Download presentation
Presentation is loading. Please wait.

1
Bioterrorism Mass Casualty Response: Current Concepts and Controversies
European Masters in Disaster Medicine Sandigliano, Italy 02 May 2005 Eric K. Noji, M.D., M.P.H., FACEP Medical Epidemiologist Centers for Disease Control & Prevention Washington, D.C.

3
The Immediate Future – A Revolution in biotechnology, genomics and proteomics that will affect all human beings

6
“A bioterrorism attack anywhere in the world is inevitable in the 21st century.” Anthony Fauci, Director, NIAID Clinical Infectious Diseases 2001;32:678

7
Smallpox Infected People Disperse
Flights to thirty eight US cities with infected passengers

8
… Life Has Changed for us all
I find this image and the next two genuinely terrifying. I hesitated using them here -- in part because they might be regarded as EXPLOITING the suffering of those who died or were left behind with horrible loss. But it is important, I believe, NOT to forget that – for good reason – it is TERROR which lends its name to terrorism.

9
Conventional (Explosive) Biological / Radoilogic
CBRNE Agents Conventional (Explosive) Chemical Biological / Radoilogic Onset Instant Rapid Often Delayed Source Obvious Often covert First Victim Encounter Prehospital Hospital Containment Easy Relatively Easy Difficult Decon Helpful Usually Not Yes Usually Not*
 Chemical. Biological / Radoilogic. Onset. Instant. Rapid. Often Delayed. Source. Obvious. Often covert. First Victim Encounter. Prehospital. Hospital. Containment. Easy. Relatively Easy. Difficult. Decon Helpful. Usually Not. Yes. Usually Not*")
14
Infection: Invasion of a host by an agent, with subsequent establishment and multiplication of the agent. An infection may or may not lead to disease. Disease results only if and when, as a consequence of the invasion and growth of a pathogen, tissue function is impaired.

15
Thou shalt Protect Thyself

16
Protection Against BW Physical Personal protective gear Chemical
pre- & post-exposure antibiotics Immunologic passive (e.g. Botulinum antitoxin) active (e.g. Anthrax & Vaccinia vaccines)
 active (e.g. Anthrax & Vaccinia vaccines)")
20
Thou shalt Decontaminate as Appropriate

21
Decontamination after Biological Attack
Materiel often unnecessary less relevant than for Chem attack 5.0% bleach more than adequate 0.1% bleach kills anthrax spores Personnel decon rarely needed less relevant than for Chem attack soap & water use common sense

22
Diagnosis Clinical Epidemiological Laboratory

23
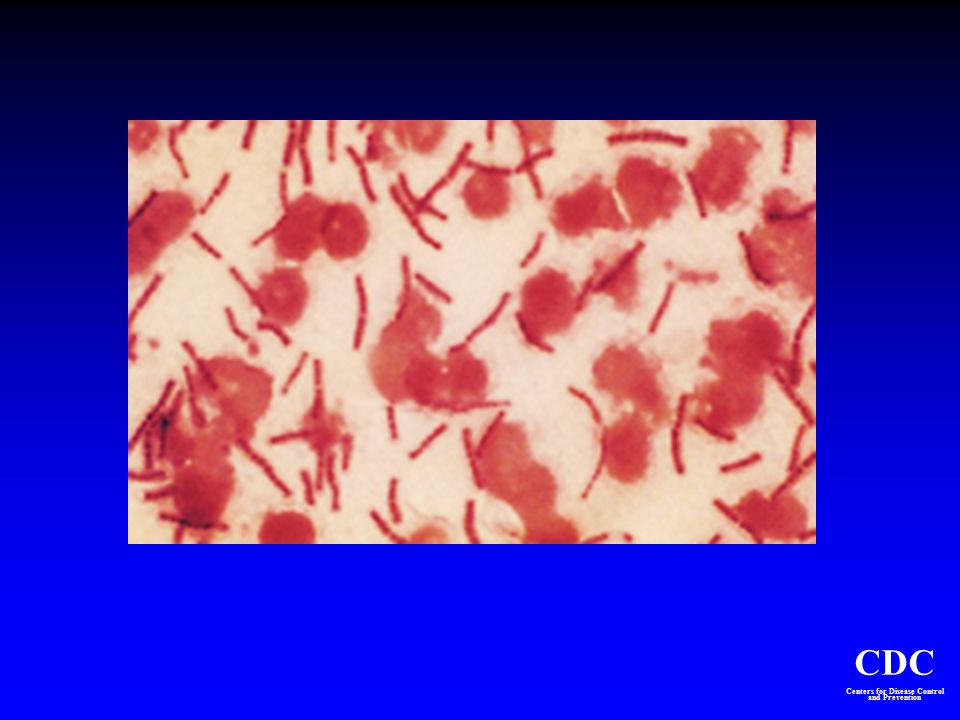
Anthrax (Bacillus anthracis)
Inhalational, gastrointestinal, cutaneous NOT communicable (except maybe cutaneous) Vaccine not available for civilian use 20%-80% mortality
 Vaccine not available for civilian use. 20%-80% mortality.")
24
Anthrax: Inhalational
Inhalation of spores Incubation: 1 to 43 days Initial symptoms (2-5 d) Fever, cough, myalgia, malaise Terminal symptoms (1-2d ) High fever, dyspnea, cyanosis Hemorrhagic mediastinitis/effusion Rapid progression shock/death Mortality rate ~ 100% w/o RX
 Fever, cough, myalgia, malaise. Terminal symptoms (1-2d ) High fever, dyspnea, cyanosis. Hemorrhagic mediastinitis/effusion. Rapid progression shock/death. Mortality rate ~ 100% w/o RX.")
25
Varying Presentations of NYC Cutaneous Lesions

