Download presentation
Presentation is loading. Please wait.

1
ICP management in Neurointensive Care

2
23 YO Male MVA, ejected from car Vitals are stabilized, NSGY consulted GCS 3T (E1 M1 V1T) Pupils sluggish to light CT Head
 Pupils sluggish to light CT Head")
4
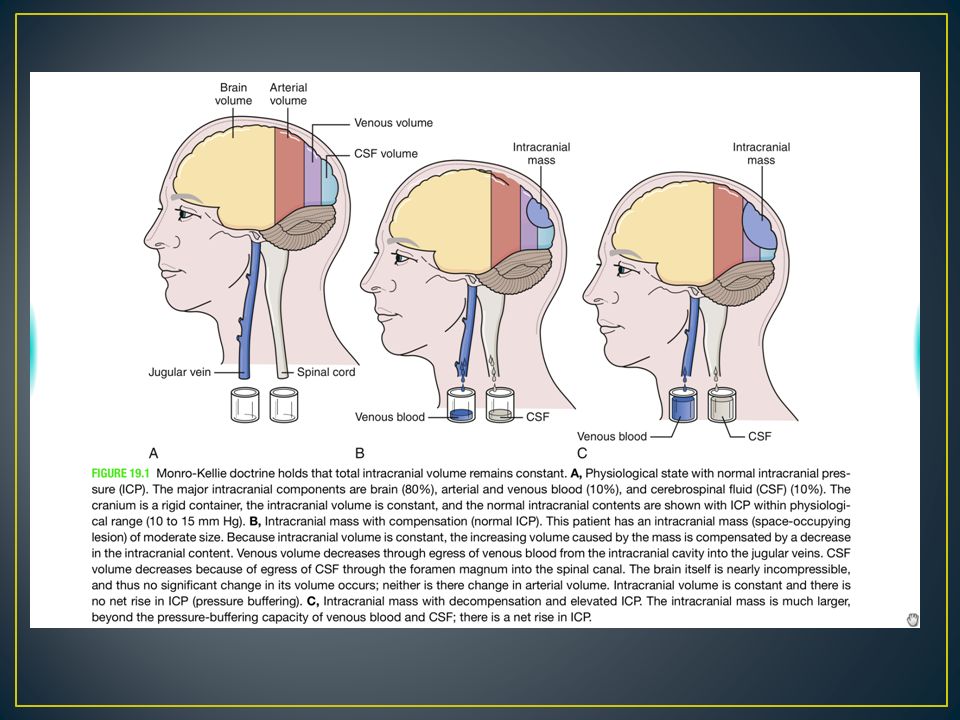
Cranium is a rigid structure Average Total Volume: 1700mL Exception: Children without fused sutures Contents: 80% Brain (70% parenchyma,10% interstitial fluid) 10% Blood 10% CSF New intracranial mass => compensatory change must occur
 10% Blood 10% CSF New intracranial mass => compensatory change must occur")
6
First venous system collapses Then CSF displaced from ventricular system into spinal subarachnoid space Once the above measures are maximized, small changes in volume => large increases in pressure

7
Compliance – dV/dP Accommodative potential of intracranial space Elastance – dP/dV Resistance to outward expansion Inverse of compliance Actually measured in clinical practice

8
Graph produced by placing a balloon in epidural space of a mouse and slowly inflating:

10
Altered level of consciousness with progressive neurological decline Obtundation due to: Compression of supramedullary reticular activating system Bithalamic or bicortical damage GCS <8 Irregular breathing Posturing Anisocoria

11
55 – 60ml/100g of Brain Tissue per minute 75mL/100g/min in gray matter 45mL/100g/min in white matter Ischemia at < 20mL/100g/min Infarction/Permanent Damage at below 10mL/100g/min Monitored by Cerebral Perfusion Pressure (CPP) MAP – ICP = CPP
 MAP – ICP = CPP")
12
Ability to maintain Cerebral Blow Flow over a wide range of CPPs (50-150 mmHg) Regulated by: CPP Arterial CO2 Arterial PO2 During the first 4-5 days of head trauma, disruption of autoregulation Likely a reason why a single episode of hypotension can lead to significantly worse outcomes
 Regulated by: CPP Arterial CO2 Arterial PO2 During the first 4-5 days of head trauma, disruption of autoregulation Likely a reason why a single episode of hypotension can lead to significantly worse outcomes")
13
Only way to measure ICP is directly Intraventricular catheter + manometer Fiberoptic transducer tipped catheter Placed within parenchyma or in subdural space Indications: Head Injury GCS between 3 and 8 Abnormal CT Scan

