Download presentation
Presentation is loading. Please wait.

1
Syncope diagnostic algorithm and management MUDr. Jakub Honěk Kardiologická klinika, 2.LF UK a FN Motol, Praha

2
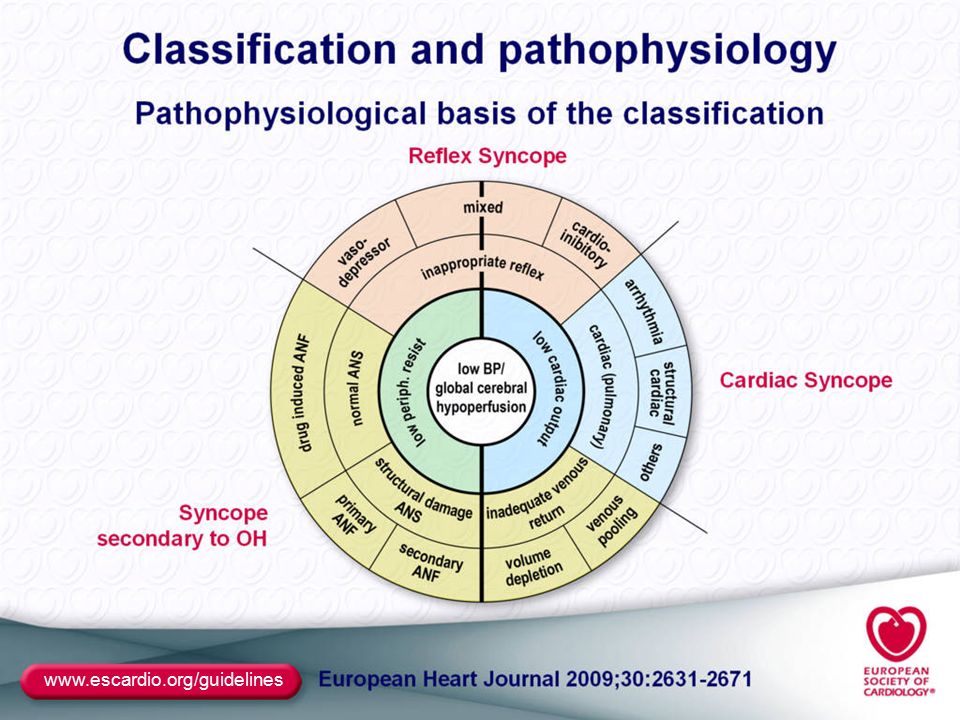
Definition of syncope Syncope is a T-LOC due to transient global cerebral hypoperfusion characterized by rapid onset, short duration, and spontaneous complete recovery. T-LOC – all cases of transient loss of consciousness regardless of the pathophysiological mechanism Transient loss of consciousness Global cerebral hypoperfusion = circulatory cause Rapid onset Short duration Spontaneous complete recovery ESC Guidelines for the diagnosis and management of syncope (version 2009): Moya et al. Eur Heart J, 2009.
: Moya et al. Eur Heart J,")
3
Significance, epidemiology Risk of fall and trauma A warning signal of sudden death Mostly benign in young A common complaint – 3% of emergency visits A fraction of patients see a doctor Bimodal age distribution

4
Prognosis, significance of syncope management and diagnostics Soteriades et al. N Eng J Med, 2003.

5
www.escardio.org/guidelines

6
Classification of syncope Reflex syncope Vasovagal Situational Carotid sinus hypersensitivity Atypical forms Syncope from ortostatic hypotension Primary ANF Secondary ANF Drug-induced Volume depletion Cardiac syncope Arrhythmia as a cause Structural heart disease

