Download presentation
Presentation is loading. Please wait.

1
Cardiovascular Disease in Women Dr Ghada Mikhail Consultant Cardiologist St Mary’s Hospital Trust

2
Death By Cause - Women 2004 UK BHF 2006 heartstats.org -CVD is responsible for 36% of deaths in women (37% in men) -Higher than deaths from all cancers combined -Breast CA is responsible for 4% deaths in women Deaths from CVS is almost 9 times higher than deaths from breast cancer.
 -Higher than deaths from all cancers combined -Breast CA is responsible for 4% deaths in women Deaths from CVS is almost 9 times higher than deaths from breast cancer.")
3
Death By Cause - Women 2004 Europe CVD is responsible for 55% of deaths in women (43% in men) 18 x mortality compared to Breast cancer
 18 x mortality compared to Breast cancer")
4
Age specific death rates from CHD, women, 1968-2003., UK, plotted as a percentage of the rate in 1968 BHF 2005 heartstats.org In women: 50% (50% in men) fall in death rates in those aged 55-64yrs 32% (35% in men) fall in death rates in those aged 35-44 yrs
 fall in death rates in those aged 55-64yrs 32% (35% in men) fall in death rates in those aged yrs")
5
BHF 2005 heartstats.org Age standardised coronary event rates, women aged 34-65 MONICA-WHO ( MONitoring trends and determinants In CArdiovascular disease)
")
6
Many women lack the basic awareness that CVD is their leading cause of death Health care professionals- Mx remains a challenge Research- women are underrepresented in clinical studies

7
CVD in Women – under-diagnosed, under- treated and under-researched Gender Differences Presentation Investigation Treatment Prognosis

