Download presentation
Presentation is loading. Please wait.

1
Primary Care Trigger Tool 29 September 2009 LHB and Trust CEOs 12 May 2009 A Trigger Tool for Primary Care Tuesday 29 September 2009 Learning Session 3 William Whitehead and Adam Southan

2
Primary Care Trigger Tool 29 September 2009 What do we know? Healthcare systems are not safe Errors harm large numbers of patients Many errors are avoidable Many patients get worse without an error occurring Much of this harm is also avoidable

3
Primary Care Trigger Tool 29 September 2009 Harm and risk in primary care (Pringle) Low Risk: –No general anaesthetics or significant surgery –Little obstetrics etc High Risk: –First presentation of serious illness including emergencies –Prescribing –Chronic disease management etc
 Low Risk: –No general anaesthetics or significant surgery –Little obstetrics etc High Risk: –First presentation of serious illness including emergencies –Prescribing –Chronic disease management etc")
4
Primary Care Trigger Tool 29 September 2009 Pringle (cont) Positive Culture: –Teams often open to improvement –Annual appraisal and Clinical Governance Negative Culture: –Both practices and PCTs variable; and –Contract makes performance management challenging –“Someone else’s problem”
 Positive Culture: –Teams often open to improvement –Annual appraisal and Clinical Governance Negative Culture: –Both practices and PCTs variable; and –Contract makes performance management challenging – Someone else’s problem")
5
Primary Care Trigger Tool 29 September 2009 Inverse reporting law?

6
Primary Care Trigger Tool 29 September 2009 We need a measure Global Trigger Tool Develop for primary care Must have face validity

7
Issues to consider around a primary care GTT: Concept of a trigger tool. What’s it for? What needs to be considered when developing it? How to make it practical? Primary Care Trigger Tool 29 September 2009

8
Concept of primary care GTT Primary Care Trigger Tool 29 September 2009

9
Wales Primary Care Global Trigger Tool Why Primary Care GTT? Major differences between secondary and primary care Multiple consultations with relatively few interventions per patient contact Lower frequency of harm Ongoing duty of care to patients Need to include harm caused by omission as well as commission

10
Wales Primary Care Global Trigger Tool Trigger tool requirements Face validity Content validity Consistency Versatility Practicality Pick up rate

11
Wales Primary Care Global Trigger Tool Trigger tool approach used Need a sampling mechanism to identify cohorts of patients with high pick up rate Different approach for both acute and chronic care Need to maximise use of IT

12
Acute Care Component Number Patients seen in previous month on more than one occasion in ten days. Trigger : No. of patients seen in past month as an unscheduled review or No. of patients who have used an out of hours provider within ten days of a consultation. No showing evidence of harm Grade of harmEFGHI Number Primary Care Trigger Tool 29 September 2009

13
Definition of harm Taken from UK Global Trigger Tool and the National Coordinating Council for medication Error Reporting and prevention E: Temporary harm to the patient F: Temporary harm to the patient requiring intervention G: Permanent harm to the patient H: Harm requiring an intervention to sustain life I: Patient Death Primary Care Trigger Tool 29 September 2009

14
Chronic Care Component ( 20 patients with chronic condition, taking 3 or more medications and seen over past two months) Number of triggers Number showing harm Hospital admission in previous 2 months Discontinuation of medication in past 2 months Abnormal Haematology or Biochemistry result in past 2 months Documented Adverse drug reaction in past 2 months OOH consultation or A&E attendance past 2 months Grade of harmEFGHI
 Number of triggers Number showing harm Hospital admission in previous 2 months Discontinuation of medication in past 2 months Abnormal Haematology or Biochemistry result in past 2 months Documented Adverse drug reaction in past 2 months OOH consultation or A&E attendance past 2 months Grade of harmEFGHI")
15
Definition of abnormal lab. results A fall of > 2 g/dl in Hb A rise of 25% above baseline of serum creatinine The development of abnormal LFT Significantly abnormal [Na] 150 mmol/L Significantly abnormal [K] 6mmol/L An INR >5 Primary Care Trigger Tool 29 September 2009

