Download presentation
Presentation is loading. Please wait.

1
INTEGRATED CARE MANAGEMENT AND QUALITY IMPROVEMENT QIO Request Submission Requirements New 6/14/2012

2
Topics Service Type(s) KePRO SCDHHS Website Service Type Requirements Contact Information
 KePRO SCDHHS Website Service Type Requirements Contact Information")
3
Prior Authorization Service Types PRTF-Psychiatric Residential Treatment Facility Freestanding Inpatient Psychiatric (under 21 y.o.)
")
4
Forms Navigate to Forms TAB to obtain Documents

5
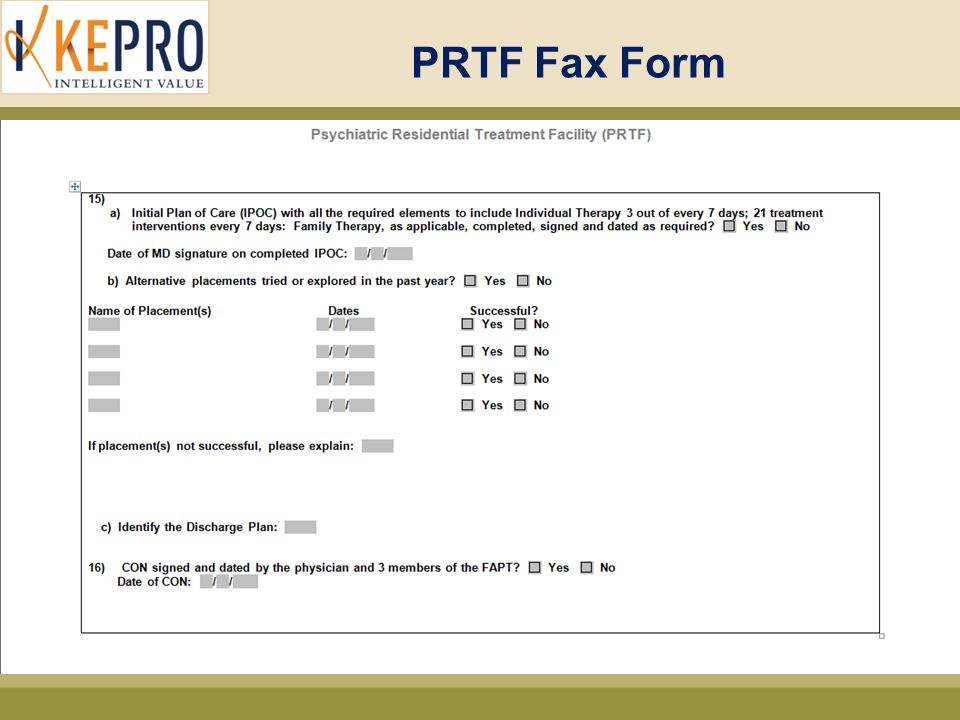
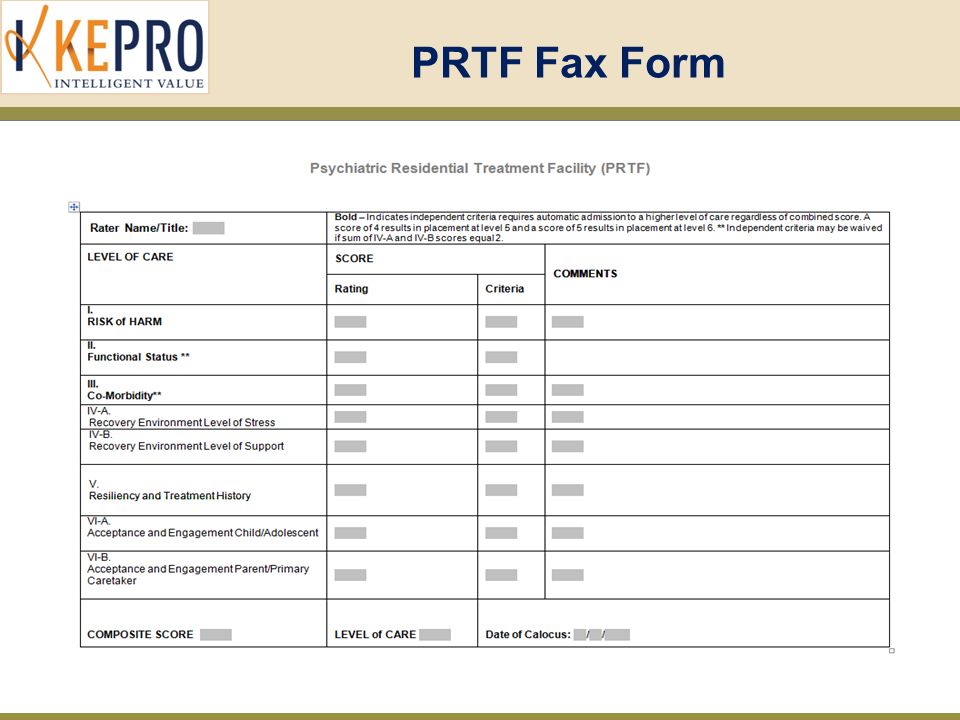
PRTF Fax Form

