Download presentation
Presentation is loading. Please wait.

1
Some Childhood infectious diseases Dr E Boait 12/8/10

2
Parvovirus B19/Slapped cheek/fifth disease Roseola infantum Hand, foot and mouth disease Scarlet fever Kawasaki disease Rubella (Management of exposure to rash in pregnancy)
")
3
Parvovirus B19 - presentation The majority of patients with Parvovirus B19 infection are either asymptomatic or exhibit mild, nonspecific, cold like symptoms. Clinical conditions associated with the infection include: erythema infectiosum (also called fifth disease and slapped cheek syndrome) –most common clinical presentation of Parvovirus B19 infection –seen in children between the ages of 6 to 14 years, a less-pronounced rash may be seen in adults –after an incubation period of 13 to 18 days, a prodrome of mild fever with a sore throat, coryza, headache and gastrointestinal disturbance (nausea) may be observed which lasts for up to 4 days –during the first stage, erythema of the cheeks (“slapped-cheek” rash) can be seen with circumoral pallor –the second stage of the rash occurs after one to four days and presents as a maculopapular rash in the extremities and trunk a lacy, reticular pattern may be seen caused by the central clearing of the rash by the second day, it usually has spread to involve the proximal arms and extensor surfaces of the legs later, it may extend to the flexor surfaces and the trunk, and rarely, the palms and soles –exposure to sunlight and heat may cause the rash to fade and reappear –it usually disappears within 7 – 10 days
 –most common clinical presentation of Parvovirus B19 infection –seen in children between the ages of 6 to 14 years, a less-pronounced rash may be seen in adults –after an incubation period of 13 to 18 days, a prodrome of mild fever with a sore throat, coryza, headache and gastrointestinal disturbance (nausea) may be observed which lasts for up to 4 days –during the first stage, erythema of the cheeks ( slapped-cheek rash) can be seen with circumoral pallor –the second stage of the rash occurs after one to four days and presents as a maculopapular rash in the extremities and trunk a lacy, reticular pattern may be seen caused by the central clearing of the rash by the second day, it usually has spread to involve the proximal arms and extensor surfaces of the legs later, it may extend to the flexor surfaces and the trunk, and rarely, the palms and soles –exposure to sunlight and heat may cause the rash to fade and reappear –it usually disappears within 7 – 10 days.")
5
Parvovirus B19 – presentation continued arthropathy –may present as a complication of erythema infectiosum or as a primary presentation of the infection itself –more common in adolescents and adults (upto 60% of infected patients might be affected) –presentation of arthropathy differ in adults when compared to children in adults – presents as symmetric and polyarticular arthropathy with involvement of the proximal interphalangeal and meta-carpophalangeal joints, knees, wrists, and ankles are affected less often, resolves within three weeks, in children – it can be symmetric or asymmetric with knees (82% of patients) and ankles usually affected
 –presentation of arthropathy differ in adults when compared to children in adults – presents as symmetric and polyarticular arthropathy with involvement of the proximal interphalangeal and meta-carpophalangeal joints, knees, wrists, and ankles are affected less often, resolves within three weeks, in children – it can be symmetric or asymmetric with knees (82% of patients) and ankles usually affected")
6
Parvovirus B19 differentials rubella measles infection roseola infantum scarlet fever erysipelas drug hypersensitivity SLE

7
Parvovirus B19 Management –There is no specific treatment for parvovirus B19 infection. However when managing patients with the infection, host factors such as underlying diseases and immunodeficiency status should be taken into account –No recommendation for school exclusion once child well –if possible parvovirus infection has occurred in pregnency then: check parvovirus serology if positive test in the first 20 weeks of pregnancy, then regular ultrasound scans are indicated to monitor fetal growth and development

8
Roseola Infantum - presentation Roseola is a benign condition is most probably due to infection with human herpes virus type 6. It is most common in infants between 6 and 18 months; the clinical condition does not occur in adults. After an incubation period of 10 to 15 days clinical features include: pyrexia mild pharyngitis lymphadenopathy Temperature returns to normal after 3-4 days, accompanied by the appearance of a rose-pink macular rash. Initially, involving the trunk, the rash may spread to the face and extremities. The exanthem is prominent over the thighs and buttocks, where each macule is sometimes surrounded by a fine halo. It disappears within two days without desquamation or pigmentation. Uncommonly, the child develops febrile convulsions. Otherwise, there is full recovery.

