Download presentation
Presentation is loading. Please wait.

2
COMET - Background, Rationale and Design

3
Pharmacological Differences Within the Blocker Class Agents currently evaluated for heart failure 1 2 1 Ancillary blockadeblockade blockade ISA effects* Carvedilol++++++ +++- +++ Metoprolol+++ ---- Bisoprolol+++ ---- Bucindolol++++++ - ++- *anti-oxidant, anti-endothelin, anti-proliferative lack of 1 receptor upregulation

4
TrialnHazard Ratio (95% CI) US Carvedilol Prog1,094 0.35 (0.20-0.61) CIBIS II 2,647 0.66 (0.54-0.81) MERIT-HF 3,991 0.66 (0.53-0.81) COPERNICUS2,289 0.65 (0.52-0.81) BEST2,708 0.90 (0.78-1.02) Prospective Outcomes Studies of Blockers in CHF Packer et al. NEJM 1996; CIBIS II Invest. Lancet 1999; MERIT-HF Study Gp. Lancet 1999 BEST Investigators. Lancet 1999; Packer et al. NEJM 2001 00.20.40.60.81 Mild to Moderate Severe

5
Carvedilol Or Metoprolol European Trial n3,029 patients with class II-IV heart failure were recruited at 317 centres in 15 European countries 6 40 37 7 17 16 27 71 12 2 24 8 4 36 10

8
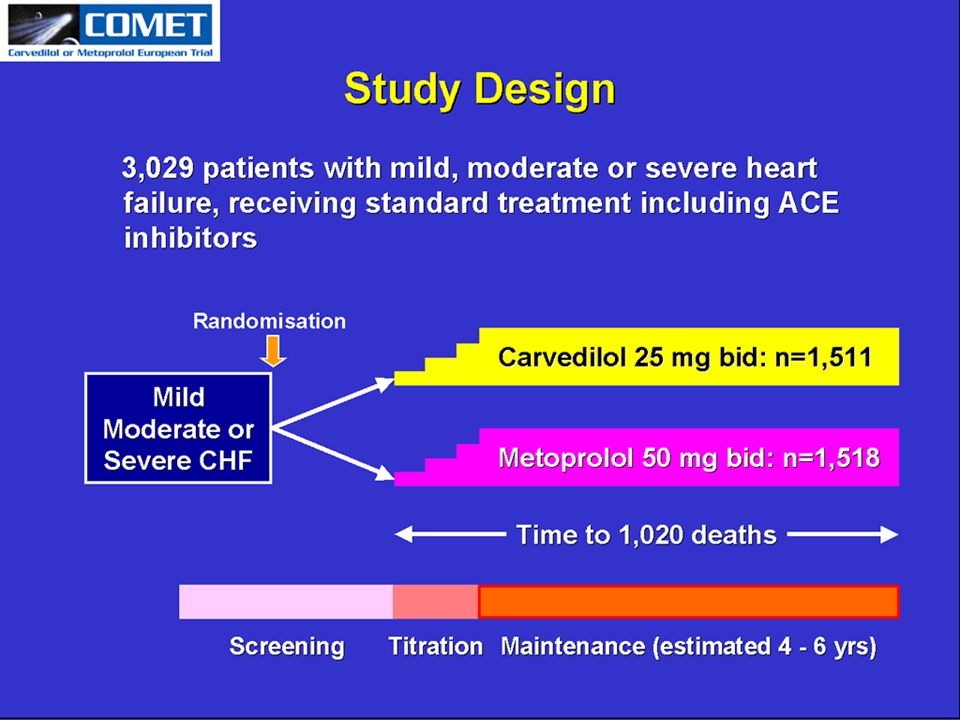
Objectives and Design nTo compare the effects of carvedilol with those of metoprolol on mortality and morbidity in patients with chronic heart failure nNo run-in period Mild, moderate or severe CHF Metoprolol (n = 1,518) Carvedilol (n = 1,511) Screening Titration Maintenance (estimated 4 - 6 yrs) Randomisation
 Carvedilol (n = 1,511) Screening Titration Maintenance (estimated yrs) Randomisation")
10
Dosing regimen nTarget dose –Carvedilol: 25 mg bd –Metoprolol tartrate: 50 mg bd nUp-titration at 2-week intervals –Carvedilol: 6.25, 12.5, 25 to 50 mg/day –Metoprolol: 10, 25, 50 to 100 mg/day