8
Risk Factors Age *Smoking *Diabetes Mellitus *Hypertension (LVH) *Hyperlipidaemia (especially HDL,TG in women) Family History of CHD Homocysteine *CRP Menopause Sedentary Lifestyle Biggest Risk factor is the misconception that CHD is a ‘’Man’s Disease’’ AHA and ACC – guidelines for gender specific risk assessment - guidelines for primary and secondary prevention ESC BCS- guidelines in progress
 *Hyperlipidaemia (especially HDL,TG in women) Family History of CHD Homocysteine *CRP Menopause Sedentary Lifestyle Biggest Risk factor is the misconception that CHD is a ‘’Man’s Disease’’ AHA and ACC – guidelines for gender specific risk assessment - guidelines for primary and secondary prevention ESC BCS- guidelines in progress")
9
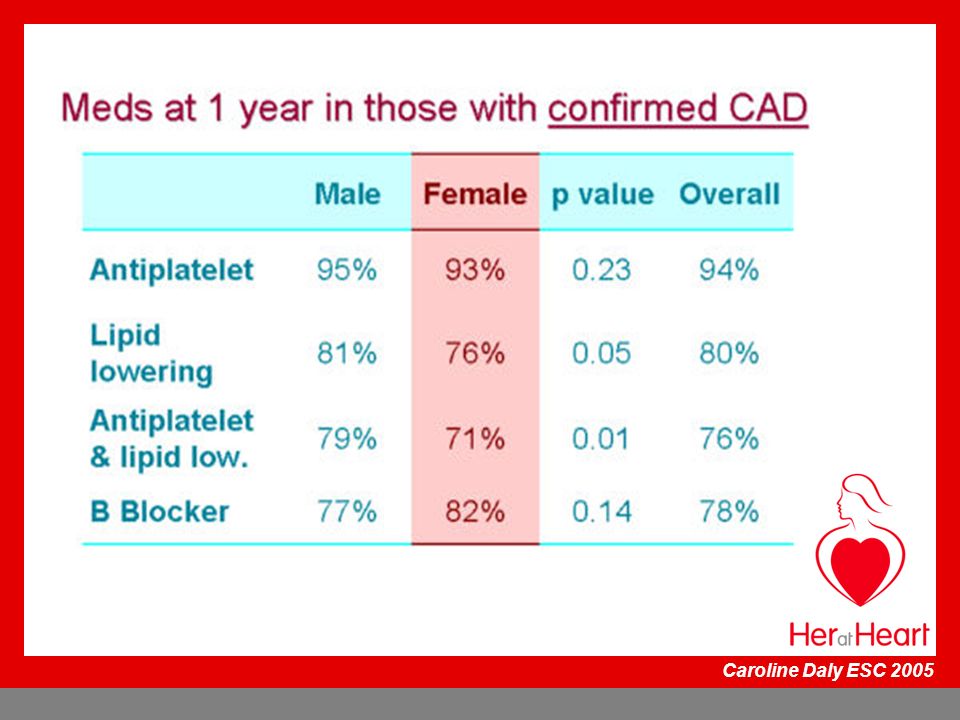
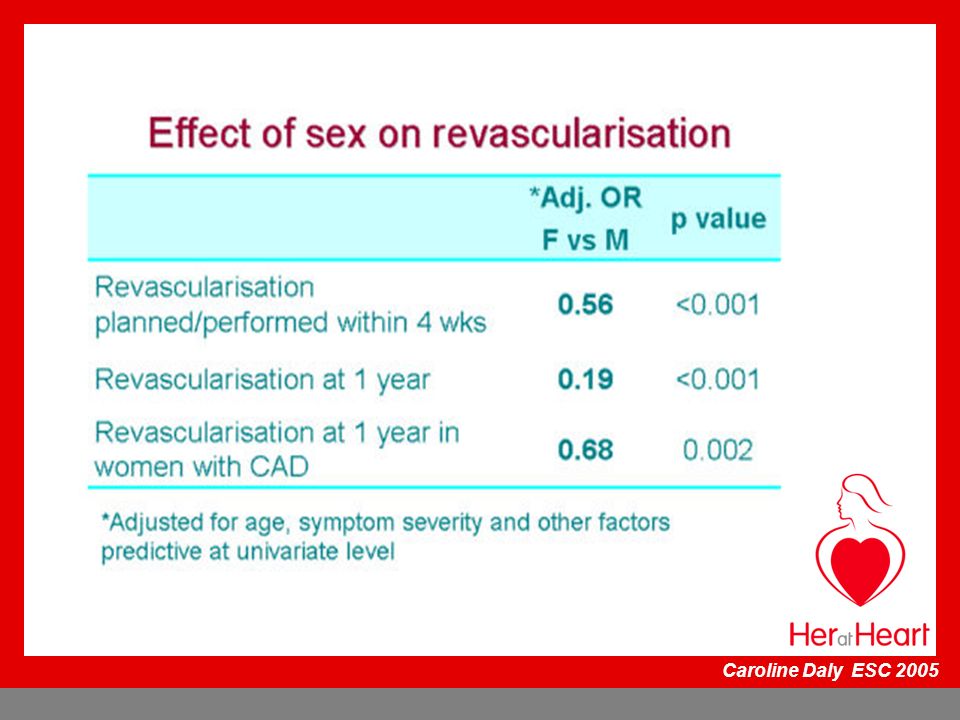
Euro Heart Survey of Angina n=3779 North n= 521 Mediterranean n=966 Central n=1341 West n=951 Caroline Daly ESC 2005

13
Effect of gender on risk of death/MI *MV HR95% CIp value Female vs Male2.08 1.13- 3.83 0.01 Abnormal LV Fxn.2.03 1.04- 3.94 0.04 Multivariate HR adjusted for age, DM, LV function and severity of CAD Caroline Daly 2005