10
Roseola infantum differentials This includes measles and rubella. measles –catarrhal stage where there may be cough, coryza; also may be conjunctivitis and the presence of Koplik spots –exanthematous stage - occurs 3 to 5 days later; initial rash behind the ears and then on the body; maculopapular rash that becomes confluent; fading by third day rubella –headache –pink macular rash, which may be absent in young children. It appears one or two days after the start of the illness, fading within four days, leaving neither staining or desquamation –fever –cervical lymphadenopathy - especially post-auricular and sub-occipital nodes –grittiness of eyes and suffusion of conjunctivae

11
Hand foot and mouth disease Febrile illness of young children characterised by the development of vesicular exanthem on the oral mucosa and a papulovesicular exanthema on the distal extremities and buttocks. frequently seen in children under the age of ten but adult cases are not unusual peaks during summer and early autumn months outbreaks are frequently seen in groups of children e.g. – in a nursery school incubation period is 3-5 days. It is usually caused by viruses belonging to human enteroviruses A (HEVA), especially coxsackie viruses A16 which in majority of patients causes a mild self limiting illness.
, especially coxsackie viruses A16 which in majority of patients causes a mild self limiting illness..")
13
Hand foot and mouth management Transmission of the disease occurs through: direct contact with nose and throat discharges aerosol spread e.g. coughing and sneezing direct contact with fluid from blisters direct contact with the stool of an infected persons from mother to fetus – if infection occurs late in the pregnancy An infected person who is asymptomatic may shed the virus in feces and saliva for several weeks There is no specific treatment for the condition. Only symptomatic treatment is necessary. Patients should be informed that the disease is not connected to foot and mouth disease of animals and transmission does not occur to or from pets or other animals. Infected persons develop immunity to the specific virus but recurrence of the disease may be caused by a different member of the enterovirus group. SCHOOL EXCLUSION -infected children should be kept away from school while they are unwell. The child should not be kept away from school till the last blister disappears, providing the child is well

14
Scarlet fever Scarlet fever is primarily a childhood disease and is commonly seen in children between the ages of two and eight years. It is a highly contagious infection. Transmission occurs when bacteria (present in an infected person’s saliva or mucous) is spread by aerosol - sneezing, coughing, or breathing out comes into direct contact with an uninfected person Although scarlet fever is seen after streptococcal sore throat in a majority of the patients, it may also occur following burns or an infected wound. Invasive group A streptococcal disease and scarlet fever are notifiable disease under the Health Protection (Notification) Regulations 2010. This disease has an incubation period of two to four days.
 is spread by aerosol - sneezing, coughing, or breathing out comes into direct contact with an uninfected person Although scarlet fever is seen after streptococcal sore throat in a majority of the patients, it may also occur following burns or an infected wound. Invasive group A streptococcal disease and scarlet fever are notifiable disease under the Health Protection (Notification) Regulations This disease has an incubation period of two to four days..")
15
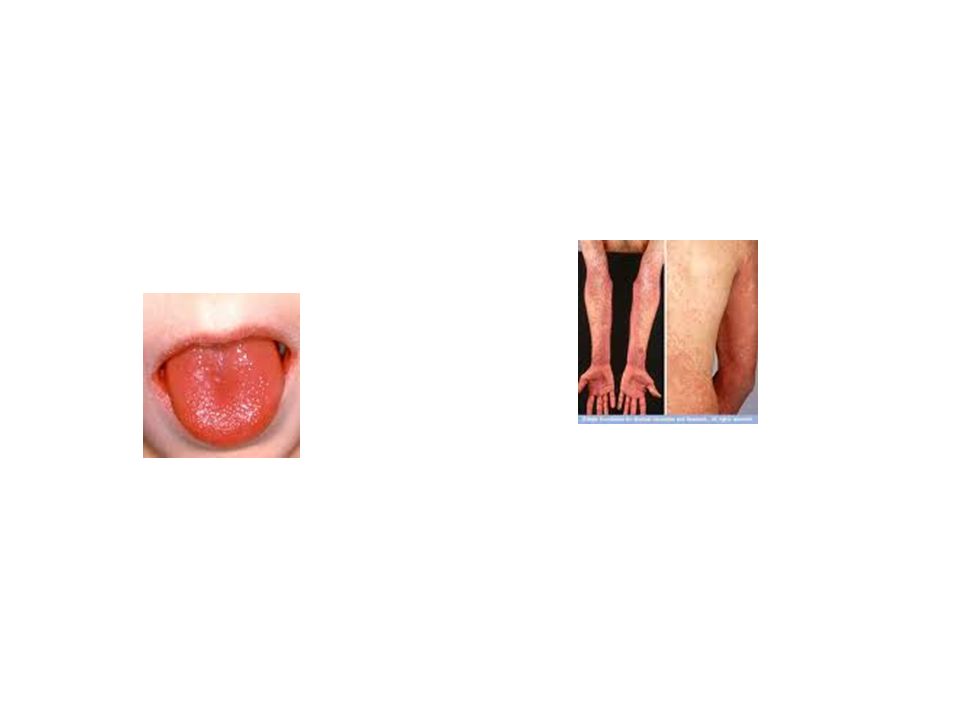
Scarlet fever - presentation typically the fist symptoms of scarlet fever develops after an incubation period of 2 to 4 days and includes: –tonsillitis –fever (usually above 38.3º C/101º F or higher) –headache, malaise, nausea and vomiting characteristic fine red rash –develops twelve to forty eight hours after the onset of these symptoms –first appears on the chest and stomach and later covers the entire body and limbs and consists of many small papules on diffuse erythema that blanches on pressure –often more marked over the skinfolds where transverse lines containing tiny petichae may be seen –area around the mouth is spared –the skin may feel rough like sandpaper –the rash lasts for a period of two to three days, after which desquamation occurs that is most prominent on the soles of the feet and the palms of the hands examination of the throat generally reveals that the pharynx is diffusely reddened, with enlarged and red tonsils covered with a white exudate. The tongue may be initially furred with enlarged papillae - an appearance described as a 'white strawberry tongue', lost after two or three days to become strawberry tongue. usually there is enlargement of regional lymph nodes flushed red face with paleness around the mouth note that although, in general the tonsil or pharynx is the site of infection, occasionally other foci e.g. surgical wounds may occur

