Download presentation
Presentation is loading. Please wait.

1
Information, choices & professional judgement: what’s right, wrong and can be done with decision making in the health professions. Dr Carl Thompson, Department of Health Sciences, University of York, UK Alberta Heritage Foundation for Medical Research Visiting Scholar

2
What are we talking about? Not tasks and not activity per se Not tasks and not activity per se The weighting of information (professional judgement) The weighting of information (professional judgement) Using these weighed pro’s and con’s to make choices (clinical decisions) Using these weighed pro’s and con’s to make choices (clinical decisions)
 The weighting of information (professional judgement) Using these weighed pro’s and con’s to make choices (clinical decisions) Using these weighed pro’s and con’s to make choices (clinical decisions).")
3
Why worry about decision making and judgement? They contribute to They contribute to health gain health gain Mortality and morbidity Mortality and morbidity Professional power Professional power Patient involvement Patient involvement Decisions and Judgements are the ‘black box’ in healthcare. Decisions and Judgements are the ‘black box’ in healthcare. Boundaries and the ball park are shifting Boundaries and the ball park are shifting

4
Cognitive inputs Organisational factors Social factors Patient values As well as: Resources Research knowledge Uncertainty Policy Time Control over decision elements

5
The good news Given conditions of irreducible uncertainty most decisions are good enough Given conditions of irreducible uncertainty most decisions are good enough People apply the same rules to professional decision making as they do in real life – this is a good thing! People apply the same rules to professional decision making as they do in real life – this is a good thing!

6
The Bad News Within unavoidable events in healthcare are avoidable events Within unavoidable events in healthcare are avoidable events Cognitive shortcuts lead to systematic errors… Cognitive shortcuts lead to systematic errors… Simply relying on clinical experience is not enough Simply relying on clinical experience is not enough

7
Does bad judgement matter? USA 44-98,000 deaths – “To Err is Human” USA 44-98,000 deaths – “To Err is Human” Australia 250,000 adverse events Australia 250,000 adverse events 50,000 permanent disability 50,000 permanent disability 10,000 deaths “Iatrogenic Injury in Australia” 10,000 deaths “Iatrogenic Injury in Australia” Denmarkconfirmed 9% of admissions Denmarkconfirmed 9% of admissions N.Z. confirmed 10% of admissions N.Z. confirmed 10% of admissions UK11% of admissions UK11% of admissions 850,000 adverse events 850,000 adverse events deaths & permanent disability deaths & permanent disability Between 7 and 8.4 additional bed days per adverse event Between 7 and 8.4 additional bed days per adverse event

8
Why do they happen… Was there a prior intention to act? Was there intention in action? Involuntary or no intentional action Spontaneous or subsidiary action Did the actions proceed as planned? Unintentional action (slip or lapse) Did the actions achieve their desired end? Intentional but mistaken action Successful action No Yes
 Did the actions achieve their desired end. Intentional but mistaken action Successful action No Yes.")
9
What can be done More sophisticated maps of the ‘black box’ More sophisticated maps of the ‘black box’ Develop what we know works Develop what we know works Decision supportive technologies Decision supportive technologies Education and training in handling uncertainty Education and training in handling uncertainty

10
ANALYSIS INTUITION Quality Of intuition Quality Of Analysis Least Precise/ explicit Definition of concepts Specification of relationships Measurement of magnitudes most Precise/ explicit MODE “7” 6 5 4 3 2 1 KNOWLEDGE non- clinical expert descriptive case randomised scientific GENERATION cognitive judgement consensus (positive) control controlled experiment “judgement” judgement model study trial DECISION non-cognitive clinical expert decision MAKING “decision” judgement consensus (normative) decision model © dowie2002
 control controlled experiment judgement judgement model study trial DECISION non-cognitive clinical expert decision MAKING decision judgement consensus (normative) decision model © dowie2002")
11
Social judgement modelling