14
Coronary Revascularisation PCI/CABG At the time of presentation with CAD, women are older and have more co-morbid factors Increased co-morbid factors -Older -Smaller in size -Hypertension -Diabetes mellitus -Hypercholesterolaemia -Peripheral vascular disease -Congestive cardiac failure (diastolic dysfunction)
")
15
Coronary Revascularisation- PCI/CABG Smaller vessel size Coronary lesion distribution and morphology is similar Women tend to have more ostial vessel disease Women receive less IMA conduits than men Stent usage is less Use of GPIIb/IIIa is less in women Higher incidence of urgent procedures

16
Coronary Revascularisation- PCI/CABG Higher mortality rate In-hospital mortality –x 2 times higher for CABG Increased mortality in younger women (? Ovarian dysfunction, ? Abnormalities of oestrogen receptors ) Higher vascular (stroke, groin) complications Higher bleeding and renal complications in women At 5 years after CABG and PCI- survival similar for men & women
 Higher vascular (stroke, groin) complications Higher bleeding and renal complications in women At 5 years after CABG and PCI- survival similar for men & women.")
17
RAVELRAVEL SIRIUSSIRIUS ESIRIUSESIRIUS T A X U S II T A X U S IV T A X U S VI MeanMean %F%F 25312924282427 Age (y) 6162 6162
")
18
TAXUS IV: n= 1,314 662 patients: (187 [28.2%] women) randomised to TAXUS 652 patients: (180 [27.2%] women) randomised to BMS Primary endpoint Rate of ischemia-driven target vessel revascularisation at 9 months Key Secondary Endpoints: MACE Angiographic (QCA) endpoints pre-specified in 732 patients Lanskey et al JACC 2005 TAXUS IV Gender Analysis TAXUS IV Gender Analysis
![TAXUS IV: n= 1, patients: (187 [28.2%] women) randomised to TAXUS 652 patients: (180 [27.2%] women) randomised to BMS Primary endpoint Rate of ischemia-driven target vessel revascularisation at 9 months Key Secondary Endpoints: MACE Angiographic (QCA) endpoints pre-specified in 732 patients Lanskey et al JACC 2005 TAXUS IV Gender Analysis TAXUS IV Gender Analysis](http://images.slideplayer.com/33/8196423/slides/slide_18.jpg "TAXUS IV: n= 1, patients: (187 [28.2%] women) randomised to TAXUS 652 patients: (180 [27.2%] women) randomised to BMS Primary endpoint Rate of ischemia-driven target vessel revascularisation at 9 months Key Secondary Endpoints: MACE Angiographic (QCA) endpoints pre-specified in 732 patients Lanskey et al JACC 2005 TAXUS IV Gender Analysis TAXUS IV Gender Analysis")
19
P=0.30P=0.03P=0.02P=0.07P=0.02 Patients (%) Control (N=180) TAXUS (N=187) Cardiac death MI TLR TVR MACE TAXUS IV- Female Group MACE at 1 Year MACE at 1 Year 66 %49 %40 %41 % No stent thrombosis in either group at 1 year Lanskey et al JACC 2005 MC Morice Euro PCR 2005
 Control (N=180) TAXUS (N=187) Cardiac death MI TLR TVR MACE TAXUS IV- Female Group MACE at 1 Year MACE at 1 Year 66 %49 %40 %41 % No stent thrombosis in either group at 1 year Lanskey et al JACC 2005 MC Morice Euro PCR 2005")
20
In-stentAnalysis Segment In-stent Analysis Segment P<0.0001 mm Control (N=72) TAXUS (N=81) TAXUS IV- Female Group Angiographic Results at 9 months Significant improvement in outcomes for MLD and Late Loss in TAXUS compare to Control Lanskey et al JACC 2005 MLD Late Loss MLDLate Loss
 TAXUS (N=81) TAXUS IV- Female Group Angiographic Results at 9 months Significant improvement in outcomes for MLD and Late Loss in TAXUS compare to Control Lanskey et al JACC 2005 MLD Late Loss MLDLate Loss")
21
In-stentAnalysis Segment In-stentAnalysis Segment Restenosis was significantly reduced with the TAXUS stent P<0.0001 P=0.001 P<0.0001P=0.001 Diameter Stenosis % % Control (N=72) TAXUS (N=81) TAXUS IV- Female Group Angiographic Results at 9 months Lanskey et al JACC 2005 Diameter StenosisRestenosis
 TAXUS (N=81) TAXUS IV- Female Group Angiographic Results at 9 months Lanskey et al JACC 2005 Diameter StenosisRestenosis")
22
TAXUS IV Gender Analysis Women – older, hypertension, diabetes, renal impairement, unstable angina, heart failure Women- higher unadjusted 1 year rates of TLR (7.6% vs 3.2%, p=0.03) Female gender - not an independent predictor of TLR or TVR
 Female gender - not an independent predictor of TLR or TVR")
23
M Leon ACC 2005

