Download presentation
Presentation is loading. Please wait.

1
The International Pharmaceutical Regulatory and Compliance Congress and Best Practices Forum Brussels, June 6-8, 2007 The pharmaceutical industry and the regulations Girolamo Sirchia MD, FRCP Edin former Minister of Health, Italy

2
Starting points Innovative drugs are of paramount importance for human beings Medicinal products are ethical goods Regulations

3
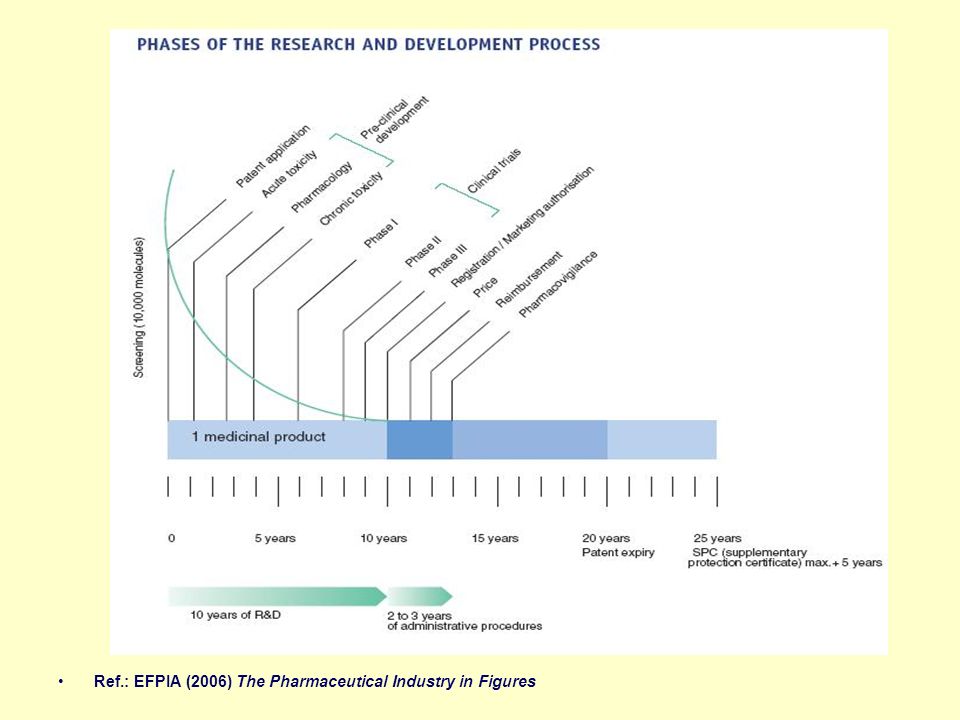
Ref.: EFPIA (2006) The Pharmaceutical Industry in Figures
 The Pharmaceutical Industry in Figures")
4
Innovative drugs stem from research Research and development are mainly designed, managed and paid by Big Pharma

5
1.Critical issues in pharmaceutical innovation 1.1. Research and development investments 1.2. Marketing pressure 1.3. Clinical trials 1.4. Priority medicines 1.5. Accessibility of medicines 1.6. Counterfeit medicines

6
1.1. Research and development investments

7
Pharmaceutical R&D costs are very high on account of the high attrition rate during the drug development process

8
Ref.: EFPIA (2006) The Pharmaceutical Industry in Figures
 The Pharmaceutical Industry in Figures")
10
1.2. Marketing pressure Big investments require big returns Marketing Marketing is addressed to prescribing physicians but also the involvement of Patient Associations, journalists and the media, politicians and civil servants is not uncommon

11
The mainstay of the industry marketing action: ❶ Advertisements directed to physicians ❷ Visits to physicians by sales representatives ➌ Gifts to physicians and their Institutions ➍ Direct-to-consumer advertising (USA)
")
12
A number of cases have brought to lights an unhealthy relationship between manufacturers and the medical profession which demonstrate how Company practices frequently cross the divide separating patient welfare from profit-seeking behaviour