8
Freestanding Psychiatric Inpatient (under 21) Fax Form
 Fax Form")
10
PRTF

11
Psychiatric Residential Treatment Facilities (PRTFs) are facilities, other than a hospital, that provides psychiatric services to children under age 21 in an inpatient setting. PRTFs provide Inpatient Psychiatric Services to children under 21 who do not need acute inpatient psychiatric care, but need a structured environment with intensive treatment services. PRTF admissions must be prior authorized by KEPRO

12
PRTF Required Documentation for Provider’s Records: CALOCUS Must be completed and current within 90 days prior to requested start date Certificate of Need (CON) Valid for 45 days from the date it is completed 30 day treatment plan Plan must be created within first 14 days Required documentation to submit to KePRO: PRTF Fax form Provider will attest to information from CALOCUS and CON 30 day treatment plan Plan must be created within first 14 days Additional clinical
 Valid for 45 days from the date it is completed 30 day treatment plan Plan must be created within first 14 days Required documentation to submit to KePRO: PRTF Fax form Provider will attest to information from CALOCUS and CON 30 day treatment plan Plan must be created within first 14 days Additional clinical")
13
LENGTH OF APPROVAL Requests initially approved for a 90-day stay. Continued stay requests approved for a 90-day stay. If indication given that the recipient is a “SUB CLASS” (DJJ juveniles with a serious mental illness) – approvals will be issued in 180-day increments.
 – approvals will be issued in 180-day increments..")
14
OVERLAPPING REQUESTS Requests for services will not be approved with overlapping dates. If for same facility, new approval period will not be approved until the old approval has ended. If for a different facility, the first-approved facility must send in notice of discharge prior to new approval being issued.

15
PRTF Criteria Initial Admission –McKesson Interqual Psychiatric Residential Treatment Level of Care Functioning criteria –SCDHHS Psychiatric Hospital Services Provider Manual

16
CRITERIA FOR PRTF ADMISSION Current diagnosis Symptoms/behaviors (length experienced and intensity) Prior treatment history Support system Functioning – How illness affects performance of ADLs and relationships with others.
 Prior treatment history Support system Functioning – How illness affects performance of ADLs and relationships with others.")
17
PRTF - CONTINUED STAY REQUESTS Require treatment plan which has been updated within previous 30 days. After one year, requires submission of new CALOCUS, updated treatment plan, and clinical information to meet McKesson requirements. Criteria requires information on current symptoms, how illness is affecting functioning, and current services being received.

18
FREESTANDING PSYCHIATRIC INPATIENT (UNDER 21)
")
19
CRITERIA Inpatient Freestanding Psychiatry Must meet criteria for either: –Immediate Safety Risk –Potential Safety Risk

20
IMMEDIATE SAFETY RISK Symptoms within previous 48 hours. Recipient is exhibiting symptoms that lead to immediate concern of decreased safety for recipient or other people. Example: Suicidal with definite plan

21
POTENTIAL SAFETY RISK Symptoms present within last week that lead to concern over recipient’s safety. As this is less urgent, requires more detailed documentation of medical necessity.