17
Scarlet fever complications Complications are rarely seen in scarlet fever. During the early stages of the infections there is a small risk of acquiring the following: middle ear disease throat abscess sinusitis pneumonia meningitis osteomyelitis septic arthritis Late complications develop two to three weeks after the infection has subsided and include: rheumatic fever post-streptococcal glomerulonephritis

18
Scarlet fever - diagnosis Diagnosis is usually clear from the clinical presentation. The diagnosis is confirmed from cultures of throat swabs. In some cases a blood test may be necessary. Antistreptolysin O titres may be helpful

19
Scarlet fever - management The treatment of choice is penicillin and this leads to the rapid resolution of symptoms in about 24 hours. A ten day course of treatment is necessary to eradicate the streptococci Erythromycin is an alternative antibiotic for this condition in penicillin - allergic patients Untreated patients may be infectious for up to 2- 3 weeks after the symptoms appear Paracetamol or ibuprofen can be given to patients for symptomatic relief. Patients should be advised about rest and hydration with plenty of fluids (1). Inform about the following to patients: infection usually clears up after a week and it is no longer a serious illness antibiotics are necessary to speed up recovery and to avoid complications to take the full course of antibiotics given by the general practitioner avoid attending school or work for a minimum of 24 hours after starting treatment wash hands frequently avoid sharing eating utensils, clothes, bedding and towels with an infected person washing or proper disposing of the tissues or handkerchiefs used by an infected person
. Inform about the following to patients: infection usually clears up after a week and it is no longer a serious illness antibiotics are necessary to speed up recovery and to avoid complications to take the full course of antibiotics given by the general practitioner avoid attending school or work for a minimum of 24 hours after starting treatment wash hands frequently avoid sharing eating utensils, clothes, bedding and towels with an infected person washing or proper disposing of the tissues or handkerchiefs used by an infected person.")
20
Kawasaki disease A febrile systemic vasculitis predominantly affecting children under age 5. The most serious complication is coronary arteritis and aneurysm formation which occurs in 1/3 untreated patients. The reported incidences of Kawasaki disease are: 3 per 100 000 in the UK 10 per 100 000 in the US 85 per 100 000 in Japan In Japan the mortality is less than 0.1%, in the UK the mortality is 3.7%. NICE note that clinical features suggestive of Kawasaki disease, in a child less than 5 years, are: fever for more than 5 days and at least four of the following: –bilateral conjunctival injection –change in mucous membranes –change in the extremities –polymorphous rash –cervical lymphadenopathy