11
Main Inclusion Criteria nSymptomatic CHF (NYHA II-IV) on standard treatment nStable diuretic treatment 2 weeks nACE inhibitor 4 weeks prior to study entry –use of digitalis and/or vasodilators was discretionary nLVEF 35% n 1 CVS hospitalisation in the previous 2 years
 on standard treatment nStable diuretic treatment 2 weeks nACE inhibitor 4 weeks prior to study entry –use of digitalis and/or vasodilators was discretionary nLVEF 35% n 1 CVS hospitalisation in the previous 2 years")
12
Main Exclusion Criteria nCVA, AMI or unstable angina in prior 2 months nUntreated valve disease or arrhythmias nOther life threatening disease nContraindications to blocker therapy –Heart rate < 60 bpm –SBP < 85 mmHg –AV block, unless treated with a pacemaker –History of asthma or COPD –Unstable insulin dependent diabetes mellitus

13
Primary Endpoints nAll-cause mortality nAll-cause mortality or all-cause hospitalisation

14
Statistical Design nEvent driven, requiring at least 1,020 fatal events for the primary analysis nAll randomised patients were included in the ITT analysis nAll patients were followed to the end of the study, even if study treatment discontinued

15
Statistical Analysis nCo-primary endpoints were analysed by log rank test nRelative risk (Hazard Ratio) calculated using Cox proportional hazard model nFinal analysis had to achieve –P < 0.039 for ‘all cause mortality’ –P < 0.01 for ‘all cause mortality or hospitalisation’
 calculated using Cox proportional hazard model nFinal analysis had to achieve –P < for ‘all cause mortality’ –P < 0.01 for ‘all cause mortality or hospitalisation’")
16
Secondary Endpoints nAll-cause mortality or cardiovascular hospitalisation nCardiovascular death, non-fatal acute MI, heart transplantation or worsening of heart failure nCardiovascular death nNYHA class nWorsening of heart failure nHospital admissions and duration of hospitalisations for heart failure and other reasons nDiscontinuation of study therapy

17
Recruitment by Country (Centres) 26 46 53 54 88 91 129 163 210 221 238 278 355 725 397 0200400600800 Hungary (2) Norway (4) Portugal (7) Austria (12) Finland (10) Switzerland (6) Belgium (17) Denmark (8) UK (16) Italy (24) France (40) Spain (37) Netherlands (27) Sweden (36) Germany (71)
 Hungary (2) Norway (4) Portugal (7) Austria (12) Finland (10) Switzerland (6) Belgium (17) Denmark (8) UK (16) Italy (24) France (40) Spain (37) Netherlands (27) Sweden (36) Germany (71)")
18
Demography 1. NEJM 1996; 334:1349-55, active group 2. Lancet 1999; 353: 2001-7, active group 3. Lancet 1999; 353: 9-13, active group Male (%) 62 80 126 77 81 Systolic BP (mean mmHg) Heart rate (mean bpm) COMET N = 3,029 Age (mean yrs) Weight (kg) Diastolic BP (mean mmHg) 79 77 58 US Carvedilol 1 N = 696 116 72 - 84 MERIT-HF 2 N = 1,990 77 64 130 78 82 81 CIBIS-II 3 N = 1,327 81 61 129 80 79 -
 Systolic BP (mean mmHg) Heart rate (mean bpm) COMET N = 3,029 Age (mean yrs) Weight (kg) Diastolic BP (mean mmHg) US Carvedilol 1 N = MERIT-HF 2 N = 1, CIBIS-II 3 N = 1,")
19
COMET N = 3,029 IHD* / MI53% / 41% Dilated cardiomyopathy**27% Hypertension36% Prior valve surgery2% Diabetes24% Atrial fibrillation20% * Ischaemic Heart Disease ** Sole diagnosis Contributory Causes of Heart Failure

20
COMET N = 3,029 26 NYHA Class (%) 48II 48III 4IV LVEF (%) Severity of Heart Failure
 48II 48III 4IV LVEF (%) Severity of Heart Failure")
21
Background Therapy COMET N = 3,029 Diuretic99% ACEi91% ARB 7% Spironolactone11% Digoxin59% Aspirin37% Warfarin46%

22
COMET RESULTS

23
COMET Carvedilol or Metoprolol European Trial To compare the effects of carvedilol with those of metoprolol on the risk of death and of death or hospitalisation in patients with chronic heart failure