26
Diagnosis -Diagnosis difficult given diseases have been seen by few living clinicians -Abnormal presentations of classical diseases may be present due to super infection -Diagnosis critical for epidemiological monitoring -Accurate data required for potential future prosecution of war crimes -Psychogenic overlay may cloud the diagnostic process

28
Small Pox (Variola major virus)
Transmitted primarily by aerosol route, contaminated clothes & linens Highly communicable Vaccine can lessen the severity of disease if given within 4 days of exposure

29
Increasing Global Travel
Rapid access to large populations Poor global security & awareness ...create the potential for simultaneous creation of large numbers of casualties

30
Epidemiological Pattern of Smallpox Weapon
New foci of secondary infection “Contaminated” zone “Infected” zone Zone of initial explosion

32
Pneumonic Plague Caused by infection with Yersinia Pestis
Pneumonic form will occur after intentional aerosol delivery Incubation period of 1-7 days

34
Obtaining Specimens CBC, ABG Nasal Swabs (culture, PCR)
Blood for Bacterial Culture, PCR Serology Sputum Bacterial Culture Toxin Assays (blood, urine) Throat Swab (viral culture, PCR, ELISA) Environmental Samples?
 Throat Swab (viral culture, PCR, ELISA) Environmental Samples")
35
Where to Send Specimens?
Local Clinical Lab Laboratory Channels 520th TAML USAMRIID USAMRICD

37
Thou shalt Render Prompt Treatment

38
Biological Warfare Diseases Non-Specific Febrile Presentations

39
Smallpox: Current Vaccine
Made from live Vaccinia virus ID inoculation with bifurcated needle (scarification) Pustular lesion/induration surrounding central scab/ulcer 6-8 days post-vaccination Low grade fever, axillary lymphadenopathy Scar (permanent) demonstrates successful vaccination Immunity not life-long Vaccine is live vaccinia virus (not smallpox virus) Intradermal inoculation Unique vaccination method compared to other current vaccination techniques (scarification with a bifurcated needle) Scar after vaccination was evidence of successful vaccination Immunity is not life-long Average immunity after vaccination 3-10 yrs. WHO
 Pustular lesion/induration surrounding central scab/ulcer 6-8 days post-vaccination. Low grade fever, axillary lymphadenopathy. Scar (permanent) demonstrates successful vaccination. Immunity not life-long. Vaccine is live vaccinia virus (not smallpox virus) Intradermal inoculation. Unique vaccination method compared to other current vaccination techniques (scarification with a bifurcated needle) Scar after vaccination was evidence of successful vaccination. Immunity is not life-long. Average immunity after vaccination 3-10 yrs. WHO.")
43
Thou shalt Practice Good Infection Control

44
Isolation Precautions Biowarfare Diseases
Pneumonic Plague Droplet Precautions Smallpox ? Airborne Precautions “Strict Quarantine” Viral Hemorrhagic Fevers Contact Precautions