22
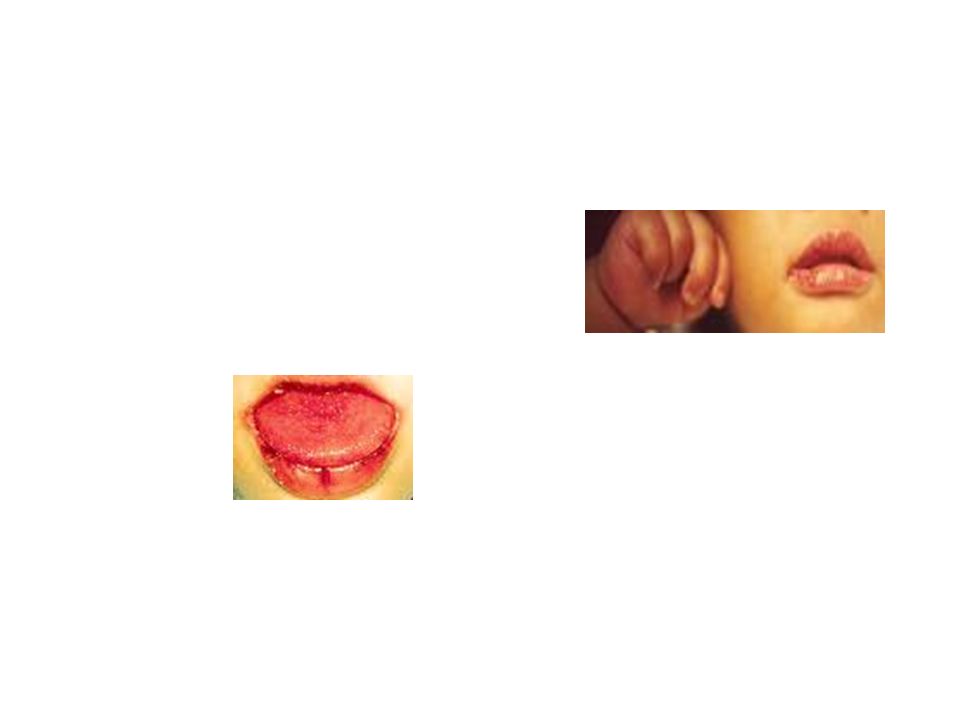
Kawasaki disease - Diagnosis A diagnosis of Kawasaki disease can be made if five out six of the major features are present. If only four of the major features are found then the demonstration of coronary aneurysms confirms the diagnosis. Major features include: fever more than 5 days bilateral non-purulent conjunctival congestion dry, fissured mouth and lips and a strawberry red tongue acute, non-purulent cervical lymphadenopathy in more than 60% polymorphous exanthema for days 1 to 5 of the fever; typically there are no vesicles or crusts changes in the extremeties: –reddening and oedema of the hands and feet occurs on days 2 to 5 of the fever –desquamation of affected skin from days 10 to 15

23
Kawasaki disease - differentials staphylococcal infection: –scalded skin syndrome –toxic shock syndrome streptococcal infection: –scarlet fever –toxic shock-like syndrome –Kawasaki disease is not excluded by the culture of a group A streptococcus from the throat measles leptospirosis rickettsial disease Stevens-Johnson syndrome drug reaction juvenile rheumatoid arthritis

24
Kawasaki disease - investigations The changes are non specific: mild to moderate normochromic normocytic anaemia polymorph leucocytosis ESR and CRP are almost always high by the second week of illness thrombocytosis

25
Kawasaki disease - treatment Consult expert advice. If the diagnosis is made within 10 days of onset: intravenous immunoglobulin aspirin: e.g. 30 mg/kg/day in divided doses for 2 weeks Thereafter: aspirin, e.g. 3-5 mg/kg/day until the 6-8 week check echocardiograph if coronary aneurysms are detected then aspirin should be continued indefinitely Intravenous immunoglobulin may be given to patients diagnosed more than 10 days after onset if there is evidence of ongoing inflammation. A second course of immunoglobulin may be given for resistant or recurrent disease.

26
Kawasaki disease - nb The aetiology of this condition is unknown. There is evidence that Kawasaki disease has an infectious aetiology: a retrovirus has been proposed recent evidence points to the role of toxin- producing staphylococci or streptococci; specifically, superantigens similar to the toxic shock syndrome toxin may be important

27
Rubella Symptoms Swollen glands, usually behind the ears and at the back of the neck. Sometimes glands in other parts of the body swell. The glands gradually go back to normal over a week or so. A spotty, pink-red rash develops any time up to seven days after the glands swell. The rash usually starts behind the ears, then spreads to the face and neck and then spreads to the rest of the body. The rash lasts 3-5 days before fading. A mild fever, cold, cough and sore throat are common. Sore red eyes (conjunctivitis) may develop for a few days. Joint pains, like a mild arthritis, may develop for a week or so. This is less common in children, but is quite common in adults with rubella. Other symptoms may include fever, tiredness and headache. Bleeding disorders and brain inflammation (encephalitis) are rare complications. The incubation period is 14 - 21 days and the period of infectivity from one week before until four days after the onset of rash
 may develop for a few days. Joint pains, like a mild arthritis, may develop for a week or so. This is less common in children, but is quite common in adults with rubella. Other symptoms may include fever, tiredness and headache. Bleeding disorders and brain inflammation (encephalitis) are rare complications. The incubation period is days and the period of infectivity from one week before until four days after the onset of rash.")
28
Rubella & Pregnancy Rubella is serious for pregnant women, because if they are infected their unborn baby may develop abnormalities. Fetal defects include mental handicap, cataract, deafness, cardiac abnormalities, retardation of intra-uterine growth and inflammatory lesions of brain, liver, lungs and bone marrow. Risk of intrauterine transmission during different stages of pregnancy less than 11 weeks 90% 11-16 weeks 20% 16-20 weeks Minimal risk of deafness only >20 weeks No increased risk

Similar presentations





 Lawrence Pike.>")

















