Download presentation
Presentation is loading. Please wait.

3
At the end of this session you will be able to: Define Evidence Based Practice Identify reasons for Promoting Evidence Based Practice Identify nursing practice that might benefit from the use of evidence Appreciate different forms of evidence

5
Sackett et al (1996) define EBP as ‘ the conscientious, explicit and judicious use of current best evidence in making nursing decisions about the care of individual patients’ Carnwell defines EBP as ‘[the] systematic search for, and appraisal of, best evidence in order to make clinical decisions that might require changes in current practice, while taking into account the individual needs of the patient.’ She adds: ‘Best evidence might be defined as that which is valid and relevant to the patient.’ (Carnwell, 2001)
![Sackett et al (1996) define EBP as ‘ the conscientious, explicit and judicious use of current best evidence in making nursing decisions about the care of individual patients’ Carnwell defines EBP as ‘[the] systematic search for, and appraisal of, best evidence in order to make clinical decisions that might require changes in current practice, while taking into account the individual needs of the patient.’ She adds: ‘Best evidence might be defined as that which is valid and relevant to the patient.’ (Carnwell, 2001)](http://images.slideplayer.com/33/8169208/slides/slide_5.jpg "Sackett et al (1996) define EBP as ‘ the conscientious, explicit and judicious use of current best evidence in making nursing decisions about the care of individual patients’ Carnwell defines EBP as ‘[the] systematic search for, and appraisal of, best evidence in order to make clinical decisions that might require changes in current practice, while taking into account the individual needs of the patient.’ She adds: ‘Best evidence might be defined as that which is valid and relevant to the patient.’ (Carnwell, 2001)")
6
‘Clinical decisions should […] be informed by up- to-date, relevant and robust evidence rather than outdated primary training or over interpretation of individual patient experiences (Donald & Greenhalgh, 2000; Sackett et al, 2000) Use of best evidence is thus important.
![‘Clinical decisions should […] be informed by up- to-date, relevant and robust evidence rather than outdated primary training or over interpretation of individual patient experiences (Donald & Greenhalgh, 2000; Sackett et al, 2000) Use of best evidence is thus important.](http://images.slideplayer.com/33/8169208/slides/slide_6.jpg "‘Clinical decisions should […] be informed by up- to-date, relevant and robust evidence rather than outdated primary training or over interpretation of individual patient experiences (Donald & Greenhalgh, 2000; Sackett et al, 2000) Use of best evidence is thus important.")
8
What areas of nursing practice might we want to ask EBP questions about? Discuss this with a partner.

9
Study Design General categories Observational Experimental Cross sectional Case control study Cohort study Community trials Clinical Trials

10
Descriptive Studies Today Cross sectional (Prevalence) Retrospective (Case Control) Prospective (Incidence) Historical Prospective Past Future
 Retrospective (Case Control) Prospective (Incidence) Historical Prospective Past Future")
11
Descriptive Study: Advantages Cross sectional Retrospective Prospective Quick Cheap Large sample Attributes Prevalence Public health Complete Risk factors Quality data Natural history Incidence Etiology Rare disease Cheap Uses records Small sample Quick Risk factors

12
It is also called prevalence study. It is conduct at one point of time and try to concurrently evaluate exposure (risk factors ) and outcome (diseases) in a population.
 and outcome (diseases) in a population..")
14
Step 1--Aim of the study and what type of study method to be applied. Step 2--Study population Step 3--Sample size calculation and sampling method

15
1. Predicted prevalence 2. d (admissible error) 3. N=400* Q/P (Q=1-p) for categorical data 4. N=4s 2 /d 2 ( for quantitative data)
 for categorical data 4. N=4s 2 /d 2 ( for quantitative data).")
16
Questionnaire (include every information of interest) Risk factors Investigators
 Risk factors Investigators")
17
Cross-sectional Study Design Selection of study population -target appropriate population -acquire a “representative” sample -Sampling definitions -sampling unit: person, patient, household -Sampling frame: list of all sampling units -Sample: all sampling units chosen rule: each unit has the same probability of being chosen