45
What is the US Health Care System?
Roughly 6000 hospitals 615,000 physicians and surgeons 2.4 million registered nurses 240,000 pharmacists Approximately $390 billion spent on healthcare in 2003 $15.5 billion spent on hospital construction (2001)
")
46
Current Issues The US healthcare system functions at capacity on a daily basis Expansion (surge) capability relies on federal programs that take time to deploy Personnel engaged in healthcare are already functioning at maximum Contagious patients may render existing facilities inoperable No formal process to identify who is in charge (of what) when using multi-jurisdictional assets
 capability relies on federal programs that take time to deploy. Personnel engaged in healthcare are already functioning at maximum. Contagious patients may render existing facilities inoperable. No formal process to identify who is in charge (of what) when using multi-jurisdictional assets.")
47
WORSENING SITUATION IN US
Many hospitals on diversion during normal times (no inpatient beds, consultants) Decreasing number of emergency depts, trauma centers, inpatient beds Not economically viable for hospitals to maintain surge capacity,
 Decreasing number of emergency depts, trauma centers, inpatient beds. Not economically viable for hospitals to maintain surge capacity,")
55
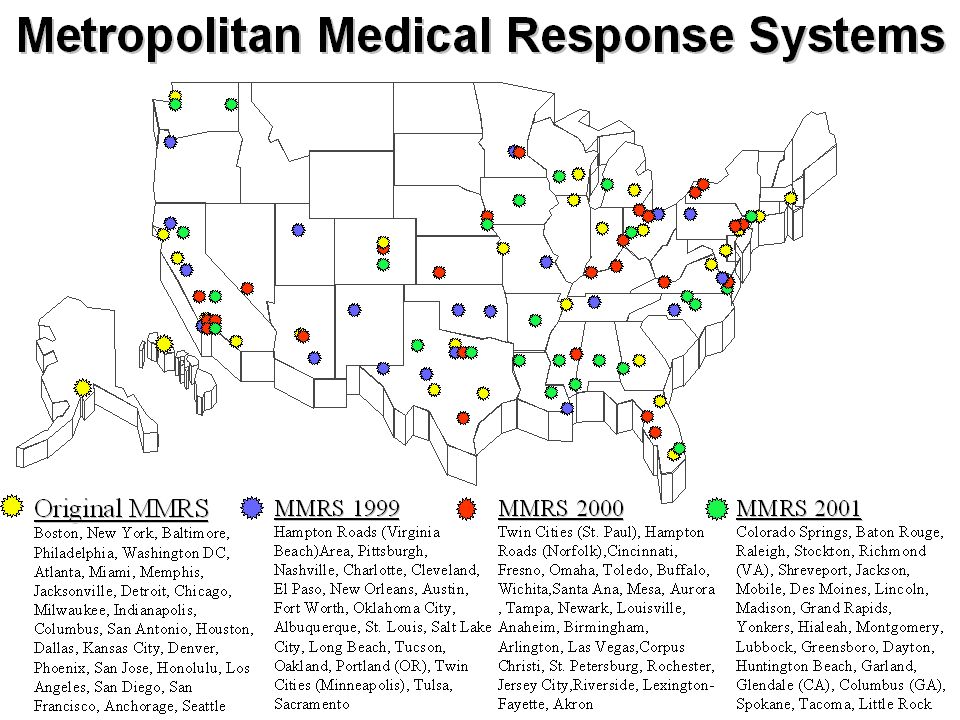
Metropolitan Medical Response System MMRS
Enhancing existing local first responder, medical, public health and emergency planning to increase capabilities to manage the incident until Federal resources arrive (typically hours)
")
57
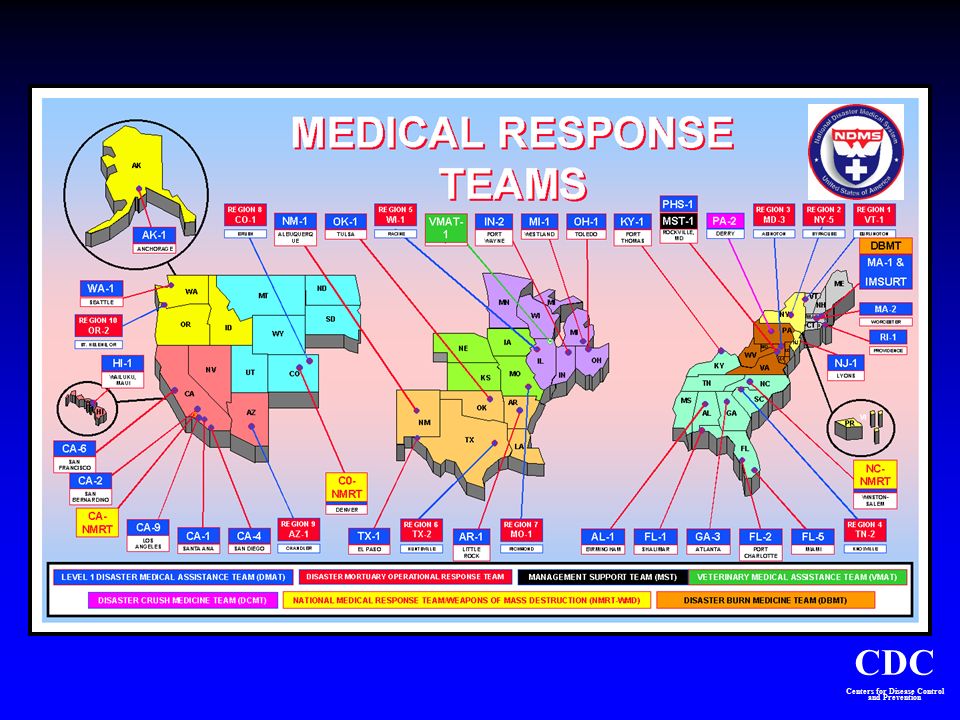
National Disaster Medical System
MAJOR COMPONENTS Medical Response Patient Evacuation Definitive Medical Care