14
3 components Percussion Wave (P1) Tallest, peak cardiac systole transmitted throughout chorid plexus Tidal Wave (P2) Filling intracranial arteries with systolic blood with a resultant rebound increase in ICP Dicrotic Notch/Wave (P3) P2 > P1 when increased ICP
 Tallest, peak cardiac systole transmitted throughout chorid plexus Tidal Wave (P2) Filling intracranial arteries with systolic blood with a resultant rebound increase in ICP Dicrotic Notch/Wave (P3) P2 > P1 when increased ICP")
17
Care must be taken to not exacerbate pressure differences between compartments Cingulate Tentorial Central Tonsillar Upward

18
An early approach to induce hypertension to target CPP >70 mmHg using volume expansion and vasopressor agents appeared to reduce mortality and morbidity. Subsequent studies have suggested that this strategy does not improve outcome and rather risks severe extra-cerebral complications such as acute respiratory distress syndrome According to guidelines published in 2007, the recommended CPP target is 60 mmHg, avoiding levels below 50 mmHg and above 70 mmHg. In children these thresholds may be lower, 40 to 65 mmHg Efforts to optimize CPP should first treat and maintain ICP at low levels when possible. Patients with more severely impaired autoregulation in particular may be more likely to respond to efforts to lower ICP than to hypertensive-focused CPP therapy

20
Elevate head of bed at 30-45 degrees, head/neck not “kinked” Promote venous drainage Normothermia Elevated brain temperature increases metabolism => increased ICP and promotes ischemia Sedation and Analgesia Propofol most commonly used Quick “on-off” Lowers cerebral metabolism Infusion rate not exceed 4 mg/kg per hour and that patients be monitored for ECG changes, lactic acidosis, and elevations in creatinine kinase and myoglobin

21
Most direct way to normalize high ICP is to eliminate its cause Reduce mass effect Evacuate hematoma Bone flap removed Dura opened Skin closed and brain is allowed to expand

22
Controversial area Employ when failure of medical management

26
Blood-brain barrier Astrocytic foot processes wrapping around capillary endothelium composed of tight junction Transport Lipid soluble materials usually cross passively Amino Acids and Sugars have specific transporters Reflection coefficient – measurement of how easily something diffuses across BBB 0 = complete passive diffusion 1 = no passive diffusion

27
Fall in ICP by reducing intracranial blood flow through vasoconstriction Sustained hyperventilation in acute Intracranial HTN has not been found to be beneficial Can promote ischemia and contraindicated for prolonged use Reduce CO2 between 30 to 35 mmHg

28
Osmotic agent universally used to treat cerebral edema Urea and glycerol used in the past Resulted in hemolysis and other adverse effects Immediate efficacy: Osmotic gradient => increases intravascular volume => increased cerebral flow => vasoconstriction through autoregulation (if intact) Delayed efficacy: cumulative effects of osmotic gradient draws fluid from brain interstitial space (if BBB intact)
 Delayed efficacy: cumulative effects of osmotic gradient draws fluid from brain interstitial space (if BBB intact)")
29
Given as bolus 0.25g – 1g/kg @ q4h – q6h Effective for 48-72 hours Reflection coefficient of 0.9 => slowly leaks into interstitial space => ineffective after 72 hours of continuous use

30
Mechanism similar to mannitol – osmotic gradient to draw fluid from interstitial space Reflection coefficient of saline is 1 => if BBB is intact, can be used for longer than 72 hrs Does not cause systemic diuretic effect