19
Simple random sampling Systematic sampling Stratified sampling Cluster sampling Multistage sampling

20
Prevalence of Metabolic Syndrome:8814 US Adults Age 20+ NHANES 1988-94, JAMA 2002 287

21
Prevalence of Cardiovascular Disease in Women with Diabetes NHIS 1997-9 MMWR 2001 50:948-54

22
Cross-sectional Studies Analysis: Study sample Cross-sectional collection of data Exposed w/disease “a” Exposed w/o disease “b” No exposure w/disease “c” No exposure w/o disease “d”

23
Cross-sectional Studies Analysis: Study sample Cross-sectional collection of data Exposed w/disease “a” Exposed w/o disease “b” No exposure w/disease “c” No exposure w/o disease “d” ab cd Exp no exp Dis no dis Compare prevalence in exposed to prevalence in non- exposed Prevalence ratio = a / a+b c / c+d

24
Cross-sectional Studies Common methods of Analysis: -t-tests -rate comparisons -categorical data analysis -descriptive analysis -comparisons can be by age, sex, or date, year

25
Description of the distribution of the disease in a population Burden of disease in a population (community) Easy and economical to carry out Test association between disease and risk factors Developing a etiological hypothesis Assessment of health services, health care needs of population
 Easy and economical to carry out Test association between disease and risk factors Developing a etiological hypothesis Assessment of health services, health care needs of population")
26
Temporal or time sequence of risk factor and disease is not available Do not provide information of natural history of disease and aetiology Provide no information about incidence

27
Good Precision Poor Accuracy Poor Precision Good Accuracy Good Precision Good Accuracy Poor Precision Poor Accuracy Precision and Accuracy Hulley & Cummings, Designing Clinical Research, 1988.

28
Population reality Disease No disease Test results Positive Negative True Positive True Negative False Negative False Positive Sensitivity= Specificity= TP ability to identify TP + FN those with disease TN ability to identify TN + FP those w/o disease

29
True characteristics in the population Disease No disease Results of screening Positive Negative 80 800 20 100 Sensitivity = = 80% Specificity = = 89% 80 100 800 900 Example: Pop: 1000 w/dis: 100 w/o dis: 900 100 9001000 820 180 Total

30
True positive (TP)= Have disease and have positive test False positive (FP) = No disease, but have positive test False negative (FN) = Have disease, but have negative test True negative (TN) = No disease and have negative test With Disease W/O Disease Population Test Results Positive Negative
= Have disease and have positive test False positive (FP) = No disease, but have positive test False negative (FN) = Have disease, but have negative test True negative (TN) = No disease and have negative test With Disease W/O Disease Population Test Results Positive Negative")
31
1. If the test results are positive in this patient, what is the probability that this patient has the disease? 2. What proportion of patients who test positive actually have the disease in question?

32
Positive Predictive Value of a Test: PPV = Negative Predictive value: With negative result, what is the probability that the patient does not have the disease? NPV = True positive Total positive True Negative Total negative

33
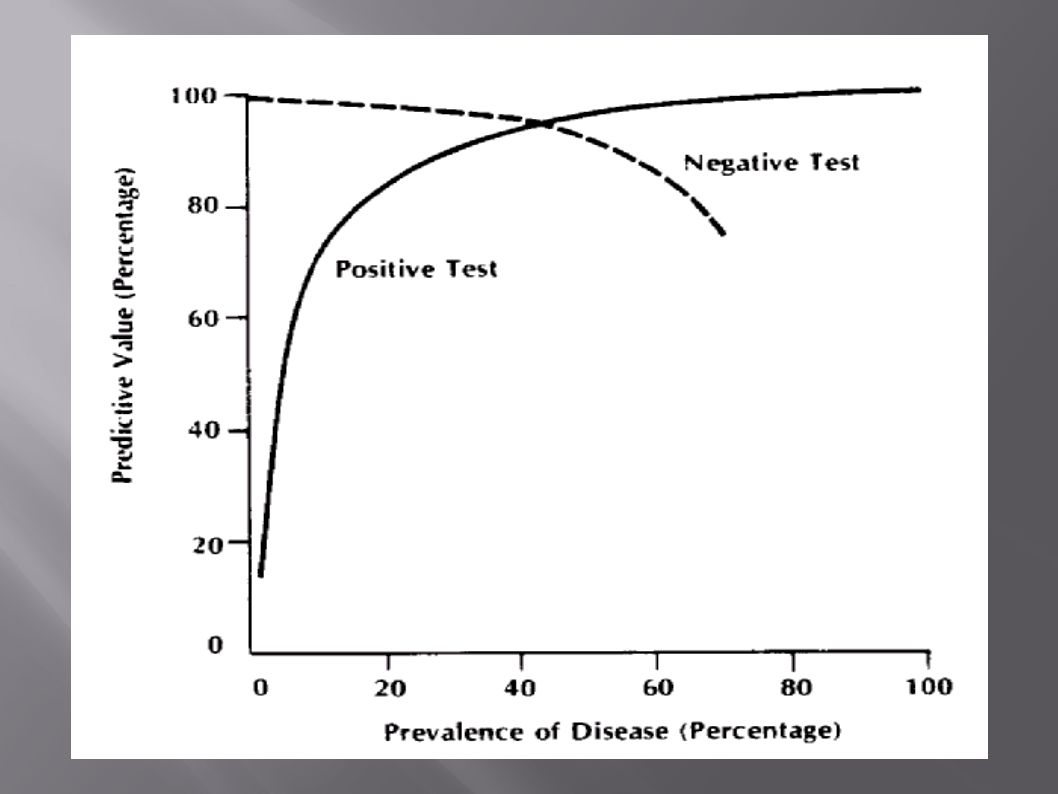
Relationship between Predictive Value and Prevalence Predictive value improves as prevalence increases. Relationship between Predictive Value and Specificity Predictive value improves as specificity of a screening test increases.