24
Primary endpoints nAll-cause mortality nCombined risk of death or hospitalisation for any reason Power: nTrial was designed to have 80% power to detect 20% difference in mortality and 15% in composite endpoint ( = 0.039 for mortality and 0.01 for the combined endpoint)
")
25
Randomised3029 Carvedilol1511Metoprolol1518 Assigned to drug and received at least one tablet Withdrew consent 10 Lost to follow-up 3 Withdrew consent 18 Lost to follow-up 2 Flow chart of patients

26
477157.9 Minimum follow-up (months): Maximum follow-up (months): Average follow-up (months): 175447 (=14621 years) 1112 Total patient months of follow-up: Total deaths prior to 15-Nov-2002: 01-Dec-199615-Jan-1999302915111518 First patient recruited: Last patient recruited: Total recruited: Carvedilol:Metoprolol: Dates, timing and follow-up
: Maximum follow-up (months): Average follow-up (months): (=14621 years) 1112 Total patient months of follow-up: Total deaths prior to 15-Nov-2002: 01-Dec Jan First patient recruited: Last patient recruited: Total recruited: Carvedilol:Metoprolol: Dates, timing and follow-up")
27
5452 Aetiology (IHD %) 42.2/2042.6/22 Months of HF (mean/median) 24.423.8Diabetes 19.220.5 AF/flutter (%) 8181 Heart rate (beats/min) 49/47/448/48/3 NYHA class (%) II/III/IV 7777 Diastolic BP (mm Hg) 126126 Systolic BP (mm Hg) 80.279.4 Male (%) 62.3/11.461.6/11.3 Age (y, mean/sd) Metoprolol(n=1518) Carvedilol (n=1511) Baseline characteristics
 42.2/2042.6/22 Months of HF (mean/median) Diabetes AF/flutter (%) 8181 Heart rate (beats/min) 49/47/448/48/3 NYHA class (%) II/III/IV 7777 Diastolic BP (mm Hg) Systolic BP (mm Hg) Male (%) 62.3/ /11.3 Age (y, mean/sd) Metoprolol(n=1518) Carvedilol (n=1511) Baseline characteristics")
28
Time (years) Mortality (%) 0 10 20 30 40 012345 Metoprolol Carvedilol hazard ratio 0.83, 95% CI 0.74-0.93, P = 0.0017 Number at risk Carvedilol151113671259 11551002383 Metoprolol151813591234 1105933352 Primary endpoint of mortality
 Mortality (%) Metoprolol Carvedilol hazard ratio 0.83, 95% CI , P = Number at risk Carvedilol Metoprolol Primary endpoint of mortality")
29
0.500.751.001.251.50 Sexmale female Age < 65 65 NYHAII III IV CauseOther IHD LVEF 25% > 25% Heart rate < 80 80 Systolic BP < 110 110 - 139 140 Diabetesyes no Overall Carvedilol better Metoprolol better 410 1200 500 1217 0.80 175 730 228 736 0.75 309 732 324 716 0.91 28 49 48 66 0.68 28 49 48 66 0.68 102 311 100 301 0.97 207 834 231 803 0.84 305 677 369 715 0.84 198 735 219 703 0.83 314 776 381 815 0.85 314 776 381 815 0.85 270 706 285 630 0.79 221 743 287 819 0.84 234 693 284 733 0.86 277 816 314 783 0.80 120 245 132 235 0.80 121 447 158 434 0.71 153 360 178 371 0.85 359 1150 419 1143 0.82 512 1511 600 1518 0.83 512 1511 600 1518 0.83 270 817 310 849 0.89 deaths n deaths n HR deaths n deaths n HR Carvedilol Metoprolol Carvedilol Metoprolol Mortality in sub-groups

30
10.08.3 Annual mortality 0.1222 0.863, 1.018 0.9371160/151876.4%1116/151173.9% Mortality or all cause hosp. 0.0017 0.736, 0.932 0.828600/151839.5%512/151133.9%Mortality P 95% CI HazardRatioMetoprololCarvedilolPrimaryendpoints Primary endpoints