33
Small studies have compared mannitol and hypertonic saline in patients with TBI: In one study (2005), nine patients received two treatments each of 200 mL 20 percent mannitol and 100 mL of 7.5 percent saline with 6 percent dextran-70 solution (HSD) in a random order. Median ICP reductions were greater with HSD than mannitol infusion (13 versus 7.5 mmHg). In another study(2003), 20 patients were randomly assigned treatment with either 20 percent mannitol or 7.5 percent hypertonic saline solution, each given as a dose of 2 mL/kg. The mean number and duration of recurrent elevated ICP episodes were higher in patients treated with mannitol than with hypertonic saline.
. In another study(2003), 20 patients were randomly assigned treatment with either 20 percent mannitol or 7.5 percent hypertonic saline solution, each given as a dose of 2 mL/kg. The mean number and duration of recurrent elevated ICP episodes were higher in patients treated with mannitol than with hypertonic saline..")
35
Given in 30mL bolus through a central line over 15 mins Single bolus does not alter Na concentrations Repeated use can cause electrolyte abnormalities

36
Furosemide has synergistic effect with mannitol Not dependent on intact BBB May also reduce CSF production

37
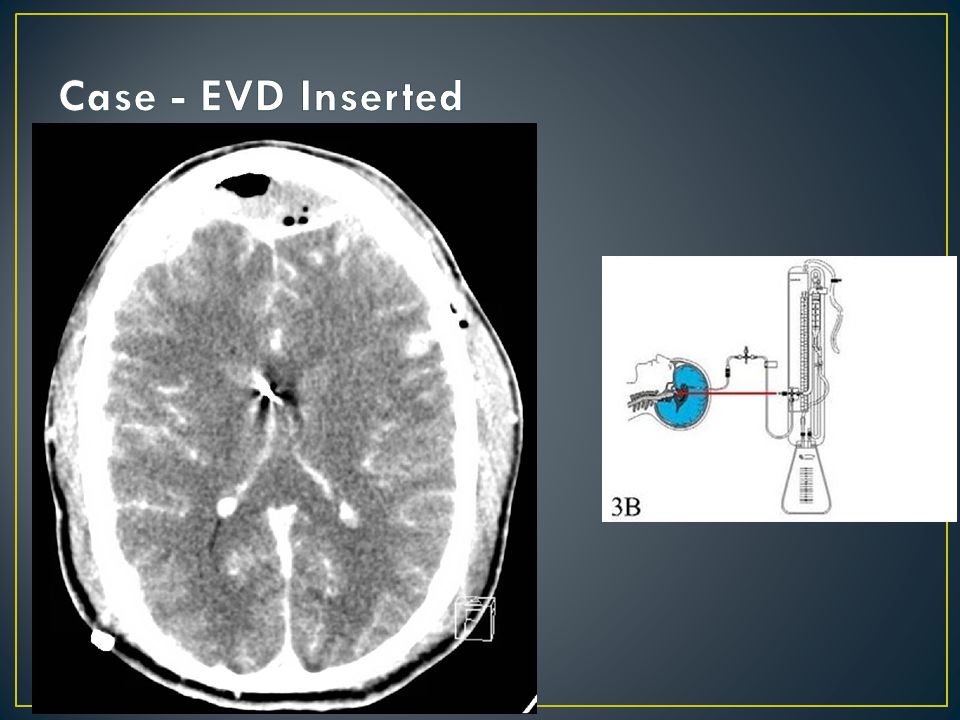
Used not only for monitoring but also for CSF drainage to externally control ICP Effective for: Acute subarachnoid hemorrhage Spontaneous/traumatic intraventricular hemorrhage

38
Decrease ICP by: Inhibit release of fatty acid perioxidation products by scavenging free radicals from mitochondria electron transport chain reaction Inhibit cerebral metabolism and cerebral blood flow Controversial – not much evidence supporting its use