35
Screening for Type 2 Diabetes: Strong Heart Study Wang, Diabetes Care, 2002.

36
Cross-sectional studies are the only way to determine prevalence for public health planning, screening rationale (and big pharma) Sampling decisions are the hardest part Look for etiologic associations (7 Countries Study) Screening decisions are based on prevalence, natural history and severity of disease. Need proven intervention, reasonable sensitivity & specificity of test, & low cost (includes follow-up). Remember competing costs for health care resources… Get enough info to start a cohort study…
. Remember competing costs for health care resources… Get enough info to start a cohort study….")
39
You might ask questions about a range of categories of practice: 1. Assessment – how to properly gather and interpret findings? 2. Causes of the problem – how to identify them? 3. Deciding what the problem is – where the symptoms/signs indicate a range of possible problems how do you decide which is most likely? 4. How to select and interpret tests used to identify problems and to monitor patient progress? 5. How to estimate the likely clinical progression of a condition/illness and any likely complications? 6. How to select interventions that do more good than harm and that are worth the effort and cost of doing them? 7. How to reduce the chance of the problem reoccurring or how to promote health? 8. How to keep up to date; improve your skills; and run a more effective/efficient nursing team? 9. How best to understand the perceptions of individuals and groups e.g. service users and carers Adapted from Sackett et al (2007) (http://www.mdx.ac.uk/www/rctsh/ebp/question.htm - Accessed 22/11/07)
 ( - Accessed 22/11/07).")
40
With a partner make a list of reasons why we should use evidence to underpin nursing care

41
Ensures patient/clients receive the care that fits their needs Facilitates sound decision making and makes it more explicit Minimises risk to the patient/client so that benefits outweigh harm Provides the nurse with the skills and knowledge to evaluate healthcare literature and practice Exposes gaps in knowledge and conflicts in evidence

