Download presentation
Presentation is loading. Please wait.

1
Diffusion-weighted MRI hyperintensity patterns differentiate CJD from other rapid dementias – Vitali et al. Neurology 76 May 17, 2011

2
CJD degenerative neurological disorder that is incurable and invariably fatal due to a type of infectious protein called a prion Prions are misfolded proteins which replicate by promotes refolding of native proteins into the diseased state

3
CJD Types sCJD: Spontaneous or somatic mutation Familial/genetic CJD (fCJD): Mutations in gene (PRNP) that codes for the prion protein (5–10% of all CJD cases) Iatrogenic CJD: Infection from prion contaminated material vCJD: BSE in cattle is transmitted to humans through infected beef
: Mutations in gene (PRNP) that codes for the prion protein (5–10% of all CJD cases) Iatrogenic CJD: Infection from prion contaminated material vCJD: BSE in cattle is transmitted to humans through infected beef")
4
Presents as a rapidly progressive dementia (RPD), but other (npRPD) disorders have similar presentation Many npRPD are treatable Important to diagnose CJD for infection control EEG & CSF biochem has limited utility in CJD dx
, but other (npRPD) disorders have similar presentation Many npRPD are treatable Important to diagnose CJD for infection control EEG & CSF biochem has limited utility in CJD dx")
5
Aim Evaluate the sensitivity and specificity of FLAIR and DWI MRI for sCJD compared to a cohort of npRPD subjects Identify MRI features that differentiate CJD from other npRPD

6
Method - Subjects Retrospective case-control study Total of 90 included subjects (61 CJD : 29 npRPD) –in whom CJD was considered as a DDx –who had sufficient quality FLAIR and DWI imaging performed at UCSF Memory & Aging Centre between Dec 2000 and Feb 2007
 –in whom CJD was considered as a DDx –who had sufficient quality FLAIR and DWI imaging performed at UCSF Memory & Aging Centre between Dec 2000 and Feb 2007")
7
61 CJD –48 sCJD (43/48 tested for PRNP mutation ie fCJD – all negative) 41 path proven 7 non-pathology proven cases, met WHO criteria –6 fCJD –7 GSS (Gerstmann–Sträussler– Scheinker syndrome) 29 npRPD –14/29 tested for PRNP: all negative –15/29 not pathologically proven, but included survival was outside the range of sCJD subjects (> 3 years) definitive (e.g., serological or genetic) evidence of another disorder and/or they improved with (or without) treatment.
 41 path proven 7 non-pathology proven cases, met WHO criteria –6 fCJD –7 GSS (Gerstmann–Sträussler– Scheinker syndrome) 29 npRPD –14/29 tested for PRNP: all negative –15/29 not pathologically proven, but included survival was outside the range of sCJD subjects (> 3 years) definitive (e.g., serological or genetic) evidence of another disorder and/or they improved with (or without) treatment.")
8
npRPD diagnostic groupsSpecific diagnosis Total (N=29) Path- proven Serologi cally or genetic proven (N=5) Neurodegenerative dementiasTotal125 Corticobasal degeneration31 Frontotemporal dementia32 Alzheimer’s disease22 Dementia with Lewy Bodies2 Parkinson’s disease1 Unknown dementia1 Autoimmune or paraneoplastic encephalopathyTotal954 Antibody-mediated neuro-autoimmune disorder434 Hashimoto’s encephalopathy2 Sarcoidosis11 metastatic non-CNS Hodgkin’s lymphoma11 Multiple sclerosis1 Vascular dementiasStrokes2 TumorsCNS lymphoma22 InfectiousMeningoencephalitis22 Toxic- MetabolicTotal21 Alcoholic encephalopathy1 MELAS11
 Path- proven Serologi cally or genetic proven (N=5) Neurodegenerative dementiasTotal125 Corticobasal degeneration31 Frontotemporal dementia32 Alzheimer’s disease22 Dementia with Lewy Bodies2 Parkinson’s disease1 Unknown dementia1 Autoimmune or paraneoplastic encephalopathyTotal954 Antibody-mediated neuro-autoimmune disorder434 Hashimoto’s encephalopathy2 Sarcoidosis11 metastatic non-CNS Hodgkin’s lymphoma11 Multiple sclerosis1 Vascular dementiasStrokes2 TumorsCNS lymphoma22 InfectiousMeningoencephalitis22 Toxic- MetabolicTotal21 Alcoholic encephalopathy1 MELAS11")
9
Exclusion criteria Some RPD subjects were initially excluded due to insufficient diagnostic confidence levels or diagnoses were not clear insufficient quality MRI*