12
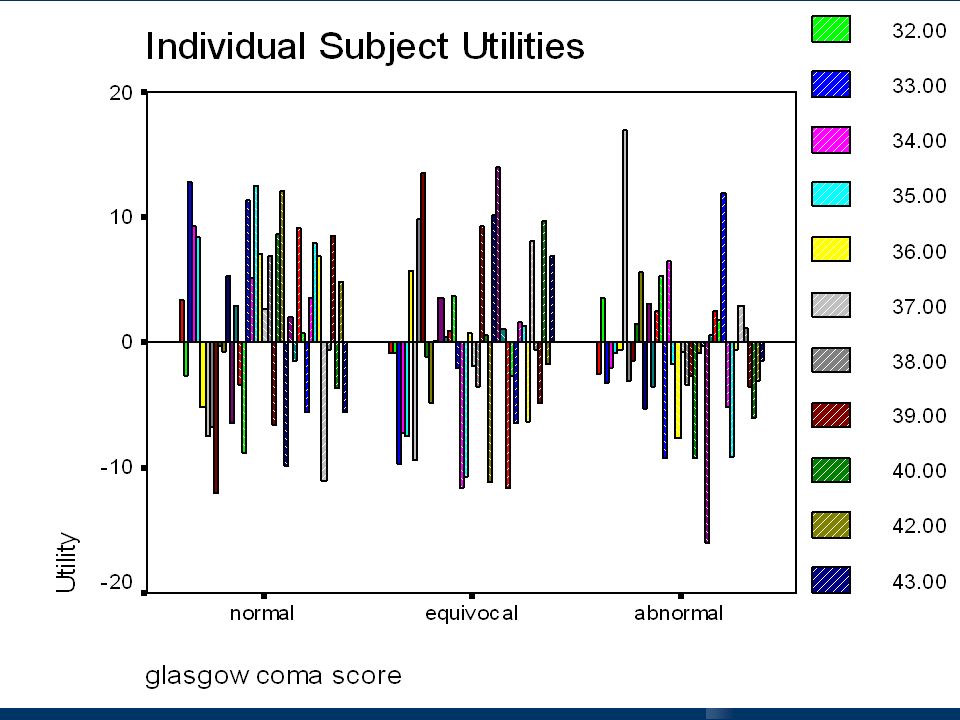
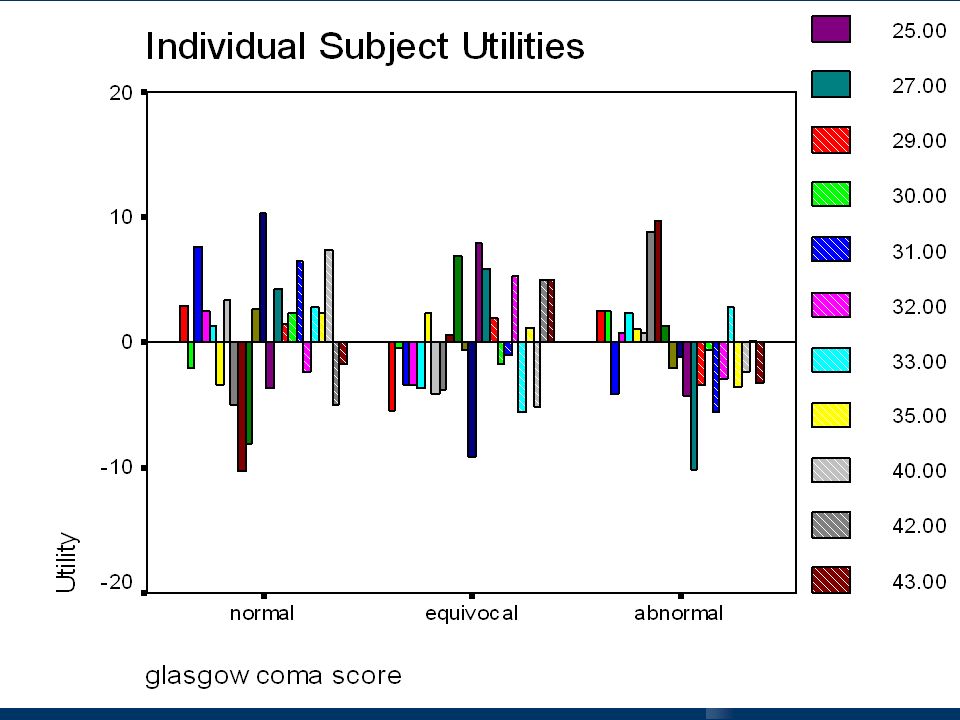
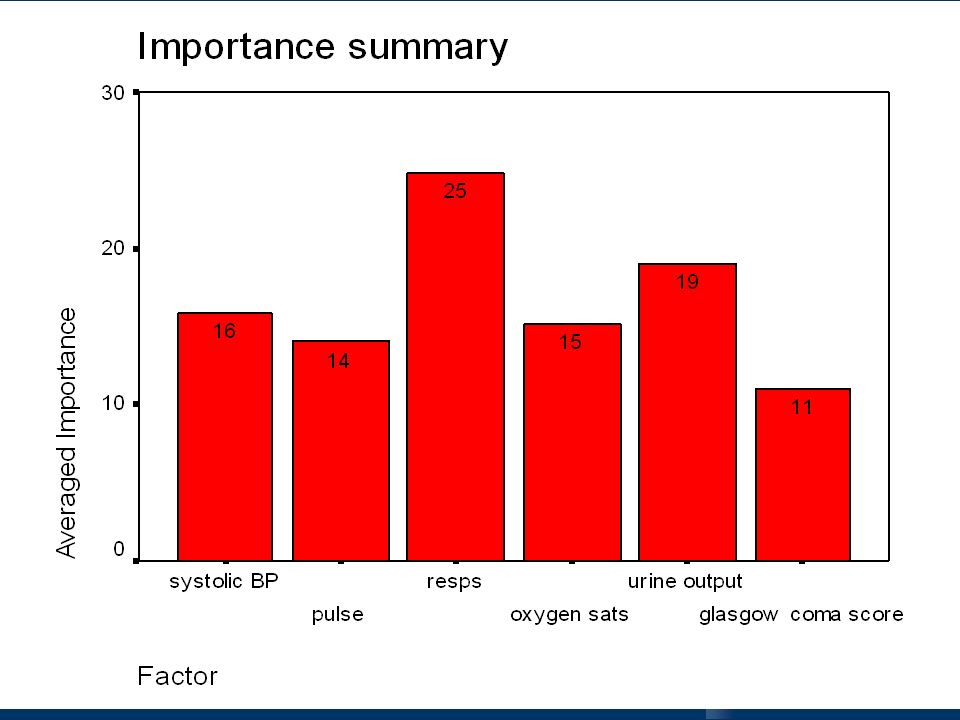
Example: shock www.york.ac.uk/res/dec/shock www.york.ac.uk/res/dec/shock www.york.ac.uk/res/dec/shock 20 cue profiles in orthogonal design 20 cue profiles in orthogonal design BP, Pulse, Resps, Urine Output, GCS. BP, Pulse, Resps, Urine Output, GCS. 3 levels (abnormal, normal, equivocal) 3 levels (abnormal, normal, equivocal) Left side from regression of 100 cases in ITU Left side from regression of 100 cases in ITU 45 students pre-post intervention (lecture and web-based teaching materials – targeted) 45 students pre-post intervention (lecture and web-based teaching materials – targeted)
 3 levels (abnormal, normal, equivocal) Left side from regression of 100 cases in ITU Left side from regression of 100 cases in ITU 45 students pre-post intervention (lecture and web-based teaching materials – targeted) 45 students pre-post intervention (lecture and web-based teaching materials – targeted).")
16
Using (refining and evaluating) effective interventions Multifaceted interventions (combine 2 or more of audit and feedback, reminders, local consensus processes, marketing) Multifaceted interventions (combine 2 or more of audit and feedback, reminders, local consensus processes, marketing) Interactive educational meetings Interactive educational meetings Reminders Reminders Educational outreach visits Educational outreach visits
 effective interventions Multifaceted interventions (combine 2 or more of audit and feedback, reminders, local consensus processes, marketing) Multifaceted interventions (combine 2 or more of audit and feedback, reminders, local consensus processes, marketing) Interactive educational meetings Interactive educational meetings Reminders Reminders Educational outreach visits Educational outreach visits")
17
