (x4) with taxane (x8) as adjuvant therapy for node-positive breast cancer: Results of N-SAS-BC02.>")


 on the Efficacy.>")




 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")





: investigational agents TTP = median time to disease progression OS = median overall survival.>")
 upregulation Dose- and time-dependent upregulation of TP in human colon cancer xenografts 20 15 10 5 0 20 15 10 5 0 PaclitaxelDocetaxel.>")