16
SummaryNumber Total number of acute and chronic care triggers Total number of patients showing evidence of harm Harm rate ( No of patients harmed/ List size )
")
17
Primary Care Trigger Tool 29 September 2009 Practice Minfor Dat e July 09 List Size 5000 Acute Care Component Number Patients seen in previous month on more than one occasion in ten days. 75 Trigger : No. of patients seen in past month as an unscheduled review or No. of patients who have used an out of hours provider within ten days of a consultation. 12 No showing evidence of harm3 Grade of harmEFGHI Number3 Chronic Care Component Number of triggers Number showing harm Hospital admission in previous 2 months30 Discontinuation of medication in past 2 months41 Abnormal Haematology or Biochemistry result in past 2 months 40 Documented Adverse drug reaction in past 2 months22 OOH consultation or A&E attendance past 2 months41 Grade of harmEFGHI Number4 SummaryNumber Total number of acute and chronic care triggers29 Total number of patients showing evidence of harm7 Harm rate ( No of patients harmed/ List size )0.0014
")
18
Primary Care GTT – experience in other countries. Scotland. Results published summer 2009 New York Ambulatory Care model published summer 2009 English Model. Extensively trialled and recruiting practices Primary Care Trigger Tool 29 September 2009

19
US Experience. 1200 patients notes reviewed over a 12 month period Primary Care Trigger Tool 29 September 2009 Trigger typeAll sites TriggersADEs (PPV) 1. Medication stop590155 (26.3%) 2. Hospitalisation10122 (21.8%) 3. Emergency-room visit9414 (14.9%) 4. INR>588 (100%) 5. TSH<0.03 on thyroxine109 (90%) 6. Creat>2.5152 (13.3%) 7. BUN>60151 (6.7%) 8. ALT>84135 (38.5%) 9. AST>80153 (20%) Total of all triggers908232 (25.5%) Sensitivity of the top 9 triggers (% of ADEs detected by these) 94.8%94.4%
 1. Medication stop (26.3%) 2. Hospitalisation10122 (21.8%) 3. Emergency-room visit9414 (14.9%) 4. INR>588 (100%) 5. TSH<0.03 on thyroxine109 (90%) 6. Creat> (13.3%) 7. BUN>60151 (6.7%) 8. ALT>84135 (38.5%) 9. AST>80153 (20%) Total of all triggers (25.5%) Sensitivity of the top 9 triggers (% of ADEs detected by these) 94.8%94.4%.")
20
Scottish Experience. 500 records over 12 month period Primary Care Trigger Tool 29 September 2009 Table 1 Outline of the preliminary primary-care global trigger tool and trigger rationale TriggerDescription and rationale for use 1. Timing of consultation >3 contacts with the practice in any given period of a week (this can include telephone calls, consultations with nurse/GP or home visits) 2. Place of consultation Any home visit, whether by the GP or by a nurse from the practice serves as a trigger 3. Frequency of consultation>10 consultations for the period of review (12 months) 4. Changes to medication Has any "repeat medication" been added or cancelled in the period under review? 5. Adverse drug events/allergies Has a new "read code" for allergy/adverse drug event been added to the record in the year under review? 6. New clinical read code Has a high priority clinical "read code" been added to the record in the period under review? 7. Abnormal blood resultsSpecific abnormalities in U&E, LFT, INR and FBC levels served as a trigger 8. Out-of-hours and/or A&E Attendance at either of these services in the period under review served as a trigger 9. Hospital admission/discharge Has the patient been admitted to a hospital for any intervention, management or procedure? The patient should have been admitted for at least one night 10. >1 outpatient appointments in last yearMore than one outpatient appointment or hospitalised as a day-case during the period under review
 2. Place of consultation Any home visit, whether by the GP or by a nurse from the practice serves as a trigger 3. Frequency of consultation>10 consultations for the period of review (12 months) 4. Changes to medication Has any repeat medication been added or cancelled in the period under review. 5. Adverse drug events/allergies Has a new read code for allergy/adverse drug event been added to the record in the year under review. 6. New clinical read code Has a high priority clinical read code been added to the record in the period under review. 7. Abnormal blood resultsSpecific abnormalities in U&E, LFT, INR and FBC levels served as a trigger 8. Out-of-hours and/or A&E Attendance at either of these services in the period under review served as a trigger 9. Hospital admission/discharge Has the patient been admitted to a hospital for any intervention, management or procedure. The patient should have been admitted for at least one night 10. >1 outpatient appointments in last yearMore than one outpatient appointment or hospitalised as a day-case during the period under review.")
21
Scottish Experience. 500 records over 12 month period. 2251 consultations. Primary Care Trigger Tool 29 September 2009 Table 4 Positive triggers, harm and severity category TriggerPresent (n)Harm Severity Code (n) Preventable harm (n) ABCDEFGTotal 1. Timing111–––192–123 2. Place18––––2––20 3. Frequency72––––2––21 4. Medication change 53–112101–156 5. Allergies17–1––5––62 6. Read codes 9621––1––42 7. Abnormal laboratory results 55––114––64 8. Out-of- hours/emerge ncy care 99––1–3––41 9. Hospital care 65–22–13197 10. Outpatient consultation 141–––12–141 Total730255539626427
Harm Severity Code (n) Preventable harm (n) ABCDEFGTotal 1. Timing111–––192– Place18––––2––20 3. Frequency72––––2––21 4. Medication change 53–112101– Allergies17–1––5––62 6. Read codes 9621––1––42 7. Abnormal laboratory results 55––114––64 8. Out-of- hours/emerge ncy care 99––1–3––41 9. Hospital care 65–22– Outpatient consultation 141–––12–141 Total")
22
English Experience Extensively trialled Results not yet publically available Concentrate harm by looking at aged > 75 Primary Care Trigger Tool 29 September 2009