24
Baseline Patient Characteristics (I) WomenMenP-value Patients, n 1741109 Age, ys 65.6 ± 11 62.5 ± 10 <0.0001 Age > 75, % 21.8%12.7%0.002 Pre MI 40.2%50.9%0.009 Pre PCI 31.6%39.5%0.5 Pre CABG 17.2%18.7%0.75 UA31.0%26.8%0.27 MV disease 70.7%75.7%0.16 EF 53.1 ± 9.5 52.8 ± 10.1 0.69 IABP6.8%2.7%0.009 IIb/IIIa14.9%12.1%0.32 Experience in Milan
 WomenMenP-value Patients, n Age, ys 65.6 ± ± 10 < Age > 75, % 21.8%12.7%0.002 Pre MI 40.2%50.9%0.009 Pre PCI 31.6%39.5%0.5 Pre CABG 17.2%18.7%0.75 UA31.0%26.8%0.27 MV disease 70.7%75.7%0.16 EF 53.1 ± ± IABP6.8%2.7%0.009 IIb/IIIa14.9%12.1%0.32 Experience in Milan")
25
Baseline Patient Characteristics (II) WomenMen P- value Patients, n 1741109 Risk factors Family Hx 45.4%43.6%0.68 Hypertension73.0%65.6%0.06 Hypercholesterolae mia 71.3% 71.3%68.5%0.53 Current Smoker 12.1%16.1%0.18 Diabetes Mellitus 36.8%25.1%0.002 - Diet controlled - Diet controlled2.3%3.6%0.5 - Oral Agents - Oral Agents21.8%14.9%0.025 - Insulin - Insulin12.6%6.6%0.008 Experience in Milan
 WomenMen P- value Patients, n Risk factors Family Hx 45.4%43.6%0.68 Hypertension73.0%65.6%0.06 Hypercholesterolae mia 71.3% 71.3%68.5%0.53 Current Smoker 12.1%16.1%0.18 Diabetes Mellitus 36.8%25.1% Diet controlled - Diet controlled2.3%3.6%0.5 - Oral Agents - Oral Agents21.8%14.9% Insulin - Insulin12.6%6.6%0.008 Experience in Milan")
26
In-Hospital and 30-days Outcomes WomenMenP-value Patients, n 1741109 In-hospital Repeat revascularization Repeat revascularization0 0.1% (1) 1.0 Myocardial infarction* Myocardial infarction* 3.4% (6) 2.7% (30) 0.62 Acute thrombosis* Acute thrombosis* 0.6% (1) 0.1% (1) 0.25 30-days Subacute thrombosis 0 0.5% (5) 1.0 Death 0.6% (1) 0.5% (5) 0.58 MACE § 1.1% (2) 0.7% (8) 0.63 Experience in Milan § § excluding peri-procedural MI
 1.0 Myocardial infarction* Myocardial infarction* 3.4% (6) 2.7% (30) 0.62 Acute thrombosis* Acute thrombosis* 0.6% (1) 0.1% (1) days Subacute thrombosis 0 0.5% (5) 1.0 Death 0.6% (1) 0.5% (5) 0.58 MACE § 1.1% (2) 0.7% (8) 0.63 Experience in Milan § § excluding peri-procedural MI")
27
Clinical Outcomes at 1 year § WomenMenP Total Death 1.7% (3) 2.8% (31) 0.61 Cardiac death Cardiac death 1.1% (2) 2.3% (25) 0.57 Myocardial infarction* 2.3% (4) 2.1% (23) 0.78 Late thrombosis* 1.1% (2) 1.0% (11) 0.69 TLR 17.8 % (31) 14.9% (165) 0.31 TVR 19.0% (33) 18.4% (204) 0.83 MACE 20.7% (36) 21.3% (236) 0.92 CABG 0.6% (1) 0.8% (9) 1.0 § Median clinical follow-up: 13.9 months (IQR 11.5-17.5)
 2.8% (31) 0.61 Cardiac death Cardiac death 1.1% (2) 2.3% (25) 0.57 Myocardial infarction* 2.3% (4) 2.1% (23) 0.78 Late thrombosis* 1.1% (2) 1.0% (11) 0.69 TLR 17.8 % (31) 14.9% (165) 0.31 TVR 19.0% (33) 18.4% (204) 0.83 MACE 20.7% (36) 21.3% (236) 0.92 CABG 0.6% (1) 0.8% (9) 1.0 § Median clinical follow-up: 13.9 months (IQR )")
28
AMI Women: Older (approx 20 yrs) Higher incidence of risk factors Increased incidence in young women (<45 yrs) Present more often with angina rather than AMI Present more often with NSTEMI than with STEMI Higher proportion of ‘silent AMI’ (? older, diabetes, less awareness) Present later to hospital with AMI (? atypical symptoms, less awareness, man’s disease)
 Present later to hospital with AMI (. atypical symptoms, less awareness, man’s disease).")
29
AMI Women have higher rate of complications: - cardiogenic shock - congestive cardiac failure - reinfarction - peripheral bleeding - stroke Higher risk of cerebral bleeding with thrombolysis Higher early mortality than men Gender is an independent risk factor for mortality in AMI Mortality rate in younger women (<45 years) is over twice that in men Late presentation to hospital Less aggressively treated
 is over twice that in men Late presentation to hospital Less aggressively treated")
30
CABG Complications Stroke Post –operative haemorrhage Prolonged mechanical ventilation Post-operative renal failure Cardiac failure

