Download presentation
Presentation is loading. Please wait.

1
Kawasaki Disease Vaishali Soneji Lafita, MD

2
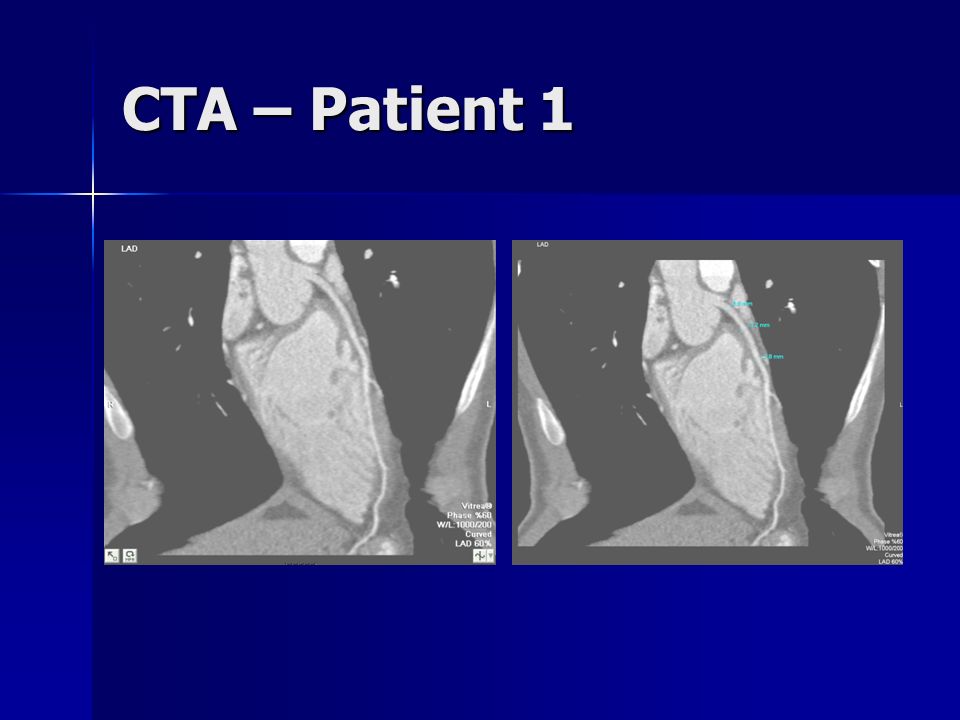
Presentation – Patient 1 10 years old male with Kawasaki Disease 10 years old male with Kawasaki Disease Possible mildly ectatic posterior descending coronary artery on Echo. Possible mildly ectatic posterior descending coronary artery on Echo. CTA was performed. CTA was performed. Heart rate control Contrast enhanced axial images of the coronary arteries Multiplanar and 3D reformats