42
In the context of evidence based practice this is research published in professional and academic journals and systematic reviews of research found in databases of evidence (such as Cochrane). ‘ Knowledge derived from a variety of sources that has been found to be credible’ (Higgs & Jones 2000)
.")
43
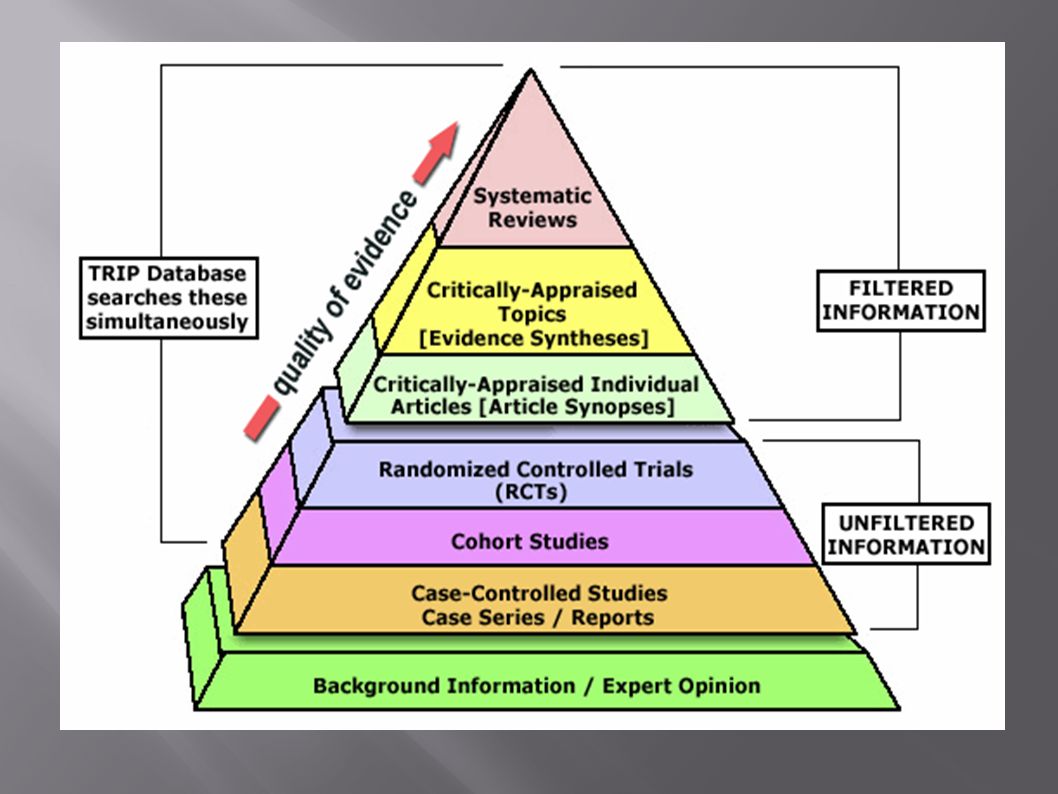
¶ At least one systematic review of multiple, well designed randomised controlled trials (RCT’s) · At least one properly designed RCT of appropriate size ¸ Well designed trials without randomisation, single group pre-post, cohort, or matched case controlled studies ¹ Well designed, non-experimental studies from more than one centre or research group º Opinions of respected authorities, based on clinical evidence, descriptive studies or reports of expert committees (Source: Muir Gray, 1997)
 · At least one properly designed RCT of appropriate size ¸ Well designed trials without randomisation, single group pre-post, cohort, or matched case controlled studies ¹ Well designed, non-experimental studies from more than one centre or research group º Opinions of respected authorities, based on clinical evidence, descriptive studies or reports of expert committees (Source: Muir Gray, 1997)")
44
Evidence based on experiences (professional or personal) Evidence gathered from patients/clients and/or carers. Evidence based theory that is not research based. Le May (1999) ‘Evidence-based practice’ Nursing Times, Monographs, 1;2.
 ‘Evidence-based practice’ Nursing Times, Monographs, 1;2..")
47
An approach to clinical practice A way to keep current with new developments N. MacIntyre, 2005

48
… a methodological approach to clinical practice where evidence is used to inform decision-making about making a diagnosis (or interpreting a diagnostic test), selecting an intervention, or evaluating prognostic indicators Centre for Evidence-Based Medicine
, selecting an intervention, or evaluating prognostic indicators Centre for Evidence-Based Medicine")
49
… an approach to health care practice in which the clinician is aware of the evidence that bears on her clinical practice, and the strength of that evidence Health Information Research Unit, McMaster, 2002

50
… an approach to decision making in which the clinician uses the best evidence available, in consultation with patient, to decide upon the option which suits that patient best J. A. Muir Gray, 1997

51
D. Sackett et al, 1996 What is Evidence-Based Practice? Evidence based health care is the integration of individual clinical expertise with the best available external clinical evidence and the values and expectations of the patient

52
Involves life-long, self-directed, problem-based learning Involves exploring the relationship between clinical reasoning and research evidence Involves practice N. MacIntyre, 2005

53
Do nothing … and get out of date Depend solely on courses/conferences Choose the main professional journal(s) and read them cover to cover every month Learn how to find and appraise the evidence to answer questions that come from clinical practice N. MacIntyre, 2005