59
Strategic National Stockpile
Twelve push packages ready for deployment within 12 hours anywhere in the U.S. Vendor Managed Inventory (VMI) – specific medical supplies needed to control and contain outbreaks of infectious diseases and other emergency incidents
 – specific medical supplies needed to control and contain outbreaks of infectious diseases and other emergency incidents.")
62
SNS Contents Pharmaceuticals: Antibiotics
Mark I kits, diazepam, atropine, pralidoxime IV Supplies: catheters, syringes, fluids, heparin-locks, administration sets Airway Supplies: ventilators, ambu-bags, ET tubes, laryngoscopes, suction devices, oxygen masks, NG tubes Other Emergency Medications: for hypotension, anaphylaxis, sedation, pain management Bandages and Dressings Vaccine

63
Bad communication adds to crisis
Mixed messages from multiple “experts” Late information “overcome by events” Over-reassuring messages No reality check on recommendations Myths, rumors, doomsayers not countered Poor performance by spokesperson/leader Public power struggles and confusion

65
A Typical Day at CDC Autumn 2001

66
Public Awareness Reliable, credible information to the public is key to keeping cooperation and minimizing panic

67
Tactical response to biological weapon exposure
Need to make life-saving decisions rapidly in the absence of data Access to subject matter experts will be limited No “textbook” experience to guide response Need coherent, rapid process for addressing staff and civilian safety in midst of crisis

68
Top STRATEGIC Challenges to Hospital Preparedness
Surge Capacity Healthcare Personnel Relevant training Sufficient numbers Materiel Pharmaceuticals Decontamination equipment Collaboration at local, state, and federal level Must prepare for MCI at the same time as providing “routine” healthcare to the community!

69
Bottom Line Early, rapid recognition of unusual clinical syndromes or deaths Early rapid recognition of increase above “expected levels” of common syndromes, diseases, or death

70
CDC and Biodefense Alexander Langmuir Founder of CDC EIS Program 1952
The detection and control of saboteurs are the responsibilities of the FBI, but the recognition of epidemics caused by sabotage is particularly an epidemiologic function…. Therefore, any plan of defense against biological warfare sabotage requires trained epidemiologists, alert to all possibilities and available for call at a moment’s notice anywhere in the country” Alexander Langmuir Founder of CDC EIS Program 1952

71
Questions ?

Similar presentations























 PROGRAM 2001 Centers for Disease Control and Prevention National Center for Environmental Health Division of.>")
,>")





 Director, Emergency, Disaster Management and.>")






 Updated 11:30 a.m. 2-9-15 1.>")