3
CTA – Patient 1

7
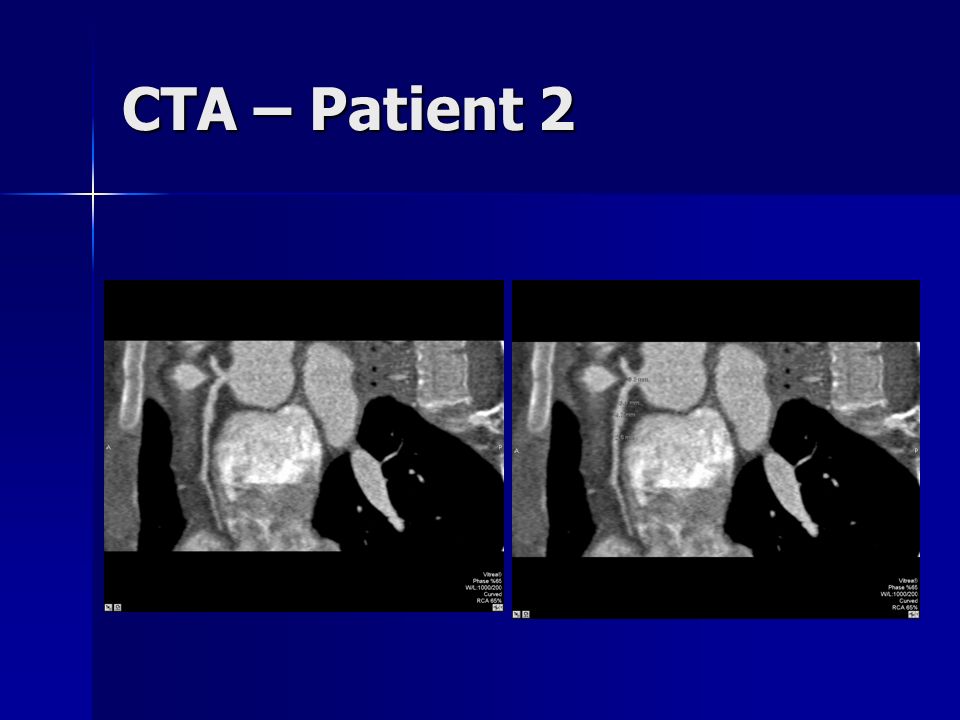
Presentation – Patient 2 13 years old male with Kawasaki Disease and known coronary aneurysm presents for CTA. 13 years old male with Kawasaki Disease and known coronary aneurysm presents for CTA. Heart rate control Contrast enhanced axial images of the coronary arteries Multiplanar and 3D reformats

8
CTA – Patient 2

11
Presentation – Patient 3 13 years old female with Kawasaki Disease and known coronary aneurysm diagnosed on Echocardiogram presents for CTA. 13 years old female with Kawasaki Disease and known coronary aneurysm diagnosed on Echocardiogram presents for CTA.

12
CTA – Patient 3

13
Kawasaki Syndrome AKA – Mucocutaneous Lymph Node Syndrome AKA – Mucocutaneous Lymph Node Syndrome First characterized in 1967 by Dr. Tomisaku Kawasaki of Tokyo First characterized in 1967 by Dr. Tomisaku Kawasaki of Tokyo Multisystem vasculitis Multisystem vasculitis Self limited Self limited Leading cause of acquired heart disease in the US. Leading cause of acquired heart disease in the US.

14
Epidemiology Syndrome of young children Syndrome of young children –>80% are 80% are < 4y/o –Most are between 1-2y/o –Very rare > 8y/o Males > females Males > females Japanese and Korean ancestry > other ethnicities Japanese and Korean ancestry > other ethnicities 4,000-8,000 cases/yr 4,000-8,000 cases/yr

15
Etiology Unknown Unknown Leading hypothesis Leading hypothesis –Infectious with immune-mediated reaction –No single etiologic agent identified

16
Clinical Manifestation and Diagnosis No recognized prodrome No recognized prodrome Acute onset Acute onset –Begins with fever –Other symptoms begin within 2-5 days Syndrome Syndrome –Fever for 5d + 4/5 symptoms –Fever for 5d + 3/5 symptoms + coronary artery abnormalities

17
Signs/symptoms 1. Nonpurulent bilateral conjunctivits 2. Oropharyngeal changes –Erythema, redness, cracking, peeling, injected pharynx, strawberry tongue 3. Polymorphous erythematous rash –Most evident with fever –Primarily on trunk, may be pruritic 4. Cervical lymphadenopathy –Often unilateral –One node >1.5cm 5. Feet/Hand changes –Erythema (palms/soles), edema, induration, desquamation
, edema, induration, desquamation.")
18
Signs/Symptoms Cardiac findings Cardiac findings –Leading cause of morbidity and mortality –May involve pericardium, myocardium, endocardium, valves, coronary arteries

19
Signs/Symptoms 20-25% of untreated pts develop coronary artery abnormalities/aneurys ms 20-25% of untreated pts develop coronary artery abnormalities/aneurys ms –Within 4 weeks of onset –Dilation can be detected at 10d –Peak 18-25d Giant aneurysm >8mm Giant aneurysm >8mm –Greatest risk thrombosis, stenosis, MI