13
1.3. The ethical problem of research: Clinical Trials design and management of trials the choice of comparators and ATV drafting of papers by ghost-writers relations with investigators

14
The risks of influencing the results and only publishing the results desired

15
1.4. The ethical problem of research: priority medicines predominance of drugs for the most common pathologies of industrialised countries

16
Priority Medicines for Europe and the World (Kaplan and Laing, 2004) 1. Infections due to antibacterial resistance 2. Pandemic influenza 3. Cardiovascular disease (secondary prevention) 4. Diabetes (Type 1 and Type 2) 5. Cancer 6. Acute stroke 7. HIV/AIDS 8. Tuberculosis 9. Neglected diseases 10. Malaria 11. Alzheimer disease 12. Osteoarthritis 13. Chronic obstructive pulmonary disease 14. Alcohol use disorders: liver diseases and dependency 15. Depression in the elderly and adolescents 16. Postpartum haemorrhage 17. Smoking cessation
 4. Diabetes (Type 1 and Type 2) 5. Cancer 6. Acute stroke 7. HIV/AIDS 8. Tuberculosis 9. Neglected diseases 10. Malaria 11. Alzheimer disease 12. Osteoarthritis 13. Chronic obstructive pulmonary disease 14. Alcohol use disorders: liver diseases and dependency 15. Depression in the elderly and adolescents 16. Postpartum haemorrhage 17. Smoking cessation.")
17
1.5. Accessibility of Medicines Access to essential drugs by developing countries: November 14th, 2000: 4th WTO Conference of Ministers – Doha Declaration August 30th, 2003: WTO General Council – Decision December 18th, 2005: WTO Conference of Ministers – Reconfirmation of the Decision May 17th, 2006: the EU (Parliament and Commission) – Regulations on the granting of mandatory licences
 – Regulations on the granting of mandatory licences.")
18
Briefly The decisions enabled given countries in a particular state of need to produce pharmaceutical products protected by patents for their own internal needs, and excluding export sales

19
1.6. Counterfeiting of drugs 7% of all drugs sold in the world are fake Serious consequences for public health and the industries (WHO)
.")
20
Frequency of counterfeiting Less than 1% in developed countries 10 to 30% in Africa, Asia, South America 20% in the States of the former URSS 50% of drugs bought on the web

21
Challenges for pharmaceutical industries Industry reputation Operation difficulties

22
Industry reputation Transparency Access to medicines Pricing Safety

23
Operation difficulties Cost-containment policy Bureaucracy Harmonisation Pricing and reimbursement criteria Access to the market Patent challenges Parallel importation Counterfeits Generics

24
(Courtesy of Dr. Thomas Lönngren)
")
25
2. Recommendations. States should: 2.1. Support pharmaceutical industry to achieve specific targets 2.2. Assure fast pricing and reimbursement procedures 2.3. Control pharmaceutical expenditure 2.4. Develop phase IV studies and improve pharmacovigilance 2.5. Promote independent research 2.6. Promote solidarity

26
2.1. Sustain the pharmaceutical industry to increase the production of innovative drugs Administrative simplification in testing, registering, pricing, reimbursement Recognition and reward of innovation Incentives for ATV (premium prices) Reward of Companies that invest in research and manufacture in the country
 Reward of Companies that invest in research and manufacture in the country.")
27
2.2. Pricing and reimbursement P ricing, reimbursement and reimbursement access time within the EU is the prerogative of single States. This leads to differences between States

28
(Courtesy of Dr. Thomas Lönngren)
")
29
The capacity of the national authorities to recognise an innovative drug and make it reimbursable with a price that recognises the level of therapeutic efficacy is one of the objectives of the European Pharmaceutical Forum