40
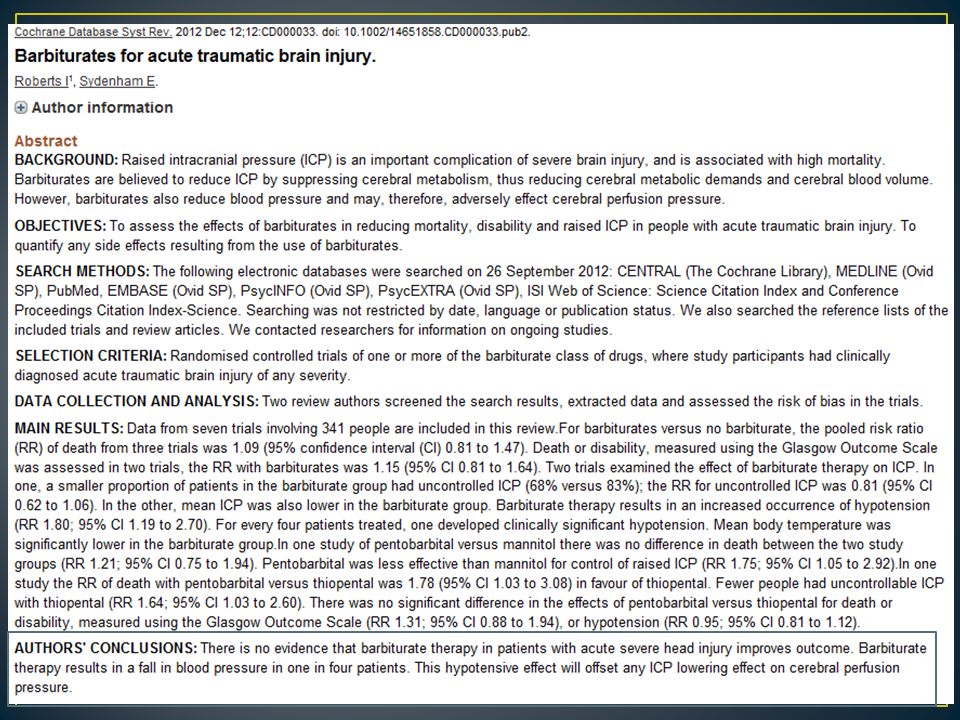
In a randomized trial of 73 patients with severe TBI, pentobarbital coma was associated with more effective ICP control compared to control treatment, but not improved 30- day mortality. Thiopental was compared to pentobarbital in a small study of 44 patients with TBI. While thiopental appeared more effective in terms of ICP control, conclusions drawn from this study are limited by its small size and an imbalance in baseline CT characteristics in the treatment groups. High-dose barbiturates often cause hypotension necessitating treatment with pressor agents

41
Pentobarbital remains a treatment option for elevated ICP refractory to other therapies. A loading dose of 5 to 20 mg/kg is given as a bolus, followed by 1 to 4 mg/kg per hour. Continuous EEG monitoring is used, with the pentobarbital infusion titrated to produce a burst-suppression pattern.