10
Methods – MRI Acquisition 2 GE Signa 1.5T scanners FLAIR and DWI/DTI in axial planes; most had coronal planes Slice thickness varied from 3-5mm

11
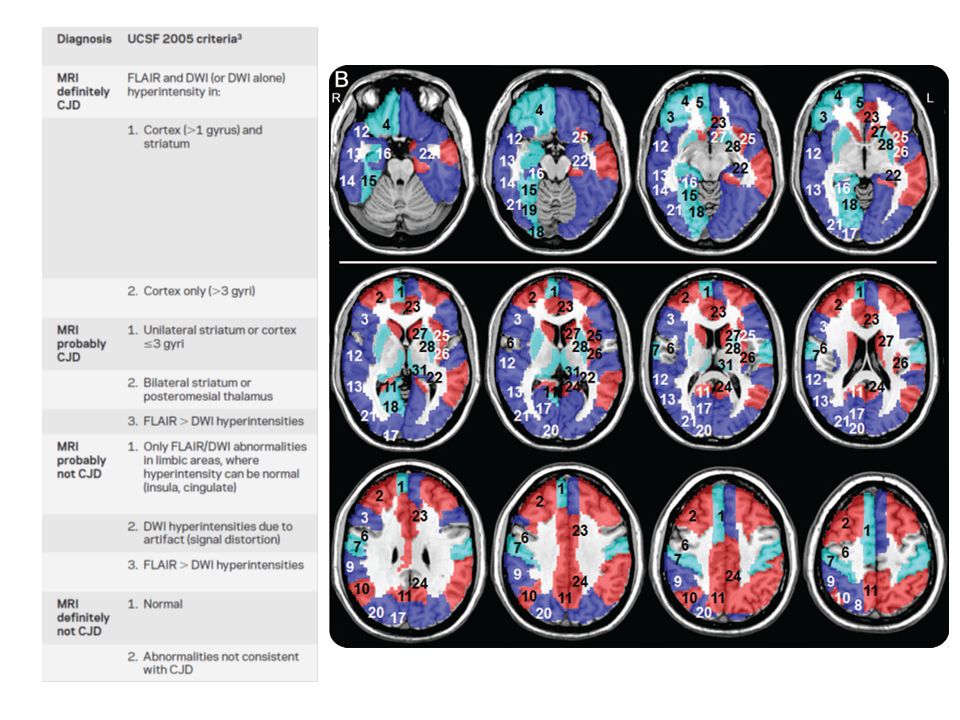
Methods – Visual assessment Multiplanar independent review by two neuroradiologists blinded to clinical diagnosis –Reader 1: 4 years experience –Reader 2: 20 years experience Gray matter involvement on FLAIR and DWI reported according to 26 cortical and 5 cortical divisions per hemisphere Based on imaging findings, readers classified subjects as definitely, probably, probably not, or definitely not CJD according to prior MRI criteria Consensus review: if readers disagreed on diagnosis (?classification), MRI examined together to make a consensus diagnosis
, MRI examined together to make a consensus diagnosis")
13
Methods – Determining patterns of gray matter involement in sCJD Each of 31 hemispheric regions on DWI MRI was scored 0, 1, or 2, according to how many readers judged a region as hyperintense The percentage of subjects with sCJD with involvement of each brain region was determined by averaging the ratings of both readers Subjects with sCJD were categorized into 6 different patterns of gray matter involvement