23
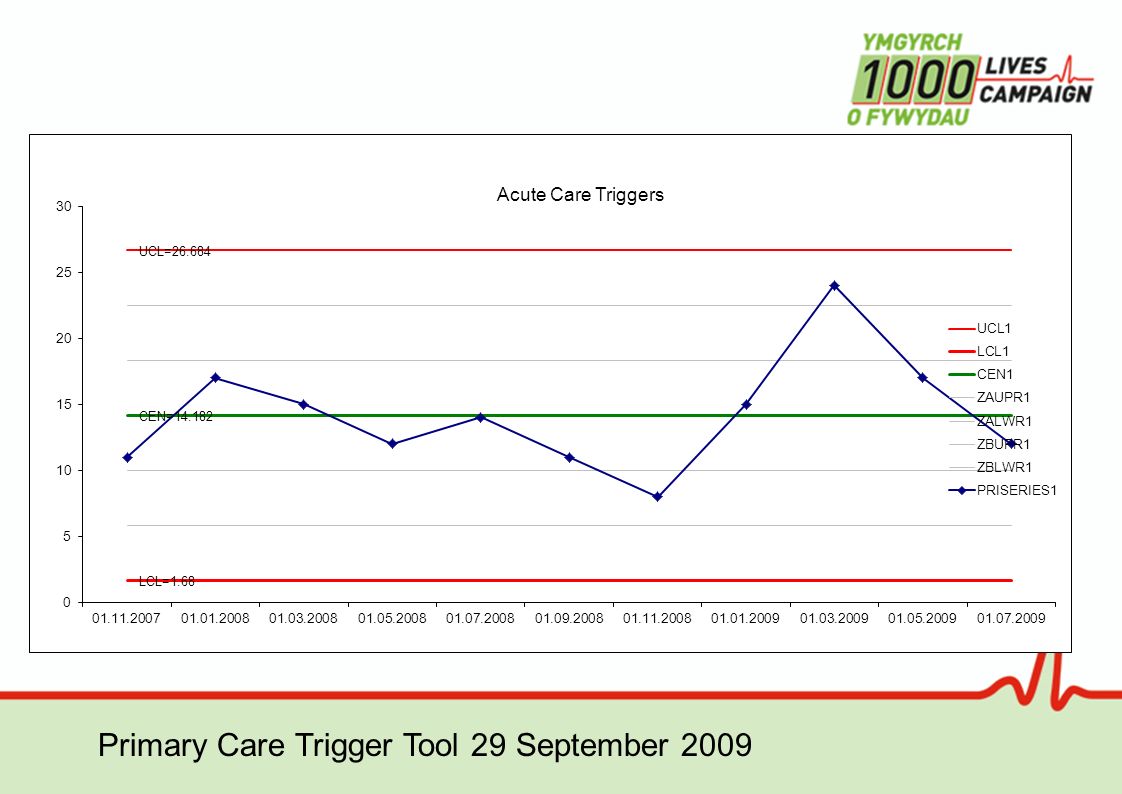
Trigger tool version one Results Acute Care NumberHarm% triggers associated with harm Pt seen more than once in 10 days over past month 570 No of these seen as an unscheduled review 902123 Primary Care Trigger Tool 29 September 2009