42
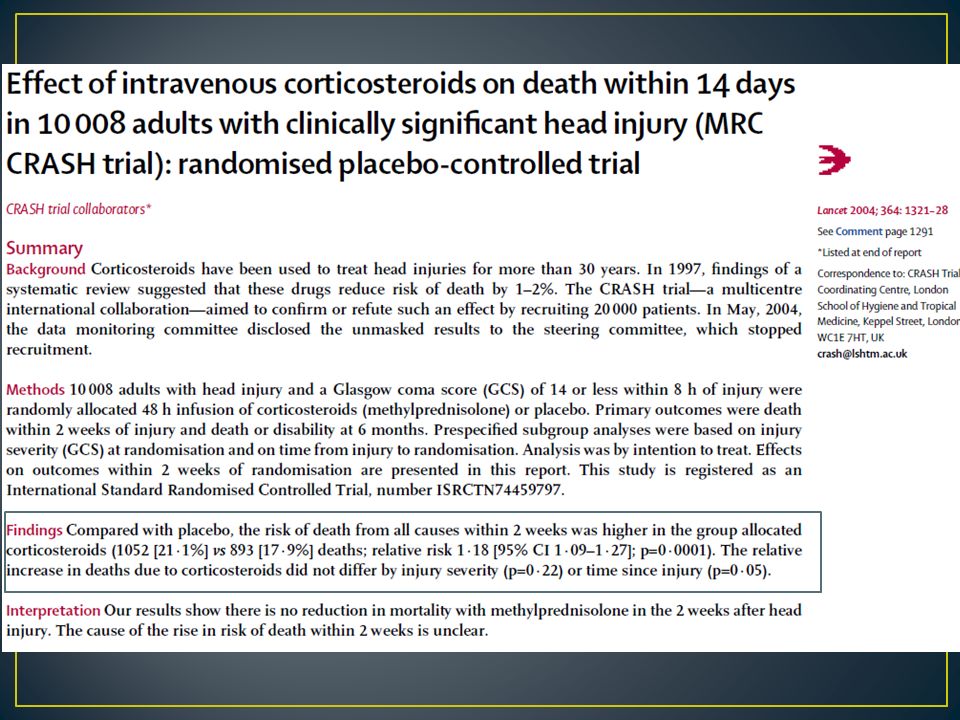
The use of a wide range of agents targeting various aspects of the TBI injury cascade has been tested in clinical trials. Currently, no neuroprotective agents or strategies (including induced hypothermia) have been shown to produce improved outcome. Based on a positive phase II studies, intravenous progesterone is being tested in a pivotal phase III clinical trial as a neuroprotective agent for severe head injury
 have been shown to produce improved outcome. Based on a positive phase II studies, intravenous progesterone is being tested in a pivotal phase III clinical trial as a neuroprotective agent for severe head injury.")
44
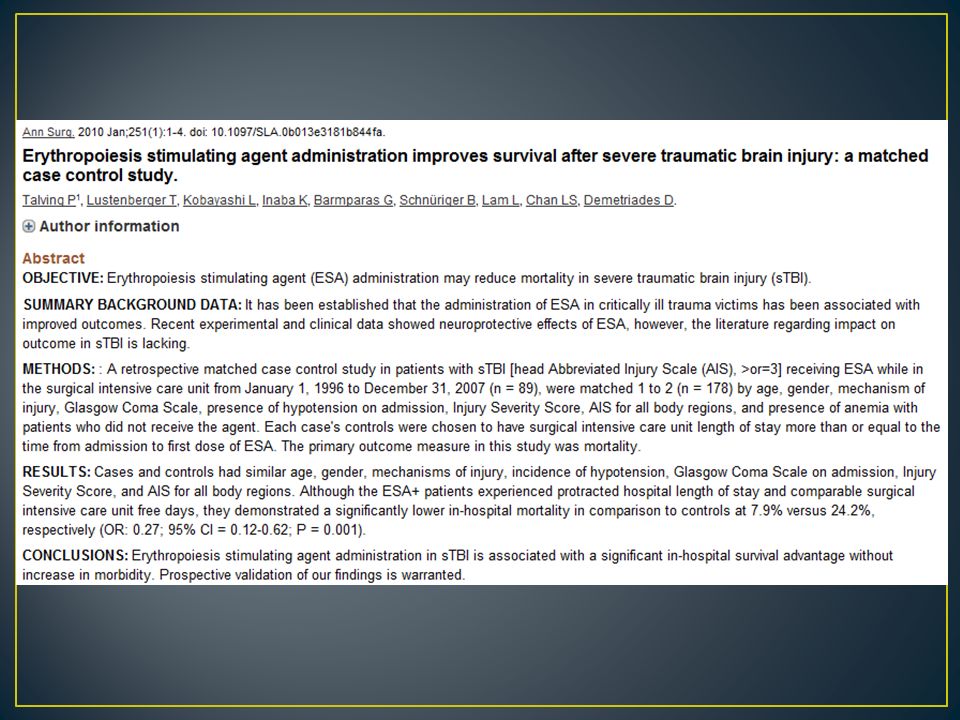
Erythropoietin has been postulated to have neuroprotective effects. In a retrospective case control study in 267 patients with severe TBI, matched for both GCS and severity of systemic injuries, in-hospital mortality was lower among 89 patients treated with erythropoietin compared with 178 control patients (8 versus 24 percent) Requires prospective validation in a clinical trial
 Requires prospective validation in a clinical trial.")
46
Other agents being investigated include magnesium, hyperbaric oxygen, and cyclosporine.