20
Complications Cardiac manifestations can be deadly Cardiac manifestations can be deadly –Most deaths occur between 2-12 weeks post illness onset Coronary aneurysm thrombosis – MI Coronary aneurysm thrombosis – MI Aneurysm rupture Aneurysm rupture Myocarditis - CHF Myocarditis - CHF

21
Predicting Coronary Artery abnormalities Harada score Harada score 1.White blood cell count > 12K 2.Platlet count < 350K 3.CRP >3+ 4.Hct < 35% 5.Albumin < 3.5 g/dL 6.Age < 12 months 7.Male sex Used to determine management Used to determine management

22
Treatment Decrease inflammation Decrease inflammation Prevent thrombosis Prevent thrombosis Overall goal Overall goal –Protect the myocardium and coronary arteries Modes of treatment Modes of treatment –IVIG –Steroids –TNF –alpha antagonists –Aspirin –abciximab

23
Cardiac findings : Imaging Echocardiography Echocardiography –Unclear sensitivity and specificity Coronary Angiography Coronary Angiography Intravascular Ultrasound (IVUS) Intravascular Ultrasound (IVUS) Transesophageal echocardiography Transesophageal echocardiography MRA MRA CTA CTA
 Intravascular Ultrasound (IVUS) Transesophageal echocardiography Transesophageal echocardiography MRA MRA CTA CTA")
24
Cardiac findings :Imaging Echocardiogram Echocardiogram 1 st at time of diagnosis 1 st at time of diagnosis Number, location and classification of aneurysms Number, location and classification of aneurysms –Small, medium or giant Repeat echo 2-3 and 6-8 weeks after onset of the disease Repeat echo 2-3 and 6-8 weeks after onset of the disease –If both normal – no further echos needed If abnormal If abnormal –Severity determines frequency and type of follow-up

25
Cardiac findings :Imaging

26
Management of Aneurysms Small to medium: long term Aspirin, no activity restriction, stress test in older children if suggests stenosis → coronary angiography Small to medium: long term Aspirin, no activity restriction, stress test in older children if suggests stenosis → coronary angiography Multiple, small to medium or giant: Aspirin with/without warfarin, >10y stress test with myocardial perfusion scan if coronary obstruction → bypass grafting, angioplasty Multiple, small to medium or giant: Aspirin with/without warfarin, >10y stress test with myocardial perfusion scan if coronary obstruction → bypass grafting, angioplasty

27
Summary Self limited systemic vasculitis Self limited systemic vasculitis Leading cause of acquired heart disease in the US. Leading cause of acquired heart disease in the US. Morbidity and mortality from cardiac involvement. Morbidity and mortality from cardiac involvement. Imaging plays critical role in diagnosis and management of cardiac involvement. Imaging plays critical role in diagnosis and management of cardiac involvement.

28
References J. W. Newburger, M. Takahashi, M. A. Gerber, M. H. Gewitz, L. Y. Tani, J. C. Burns, S. T. Shulman, A. F. Bolger, P. Ferrieri, R. S. Baltimore, W. R. Wilson, L. M. Baddour, M. E. Levison, T. J. Pallasch, D. A. Falace, and K. A. Taubert Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Statement for Health Professionals From the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association Pediatrics, December 1, 2004; 114(6): 1708 - 1733. http://www.emedicine.com/EMERG/topic811.htm http://www.emedicine.com/EMERG/topic811.htm http://www.emedicine.com/EMERG/topic811.htm http://www.cdc.gov/ncidod/diseases/kawasaki/index.htm http://www.cdc.gov/ncidod/diseases/kawasaki/index.htm http://www.cdc.gov/ncidod/diseases/kawasaki/index.htm http://www.americanheart.org/presenter.jhtml?identifier=111 63 http://www.americanheart.org/presenter.jhtml?identifier=111 63 http://www.americanheart.org/presenter.jhtml?identifier=111 63 http://www.americanheart.org/presenter.jhtml?identifier=111 63
: identifier= identifier= identifier= identifier=")
Similar presentations



















 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")

 also known as Kawasaki Syndrome. An unusual and serious illness of young children. It is an autoimmune.>")