24
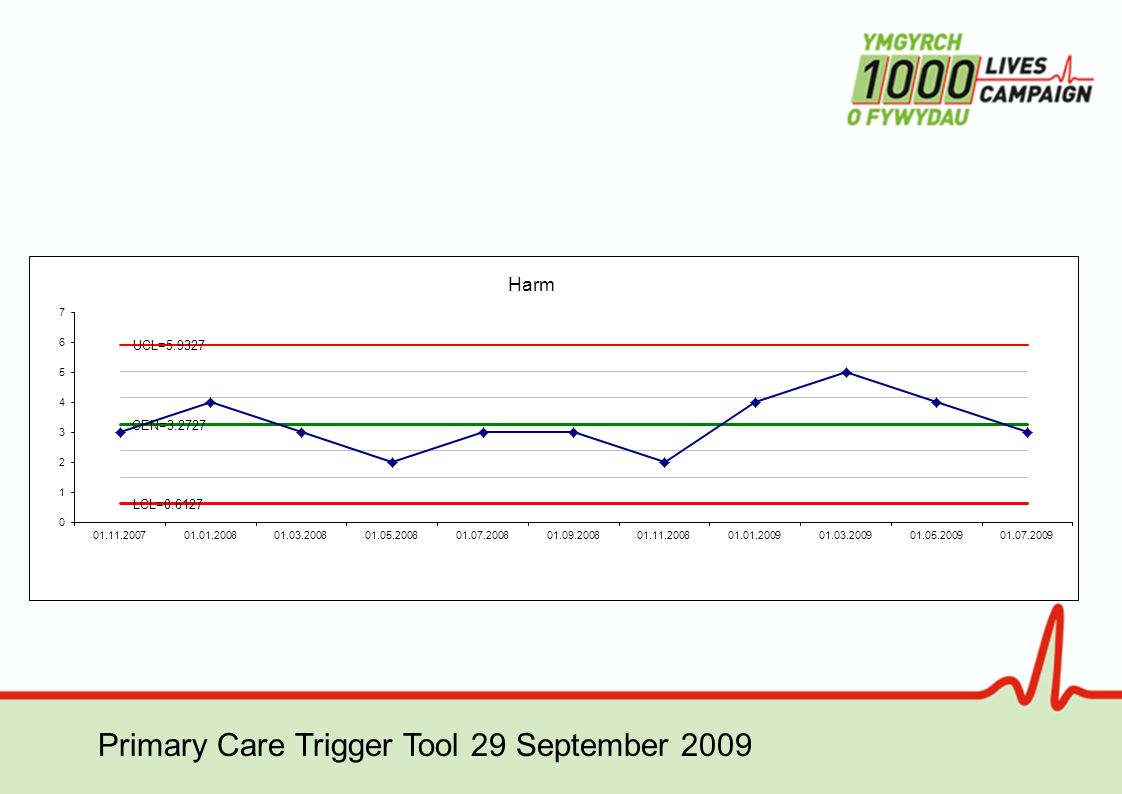
Trigger tool version one results Chronic Care No. Of TriggersNo. With harm% triggers associated with harm Hospital admission in previous 3 months 12325 Discontinuation of medication in 3 months 13646 Abnormal haematology or biochemistry 1716 Adverse drug reaction9888 OOH consultation or A and E 1417 Total chronic care triggers 651929 Primary Care Trigger Tool 29 September 2009

27
Conclusions The Welsh, Scottish and US tools use similar triggers The triggers which are most predictive of harm are similar in the Welsh, Scottish and US tools The Welsh tool is just about sufficiently practical to use on a regular basis to follow the progress of triggers and the risk of harm, unlike the other models. The English tool concentrates on the elderly, unlike the Welsh tool which looks at all age ranges, particularly in the acute component. We need to recruit more practices to use the tool regularly and collate the results. Primary Care Trigger Tool 29 September 2009

28
Next steps! Recruit a minimum of one practice per former LHB area By October 14 inform local Regional Coordinator of –Practice list size –Clinical system –Practice Lead for project By 30 October practice briefed and prepared for first run Results reported by end December Drs William Whitehead and Adam Southan will be available for phone advice throughout trial through the Regional Coordinators

29
Regional Coordinator Contact details North Wales Regional Coordinator – Andrea Hobbs Andrea.hobbs@gwyneddlhb.wales.nhs.uk Andrea.hobbs@gwyneddlhb.wales.nhs.uk Mid & West Regional Coordinator – Carol Tofts Carol.tofts@ceredigionlhb.wales.nhs.uk Carol.tofts@ceredigionlhb.wales.nhs.uk South Wales Regional Coordinator – Julie Hopkins Julie.hopkins@newportlhb.wales.nhs.uk Julie.hopkins@newportlhb.wales.nhs.uk

Similar presentations




 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")
>")
 Dr Ian Williams Greater Metro South Brisbane Medicare.>")








>")