54
Knowledge Standard Each nurse possesses, through basic education and continuing learning, knowledge relevant to her/his professional practice Ontario College of Nurses, 2002

55
Knowledge Standard Indicators Providing a theoretical and/or evidence-based rationale for all decisions Understanding the knowledge required to meet the needs of complex clients Knowing where/how to access learning resources when necessary Ontario College of Nurses, 2002

56
Knowledge Standard Indicators Seeking and reviewing research in nursing, health sciences and related disciplines Using research to inform practice/professional service Ontario College of Nurses, 2002

58
Knowledge Application Standard Each nurse continually improves the application of professional knowledge Ontario College of Nurses, 2002

59
Knowledge Application Standard Indicators Ensuring practice is based in theory and evidence and meets all relevant standards/guidelines Assessing/describing the client situation using a theory, framework or evidence-based tool Managing multiple nursing interventions simultaneously Ontario College of Nurses, 2002

60
Knowledge Application Standard Indicators Evaluating/describing the outcome of specific interventions and modifying the plan/approach Integrating research findings into professional service and practice Ontario College of Nurses, 2002

61
Copyright ©2004 BMJ Publishing Group Ltd. Thompson, C. et al. Evid Based Nurs 2004;7:68-72 The cognitive continuum.

62
Define the Question Identify Question ~ Search and Screen Literature ~ Refine Question Collect the Evidence Critically Appraise the Evidence for Validity and Relevance N. McKibbon, 1999

63
Integrate the Evidence and Patient Factors Make & Carry Out the Decision Evaluate the Process Results ~ Self-reflection N. McKibbon, 1999

64
A clinical question should incorporate at least three elements Patient Age, sex, ethnicity, etc. Condition, diseases, general health status Intervention Education, diagnostics, treatment plan, self-care, etc.

66
Do nurse led tobacco cessation interventions result in decreased smoking rates after hospital admission for coronary heart disease?

67
PATIENT (Adult) coronary heart patients Smokers Discharged from hospital INTERVENTION Nurse led tobacco cessation programmes
 coronary heart patients Smokers Discharged from hospital INTERVENTION Nurse led tobacco cessation programmes")
69
COMPARISON (Non-nurse led tobacco cessation programmes Self-administered, non-nurse administered, etc.) No comparison OUTCOME Lower rates of tobacco use among Patient group
 No comparison OUTCOME Lower rates of tobacco use among Patient group")
70
Not all questions are of a clinical nature Intervention can be interpreted very broadly

71
SUNY Downstate Medical Center, 2003

72
“ Important medical questions are typically studied more than once, often by different research teams in different locations. A meta-analysis combines results from different studies, hopefully averaging out any differences caused by random change or local variation and getting at something close to the real truth. In general a meta-analysis, if you can find one, will be a better guide to practice than an individual article. ” SUNY Downstate Medical Center, 2003