14
Methods – Unblinded review and identifying differentiating features After consensus review, the readers re- examined the MRIs “unblinded” to identify crucial differentiating features. Modified sCJD MRI criteria based on the results of the analysis

15
Results - Sensitivity and specificity for diagnosing sCJD SensitivitySpecificity Reader 192%72% Reader 294%100% Consensus reached in all but 3 cases (1 sCJD, 2 npRPD) 96%93%
 96%93%")
16
Pattern of FLAIR and DWI neocortical, limbic and subcortical hyperintensities in sCJD vs npRPD 60/61 sCJD had hyperintensities in neocortical, subcortical or limbic regions or in combination None had isolated limbic involvement Abnormalities more evident on DWI > FLAIR

17
Pattern of FLAIR and DWI neocortical, limbic and subcortical hyperintensities in sCJD vs npRPD 9/29 npRPD had abnormal gray matter hyperintensities All had limbic involvement (7 isolated; 2 cases with also subcortical involvement) Abnormalities more evident FLAIR > DWI
 Abnormalities more evident FLAIR > DWI")
18
MRI features in genetic prion disease 5/6 fCJD had gray matter hyperintensities Overlapping pattern of MRI abnormality with sCJD 1/7 GSS read as positive 2/7 GSS had isolated limbic involvement 4/7 GSS no abnormality

19
MRI unblinding False positives due to misinterpreting artifactual hyperintense signals on DWI as restricted diffusion (?without looking at ADC) False negatives due to failure to notice diffuse hyperintense cortical signals in subjects without subcortical abnormalities
 False negatives due to failure to notice diffuse hyperintense cortical signals in subjects without subcortical abnormalities")
20
Cases without MRI diagnosis at consensus review 1 sCJD 1 sarcoid 1 dementia with Lewy Bodies

21
Improving MRI criteria for sCJD MRI criteria for sCJD modified given the findings above Unblinded consensus review –98% sensitivity –100% specificity

22
Discussion In sCJD hyperintensity on DWI > FLAIR In npRPD hyperintensity on FLAIR > DWI Subcortical DWI hyperintensity in sCJD always associated with ADC hypointensity ie. Diffusion restriction (which is thought to be due to vacuolation) *Diffusion restriction may decline in late stages of sCJD → therefore early MRI may yield better sensitivity than later MRI
 *Diffusion restriction may decline in late stages of sCJD → therefore early MRI may yield better sensitivity than later MRI.")
23
Discussion Other npRPD conditions not included in the study cohort (eg. Extrapontine myelinolysis, Wilson’s disease, Wernicke encephalopathy and Bartonella infection) may have MRI features that mimic sCJD
 may have MRI features that mimic sCJD.")
24
Discussion Isolated limbic involvement only seen in npRPD (and GSS) If isolated limbic involvement is seen FLAIR > DWI → “probably not CJD” If isolated limbic involvement is seen DWI > FLAIR, particularly with diffusion restriction → consider encephalitis and seizures
 If isolated limbic involvement is seen FLAIR > DWI → probably not CJD If isolated limbic involvement is seen DWI > FLAIR, particularly with diffusion restriction → consider encephalitis and seizures")
25
fCJD MRI pattern closely resembles sCJD This MRI pattern not found in GSS

26
Reader variability

27
Conclusion Patterns of FLAIR and DWI abnormalities can differentiate sCJD from npRPD Only some fCJD/GSS cases have overlapping features with sCJD MRI with DWI and ADC would be included in sCJD diagnostic criteria

28
Limitations ADC maps only examined only in cases with DWI hyperintensity Retrospective review after the study showed ADC hypointensities without DWI hyperintensity in some cases This may be due to “T2 blackout” effect caused by age related iron deposition in the GP and precental gyrus which cases hypointense signal and masks the hyperintense signal from prion disease

Similar presentations
>")



 rare progressive neurodegenerative disorders that affect both humans and animals. They.>")






 Jeanette Meadway FRCP Consultant Physician Mildmay Hospital UK Hackney Road, London E2 7NA.>")


 involves an immune-mediated process in which an abnormal response of the body’s immune system.>")