22
POTENTIAL SAFETY RISK Clinical to be submitted includes: –Symptoms/circumstances that cause concern –Social risk; changes within previous month in relationships with others, role performance (school) or residence –Is recipient expected to adhere to treatment plan? –Why is current support system inadequate to provide care as an outpatient?

23
ADOLESCENT SUBSTANCE USE Freestanding Inpatient Psychiatry admissions for substance use issues have a separate set of criteria that must be met. Requirements include submission of the recipient’s history of substance use as well as behaviors exhibited as a result of substance use.

24
CRITERIA – ADOLESCENT SUBSTANCE USE Require evidence of impairments in: –Relationships – such as a negative peer group or gang involvement, or increased conflicts with others. –Role performance – How has substance use affected education?

25
CRITERIA – ADOLESCENT SUBSTANCE USE Admission to a residential treatment center for substance use issues also requires information on: –Prior treatment history –Issues in current social/home setting that places the recipient at increased risk –Support system

26
Registration for Atrezzo Connect Provider Portal INTEGRATED CARE MANAGEMENT AND QUALITY IMPROVEMENT

27
How To Register For Atrezzo Connect Website Address: https://scdhhs.kepro.com https://scdhhs.kepro.com Select “ Registration For Atrezzo Connect” (Slide 3) Enter your 10 digit National Provider Identifier (NPI) number and Legacy South Carolina Medicaid provider ID Select a unique user name and password & complete required user information
 Enter your 10 digit National Provider Identifier (NPI) number and Legacy South Carolina Medicaid provider ID Select a unique user name and password & complete required user information")
29
Atrezzo Connect Atrezzo Connect allows for: – Secure access to Atrezzo Connect (Provider Portal) – Provider will be able to access letters by Case/Request, Respond/Send messages To/From KePRO
 – Provider will be able to access letters by Case/Request, Respond/Send messages To/From KePRO")
30
Required Information for Security Verification The provider must enter information to verify authenticity for security reasons Registration Code: – SCDHHS Legacy ID

31
Simple -5 Step Registration Process Start by clicking the Atrezzo Login button on the SCDHHS-KePRO website

32
Login Page You will be brought to this login page

33
Step 2 – Enter NPI and Legacy ID Enter your organization’s NPI number and Legacy Provider ID = Provider Registration Code Click NEXT

34
Step 3 – Terms of Agreement Review Terms of Agreement. Upon acceptance, you will be taken to setup for User information.

35
Step 4 – Verify Address Click on the correct address(s) for the new account (this associates your user information with these locations) If all apply, check all of them Click SELECT
 for the new account (this associates your user information with these locations) If all apply, check all of them Click SELECT")
36
Step 5 – Enter Account Information Enter user account information User Name, Password, First/Last Name, E-mail and Fax Number are required fields! Click NEXT-This will take you to the Password setup and security question Slide) Passwords do not expire. Minimum 8 characters required.
 Passwords do not expire. Minimum 8 characters required..")
37
Successful Completion Successful Completion of setup, takes you to the Home Page

38
View all request and Create new request Click Member to search using Member id or Last name/DOB Click Request/Case to search using Case id, Member info or Request info

39
Create Preferences, Manage User accounts and New Provider Registration Use this tab to change your password or update your contact information View Atrezzo User Guide and View FAQs

40
Account Administrator All information submitted for registration under Provider/Facility Information will represent as the Provider Portal Administrator (Group Admin). The Group Admin is responsible for managing and creating all Submitting User accounts for your NPI # – Create other Group Admins’ & Admin Users – Set Preferences, i.e. Diagnosis and Procedure codes, etc

41
KePRO Contacts

42
42 Thank You!

Similar presentations







 : MRI, MRA, CAT, CTA and Pet Scans INTEGRATED CARE MANAGEMENT.>")





 course Section 2: VCSS Account Registration & Requesting Access This presentation.>")
 New 1/15/2015.>")






>")