7
www.escardio.org/guidelines
8
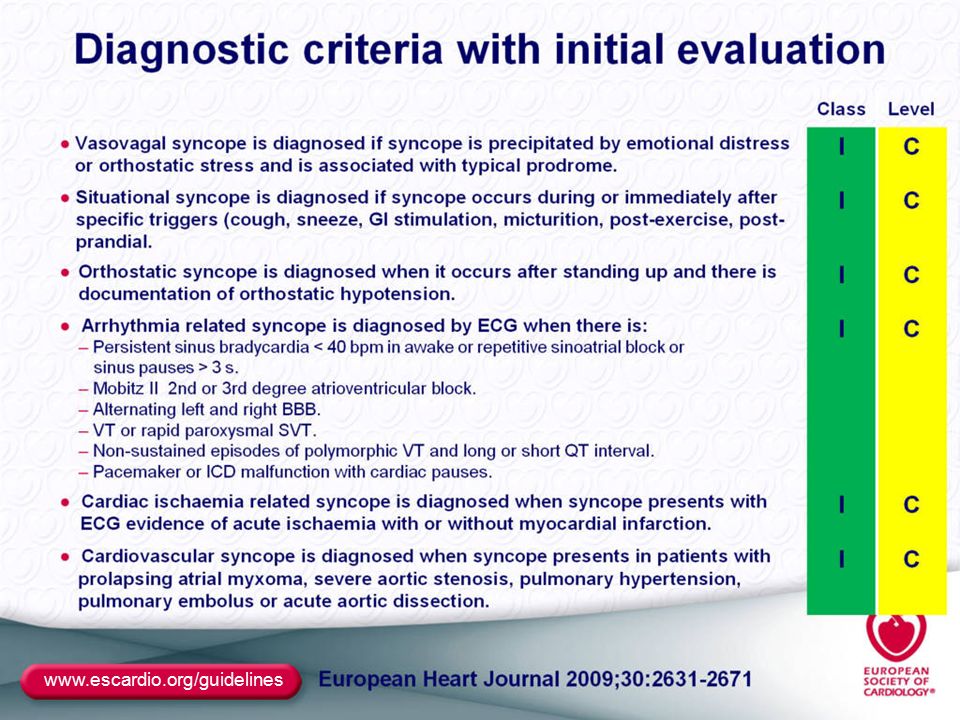
Initial diagnostic work-up A thorough history What preceded syncope, prodromes, eyewitness report, symptoms after syncope Personal and family history, medication, recurrent syncope? Physical exam BP supine and standing 5 min. supine, 1st and 3rd min. standing ECG

9
Initial evaluation – key questions Syncope? Is it syncope? Diagnosis? Was diagnosis made? Risk? Is there a high-risk profile for casrdiovascular diseases or high sudden-death risk?

10
Initial evaluation Suspected syncopeSyncope Diagnosis made Diagnosis uncertain High-risk Admitt, diagnose, treat Low risk, recurrent Diagnose, treat? Low-risk, sporadic No further work-up NO Consider other diagnosis

11
www.escardio.org/guidelines
12
Initial evaluation Risk startification Structural heart disease CHD (previous MI), heart failure, aortic stenosis, HCM… Clinical or ECG signs suggestive of arrhytmic etiology Syncope while supine, exercising, palpitations Family history of sudden death Bifascicular block, nsVT, susp. SSS, preexcitation, ↑ QTc, Brugada, susp. ARVC Age >40 + recurrent syncope (50% arrhythmia) Severe comorbidities Anemia, ion dysbalance
 Severe comorbidities Anemia, ion dysbalance.")
13
Further evaluation Diagnostic methods Carotid massage Pause > 3s, BP drop > 50 mmHg Unknown cause in pts. > 40 yrs Tilt test Reflex syncope - cardioinhibitory, vasodepresoric and mixed reaction X ortostatic hypotension Indicated in suspected reflex syncope, unknown etiology, susp. OH, difdg. of falls, pseudosyncope…