31
Coronary Revascularisation- PCI/CABG Earlier detection of CAD by non-invasive imaging Wider use of stents Role of drug eluting stents Increasing use of GIIb/IIIa inhibitors Off-pump bypass surgery Minimal access procedures Research Studies / Trials

32
Women are evaluated less intensively and are undertreated Women under-represented in research studies Better awareness Appropriate access to diagnosis & treatment Earlier & more aggressive control of risk factors

33
AWARENESS HEALTH CARE PROFESSIONALS GENERAL PUBLIC - Education / Scientific Meetings - Research - Education /Scientific Meetings - Research

34
Scientific Initiatives & Awareness Campaigns Go Red Campaign – AHA -Heart Truth Campaign- NHLBI

35
European Society of Cardiology 2005

36
UK Scientific & Public Awareness Campaign

37
CVD in Women- CVD in Women- Healthcare Professionals Primary Care- GPs General Physicians Cardiologists Nursing staff- chest pain nurses Dept of Health BCS / BCIS Cardiac Networks CHD Leads Nursing Leads

38
CVD in Women- CVD in Women- Healthcare Professionals Symposium on CVD in Women- Friday 7 th July Recommendations Consensus Statement Working Group of BCS Research

39
CVD in Women- CVD in Women- General Public Symbol Website- heratheart.org.uk

41
Posters Patient Leaflets CVD in Women- CVD in Women- General Public Endorsed by BCS

Similar presentations











>")