47
Jugular venous oximetry: retrograde cannulation of the internal jugular vein that allows measurement of oxygen saturation in the blood exiting the brain. Normal jugular venous oxygen saturation (SjVO2) is about 60 percent. SjVO2 <50 percent for 10 minutes is considered an "ischemic desaturation" and is associated with impaired CPP and worsened outcome. Brain tissue oxygen tension (PbtO2) monitoring: intraparenchymal oxygen electrode placed in a manner similar to a fiberoptic ICP probe that measures PbtO2 in the white matter. Normal PbtO2 is >20 mmHg; duration and depth of PbtO2 below 15 mmHg is associated with worsened outcome. One case series used oxygen supplementation to maintain PbtO2 above 25 mmHg and found better outcomes compared with historical controls. Cerebral microdialysis: intraparenchymal probe placed similarly to a PbtO2 probe that allows measurement of extracellular glucose, lactate, pyruvate, glutamate. A lactate:pyruvate ratio >40 is suggestive of anaerobic metabolism, which is believed to exacerbate secondary brain injury. Thermal diffusion flowmetry: intraparenchymal probe placed similarly to a PbtO2 probe that allows continuous measurement of CBF, usually in the white matter. Correlation with CBF from neuroimaging and outcome data is very preliminary at present.
 is about 60 percent. SjVO2 <50 percent for 10 minutes is considered an ischemic desaturation and is associated with impaired CPP and worsened outcome. Brain tissue oxygen tension (PbtO2) monitoring: intraparenchymal oxygen electrode placed in a manner similar to a fiberoptic ICP probe that measures PbtO2 in the white matter. Normal PbtO2 is >20 mmHg; duration and depth of PbtO2 below 15 mmHg is associated with worsened outcome. One case series used oxygen supplementation to maintain PbtO2 above 25 mmHg and found better outcomes compared with historical controls. Cerebral microdialysis: intraparenchymal probe placed similarly to a PbtO2 probe that allows measurement of extracellular glucose, lactate, pyruvate, glutamate. A lactate:pyruvate ratio >40 is suggestive of anaerobic metabolism, which is believed to exacerbate secondary brain injury. Thermal diffusion flowmetry: intraparenchymal probe placed similarly to a PbtO2 probe that allows continuous measurement of CBF, usually in the white matter. Correlation with CBF from neuroimaging and outcome data is very preliminary at present..")
50
Headache is most common complaint Generally worse in morning Increase in CO2 Increase in venous pressure Vomiting often without nausea CN6 Dysfunction Compression at petroclinoid ligament

51
Effective for vasogenic edema by stabilizing endothelial cell permeability Inhibit lysosomal activity Suppress polyunsaturated fatty acid production Decrease free radical production Loading dose of 10mg followed by 4mg q6h Needs to be tapered off if prolong use

53
Craniotomy Reduce the mass effect from tumor or chronic SDH Shunt Pseudotumor cerberi Hydrocephalus

54
GCS at presentation (especially the GCS motor score) Presence and severity of CT abnormalities (subarachnoid hemorrhage, cisternal effacement, midline shift) Pupillary function Age Associated injuries and complications Hypotension Hypoxemia Pyrexia Elevated ICP Reduced CPP Bleeding diathesis (low platelet count, abnormal coagulation parameters)
 Presence and severity of CT abnormalities (subarachnoid hemorrhage, cisternal effacement, midline shift) Pupillary function Age Associated injuries and complications Hypotension Hypoxemia Pyrexia Elevated ICP Reduced CPP Bleeding diathesis (low platelet count, abnormal coagulation parameters)")
55
Sedation, head of bed at 30 degrees, head “unkinked” Adjust minute ventilation for goal etCO2/PaCO2 30-35mmHg EVD or evacuation of mass lesion Medical osmotic therapy Mannitol 1g/kg dose then 23% hypertonic saline 30mL x1-4 dose Recurrent crisis: Manitol 0.5g/kg q6h alternating with 3% saline 250mL q6h with goal serum osm >320, Na > 155 Hemicraniectomy Barbiturate coma Paralysis or abdominal decompressive lapartomy – last resort

Similar presentations