14
Further evaluation Diagnostic methods ECG monitoring In-hospital monitoring High-risk pts. Holter ECG (24h, 48h, 7d) frequent syncope/presyncope Implantable/external loop recorder (ILR) Recurrent syncope of unknown etiology, therapy- resistant epilepsy, susp. arrhytmic cause Arrhythmia during syncope or occurrence of severe arrhythmia make diagnosis, syncope with no ECG changes rule out arrhythmic cause
 frequent syncope/presyncope Implantable/external loop recorder (ILR) Recurrent syncope of unknown etiology, therapy- resistant epilepsy, susp. arrhytmic cause Arrhythmia during syncope or occurrence of severe arrhythmia make diagnosis, syncope with no ECG changes rule out arrhythmic cause.")
15
Further evaluation Diagnostic methods Electrophysiological exam Specific indications, high suspicion not confirmed non-invasively Echocardiography Risk stratification, structural heart disease Stress test Psychiatric evaluation Neurological evaluation

16
www.escardio.org/guidelines
17
Take home messages Not every LOC is a syncope Thorough history is the cornerstone Initial evaluation makes diagnosis 25- 40%, risk-stratification in the rest There is plenty of diagnostic methos, use them wisely

18
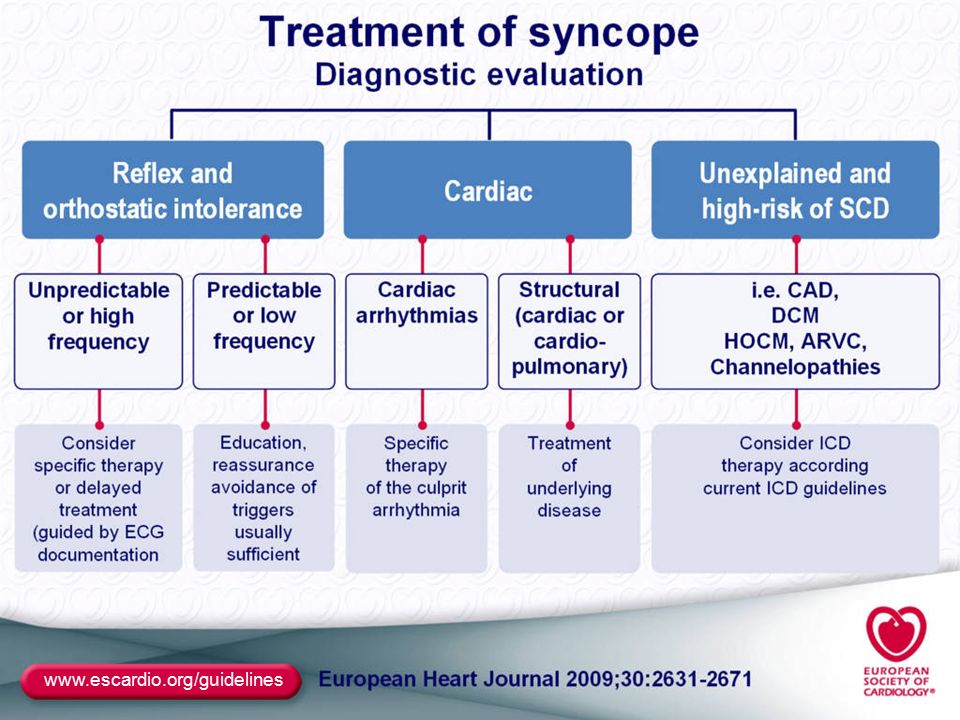
Therapy Indications for permanent pacing SSS + ECG correlated symptoms SSS + abnormal CSNRT Asymptomatic pauses >6s (SSS/AVB) AVB II Mobitz II, AVB III BBB + abnormal HV conduction Alternating BBB BBB + unexplained syncope – risk/ILR Reflex cardio-inhibitory – „ultimum refugium“ Syncope due to hypersensitive carotid sinus
 AVB II Mobitz II, AVB III BBB + abnormal HV conduction Alternating BBB BBB + unexplained syncope – risk/ILR Reflex cardio-inhibitory – „ultimum refugium Syncope due to hypersensitive carotid sinus")
Similar presentations


 -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2 nd /3 rd heart block -Exercise.>")













>")