31
Daily target doseMean dose received (given in divided doses bid) Carvedilol50 mg 42 mg Metoprolol 100 mg 85 mg Dose of drugs
 Carvedilol50 mg 42 mg Metoprolol 100 mg 85 mg Dose of drugs")
32
Heart rate (beats.min -1 ) Metoprolol Carvedilol Time (years) 70 75 80 012345 65 85 ** * * P < 0.05, ** P < 0.01 Error bars represent 1 standard error Heart rate
 Metoprolol Carvedilol Time (years) ** * * P < 0.05, ** P < 0.01 Error bars represent 1 standard error Heart rate")
33
Time (years) Error bars represent 1 standard error Blood pressure (mm Hg) 70 80 90 100 110 120 130 012345 ****************** ******** * P = 0.05 ** P = 0.01 *** P = 0.001 Blood pressure Metoprolol Carvedilol
 Error bars represent 1 standard error Blood pressure (mm Hg) ****************** ******** * P = 0.05 ** P = 0.01 *** P = Blood pressure Metoprolol Carvedilol")
34
95.8%75.8%77.4%57.4%82748393.6%73.9%75%55.1%762481 Patients with at least one AE Patients with at least one CV AE Patients with at least one SAE Patients with at least one CV SAE Patients withdrawn any cause Patients withdrawn excl. deaths 15181511NMetoprololCarvedilol Adverse events and withdrawals

35
8.9% 2.6% 2.6%10.5%1.9%9.5%2.6%14.2%3.2% Bradycardia as AE Bradycardia as SAE Hypotension as AE Hypotension as SAE 15181511NMetoprololCarvedilol Events related to blockade

36
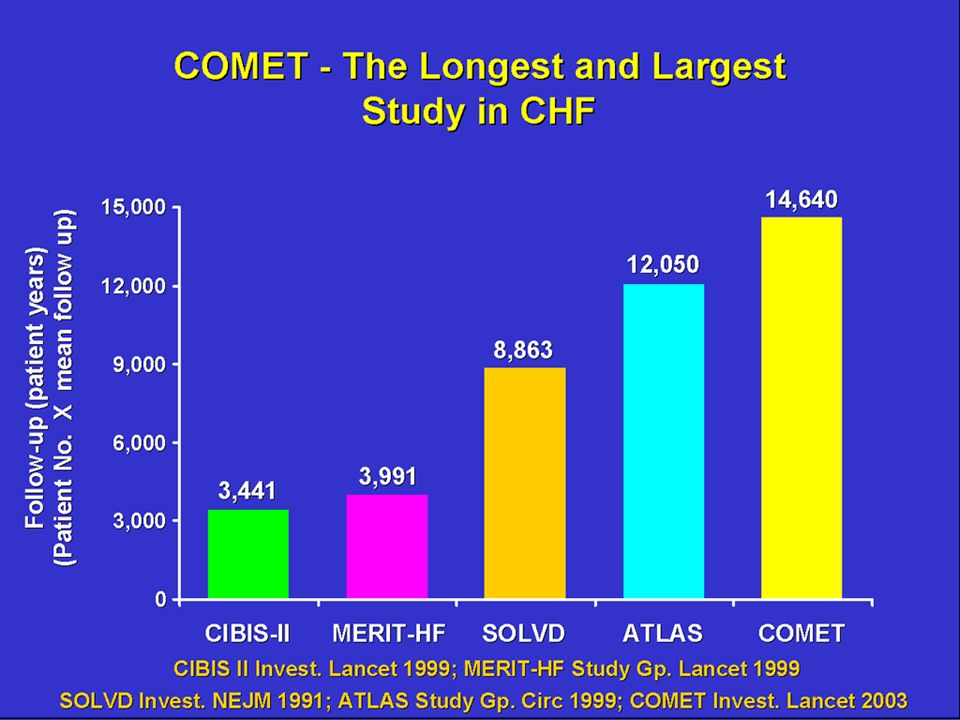
Summary and conclusion nCOMET is the longest and largest study in CHF nFirst head-to-head mortality study comparing two beta- blocking agents in CHF nCarvedilol saved significantly more lives than metoprolol (by 17%, P = 0.0017) nCarvedilol compared to metoprolol reduced annual mortality from 10.0% to 8.3% and prolonged median survival by 1.4 years nCarvedilol is the preferred beta-blocker for the treatment of chronic heart failure
 nCarvedilol compared to metoprolol reduced annual mortality from 10.0% to 8.3% and prolonged median survival by 1.4 years nCarvedilol is the preferred beta-blocker for the treatment of chronic heart failure")
Similar presentations



 Trial>")
, B Dahlöf (Co-chair), N Poulter (Secretary), H Wedel (Statistician), G Beevers, M Caulfield, R Collins, SE Kjeldsen, A Kristinsson,>")









 Monotherapy versus ARB plus Calcium Channel Blocker Combination on Cardiovascular Events in Japanese.>")


>")