Decision support Function Example AlertingHighlighting out of range (either too high or too low laboratory values) RemindingReminding the clinician to schedule a cervical smear CritiquingRejecting an inappropriate order for a new drug InterpretingAnalysing an electrocardiogram PredictingCalculating the risk of mortality from a severity of illness score DiagnosingListing a differential diagnosis for a patient with chest pain AssistingTailoring the antibiotic choices for patients with STDs SuggestingGenerating suggestions for adjusting a mechanical ventilator in an Intensive Therapy Unit. FacilitatingProviding a forum for interaction, model building and joint negotiation of treatment.

18
Better education Right knowledge for professional activity? Right knowledge for professional activity? A Role for learning new ‘languages’: A Role for learning new ‘languages’: Collecting and interpreting evidence (statistics; information science) Collecting and interpreting evidence (statistics; information science) Dealing with uncertainty (probability theory) Dealing with uncertainty (probability theory) Making decisions (economics and decision theory) Making decisions (economics and decision theory)
 Collecting and interpreting evidence (statistics; information science) Dealing with uncertainty (probability theory) Dealing with uncertainty (probability theory) Making decisions (economics and decision theory) Making decisions (economics and decision theory).")
19
‘Accept the fact of uncertainty and learn to live with it. Since no magic will provide certainty, our plans must be made without it’: Roberta Wohlstetter (1962) ‘There is nothing more profitable for a person than to take good counsel with oneself; for even if the event turns out contrary to one’s hopes, still one’s decision was right’: Herodotus
 ‘There is nothing more profitable for a person than to take good counsel with oneself; for even if the event turns out contrary to one’s hopes, still one’s decision was right’: Herodotus.")
Similar presentations