73
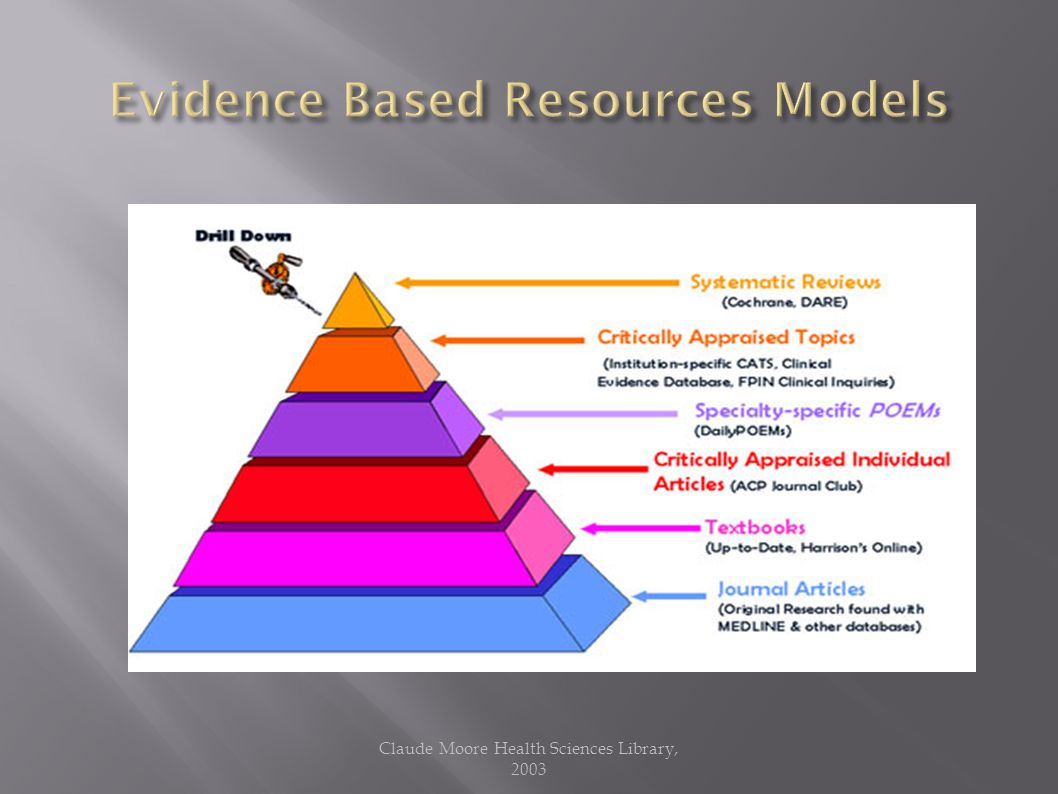
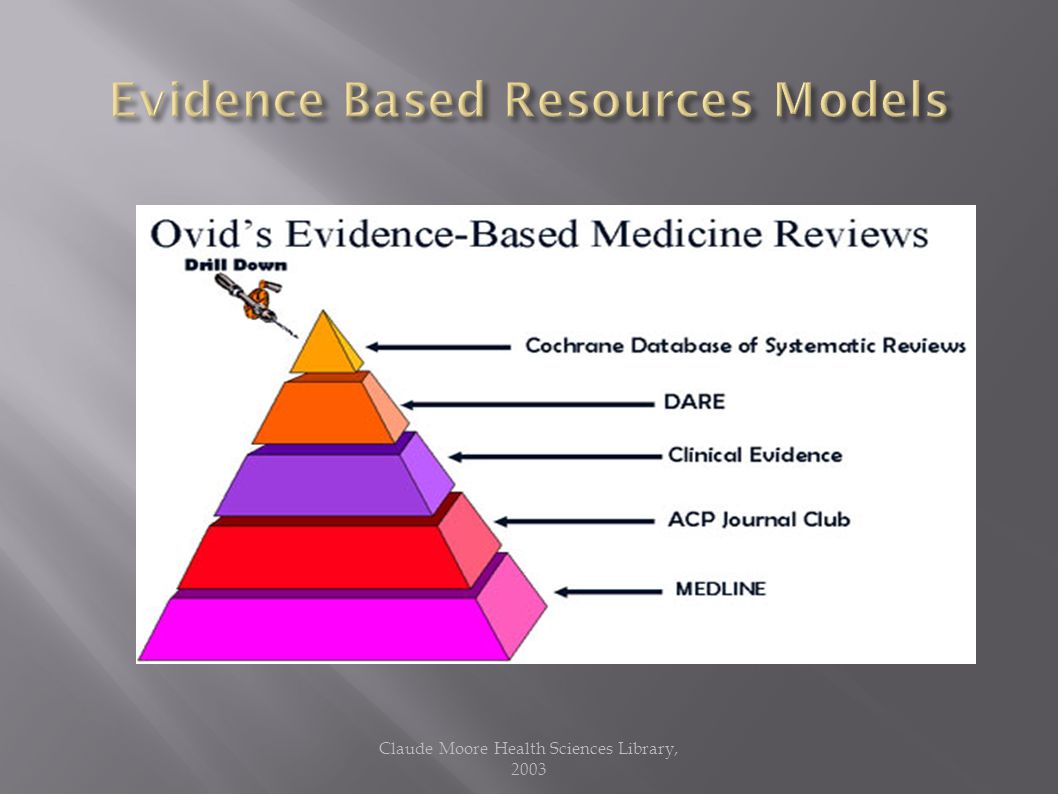
Usefulness = Relevance x Validity Work Claude Moore Health Sciences Library, 2003

Similar presentations