30
The Paediatric Exclusivity Provision (Section 505A of the US FDA Modernization Act, 1997) Additional 6 months of patent protection in return for performing studies in children as specified by FDA A very similar program has been developed and adopted in EU Has been a success from the perspective of conducting trials for labelling in children Overcompensates blockbuster products
 Additional 6 months of patent protection in return for performing studies in children as specified by FDA A very similar program has been developed and adopted in EU Has been a success from the perspective of conducting trials for labelling in children Overcompensates blockbuster products")
31
It is believed by many that it would be appropriate for EMEA to propose a “Geriatric Exclusivity Provision” to the European Parliament similar to the Paediatric Exclusivity Provision and with similar advantages

32
In Italy a network of long-term care and geriatric hospitals is being organized. More than 5000 beds are available for clinical trials on acute and chronic fragile old people

33
2.3. Controlling pharmaceutical spending Natural increase Appropriate drug use Drugs for prevention Aggressive marketing

34
The use of drugs for prevention (statins, smoking dissuaders, etc.)
")
35
2.4. Aggressive marketing Relations between industry and investigators – Register of Trials Relations between industry and prescribing physicians ( Should we eliminate the sponsorship of congresses,CME, etc.?) ① Brennan et al, 2006 ③ Am. Med. Ass. J. of Ethics, 2006 ② The Prescription Project, 2007 ④ R. Smith, 2005
 ① Brennan et al, 2006 ③ Am. Med. Ass. J. of Ethics, 2006 ② The Prescription Project, 2007 ④ R. Smith,")
36
2.5. Pharmacovigilance (1) The European Commission believes that the pharmacovigilance system must be improved Cooperation between the States is indispensable in order to evaluate in an independent manner relative efficacy and safety in the clinical practice of innovative drugs
 The European Commission believes that the pharmacovigilance system must be improved Cooperation between the States is indispensable in order to evaluate in an independent manner relative efficacy and safety in the clinical practice of innovative drugs.")
37
2.5. Pharmacovigilance (2) The identification, design and prioritization of large phase 4 drug trials of public health importance represent a major medical, social and scientific effort that currently lacks a champion in the USA (Psay and Weiss, 2007) The Institute of Medicine’s Committee on Drug Safety has proposed a public-private partnership to help define key public health questions that merit investment in large, long-term phase 4 trials (2007)
 The identification, design and prioritization of large phase 4 drug trials of public health importance represent a major medical, social and scientific effort that currently lacks a champion in the USA (Psay and Weiss, 2007) The Institute of Medicine’s Committee on Drug Safety has proposed a public-private partnership to help define key public health questions that merit investment in large, long-term phase 4 trials (2007).")
38
2.6. Indipendent research Given that: ⒜ the research and development of drugs are important for humankind ⒝ industry is the largest investor in pharmaceutical research but manages the trials ⒞ high costs require industries to maximise revenues and thus invest in drugs with the largest market it is necessary that developed States invest in independent research

39
2.7. Access to essential drugs by developing countries: The initiatives hitherto implemented are insufficient Forms of health aid have a considerable diplomatic value

40
If we continue to believe that the bonds between persons and peoples can only be entrusted to contractual market relations without friendship and without respect for the rights of all to human values and essential goods (such as food, water, housing and health), our fate will be sealed (His Holiness Benedictus XVI, Message for the World Peace Day, 2007)
, our fate will be sealed (His Holiness Benedictus XVI, Message for the World Peace Day, 2007)")
41
A good start could be to study arrangements for making investments by States and Companies in favour of countries with poor economies remunerative

42
Conclusion: some political agreements are needed for an international roadmap 1.State investments Attention to the pharmaceutical industry Independent research Independent pharmacovigilance Supervision on the system’s ethical compliance Support to developing countries ctd.

43
2.Harmonisation between States (simpler and more harmonised regulations) 3.Independent information for physicians and the public on the correct use of drugs
 3.Independent information for physicians and the public on the correct use of drugs")
44
The USA and the EU should work together to lead the improvement

45
In the EU Vice President G ü nter Verheugen has recently proposed a Commission Communication pointing to an EU single market for pharmaceuticals. A first step in the right direction

46
(Courtesy of Dr. Thomas Lönngren)
")
Similar presentations

>")


















