Download presentation
Presentation is loading. Please wait.

1
MA STAAR Learning Session Completing the Transition into Skilled Nursing, Acute Rehabilitation, and Long Term Care Facilities Laurie Herndon and Kate Bones

2
Session Objectives Participants will be able to: Describe the role community providers can play in improving transitions in care Discuss specific strategies for enhancing care coordination with SNF, Acute Rehab, and LTC facilities

3
Transitions into SNF/LTC Facilities Small Group work: ─Describe how a patient and/or family member would (ideally) experience care as they transition into your setting (i.e., what they might want and need?) ─Identify three things that you will need to do in order to deliver that ideal system for your patients (i.e., processes that you will have to put in place) Report out on your discussions
 experience care as they transition into your setting (i.e., what they might want and need ) ─Identify three things that you will need to do in order to deliver that ideal system for your patients (i.e., processes that you will have to put in place) Report out on your discussions")
4
Digging In-Open Mind I. Perform an in-depth review of the last five rehospitalizations to identify opportunities for improvement Conduct chart reviews of the last five readmissions, transcribing key information onto the data collection sheets (see Diagnostic Worksheet A or INTERACT Quality Improvement Tool). Conduct interviews with patients recently readmitted and their family members (If possible, interview the same patients whose charts were reviewed). Next, conduct interviews with clinicians in the community who also know the readmitted patient (physicians, nurses in the skilled nursing facility, home care nurse, etc.) to identify problem areas from their perspective. Transcribe information from these interviews onto the data collection sheet (see Diagnostic Worksheet B).
. Conduct interviews with patients recently readmitted and their family members (If possible, interview the same patients whose charts were reviewed). Next, conduct interviews with clinicians in the community who also know the readmitted patient (physicians, nurses in the skilled nursing facility, home care nurse, etc.) to identify problem areas from their perspective. Transcribe information from these interviews onto the data collection sheet (see Diagnostic Worksheet B)..")
5
Lack of a clear picture of the resident’s entire history, including the severity of the resident’s condition and complications during hospitalization (e.g., C. difficile infection, pressure ulcers, urinary tract infection, delirium); Premature discharge from the hospital with unstable clinical condition Lack of an available primary provider who is familiar with the resident’s condition and treatment Lack of advance directives, palliative care services, and other types of care that prevent readmission to the hospital Inadequate availability and consistency of primary care providers for residents Opportunities Discovered through Diagnostics
; Premature discharge from the hospital with unstable clinical condition Lack of an available primary provider who is familiar with the resident’s condition and treatment Lack of advance directives, palliative care services, and other types of care that prevent readmission to the hospital Inadequate availability and consistency of primary care providers for residents Opportunities Discovered through Diagnostics.")
6
Transitions into SNF/LTC Facilities Small Group work: ─At your table, identify typical gaps in your clinical setting (3 or more!) ─What have you seen? What gets in the way of patients getting what they need? Report out on your discussions

7
Working Across the Continuum By understanding mutual interdependencies at each step of the patient journey across the care continuum, the team will codesign processes to improve transitions in care. Collectively, team members will explore the ideal flow of information and patient encounters as the patient moves from one setting to the next and then home. 29

8
Hospitals Perform an enhanced assessment of post-hospital needs Provide effective teaching and facilitate enhanced learning Ensure post- hospital care follow- up Provide real-time handover communications Office Practices Provide timely access to care following a hospitalization Prior to the visit: prepare patient and clinical team During the visit: assess patient and initiate new care plan or revise existing plan At the conclusion of the visit: communicate and coordinate ongoing care plan Home Care Meet the patient, family caregiver(s), and inpatient caregiver(s) in the hospital and review transition home plan Assess the patient, initiate plan of care, and reinforce patient self- management at first post-discharge home care visit Engage, coordinate, and communicate with the entire clinical team Skilled Nursing Facilities Ensure that SNF staff are ready and capable to care for the resident patient’s needs Reconcile the Treatment Plan and Medication List Engage the resident and their family or caregiver in a partnership to create an overall place of care Obtain a timely consultation when the resident’s condition changes
, and inpatient caregiver(s) in the hospital and review transition home plan Assess the patient, initiate plan of care, and reinforce patient self- management at first post-discharge home care visit Engage, coordinate, and communicate with the entire clinical team Skilled Nursing Facilities Ensure that SNF staff are ready and capable to care for the resident patient’s needs Reconcile the Treatment Plan and Medication List Engage the resident and their family or caregiver in a partnership to create an overall place of care Obtain a timely consultation when the resident’s condition changes")
9
Transition from Hospital to Home Enhanced Assessment Teaching and Learning Real-time Handover Communications Follow-up Care Arranged Post-Acute Care Activated MD Follow-up Visit Home Health Care (as needed) Social Services (as needed) Skilled Nursing Facility Services Hospice/Palliative Care Supplemental Care for High-Risk Patients * Transitional Care Models Intensive Care Management (e.g. Patient-Centered Medical Homes, HF Clinics, Evercare) or IHI’s Roadmap for Improving Transitions and Reducing Avoidable Rehospitalizations * Additional Costs for these Services Improved Transitions and Coordination of Care Reduction in Avoidable Rehospitalizations Patient and Family Engagement Cross-Continuum Team Collaboration Evidence-based Care in All Clinical Settings Health Information Exchange and Shared Care Plans
 or IHI’s Roadmap for Improving Transitions and Reducing Avoidable Rehospitalizations * Additional Costs for these Services Improved Transitions and Coordination of Care Reduction in Avoidable Rehospitalizations Patient and Family Engagement Cross-Continuum Team Collaboration Evidence-based Care in All Clinical Settings Health Information Exchange and Shared Care Plans.")
10
Improving Transitions into Skilled Nursing and Long Term Care Facilities Developing and Testing Changes to achieve an optimal reception (or return) into the skilled nursing or long- term care facility: 1.Assure SNF staff are ready and capable to care for the resident 2.Reconcile treatment plan and medications 3.Engage the resident and their family or caregiver in a partnership to create an overall plan of care 4.Provide timely consultation when a resident’s condition changes
 into the skilled nursing or long- term care facility: 1.Assure SNF staff are ready and capable to care for the resident 2.Reconcile treatment plan and medications 3.Engage the resident and their family or caregiver in a partnership to create an overall plan of care 4.Provide timely consultation when a resident’s condition changes")
11
1. Assure SNF Staff are Ready and Capable to Care for the Resident a.Develop mutually agreed upon standardized transfer criteria. b.Receive and confirm understanding of resident care needs from hospital staff. c.Resolve any questions regarding resident transition status to ensure fit between resident needs and SNF resources and capabilities. d.Identify an emergency clinician contact for the resident.

12
2. Reconcile Treatment Plan and Medications a.Re-evaluate the resident’s clinical status since transfer. b.Reconcile the treatment plan and medication list based on an assessment of the resident’s status, information from the hospital, and past knowledge of the resident (if applicable).
..")
13
a.Assess the resident’s and family or caregiver’s desires and understanding of the plan of care. b.Reconcile the care plan developed collaboratively with the resident and their family or caregiver. 3. Engage the Resident and Family/Caregiver in a Partnership to Create an Overall Plan of Care

14
a.Use protocols to guide immediate interventions with commonly occurring conditions and complications in the SNF 4. Obtain a Timely Consultation when Resident’s Condition Changes

15
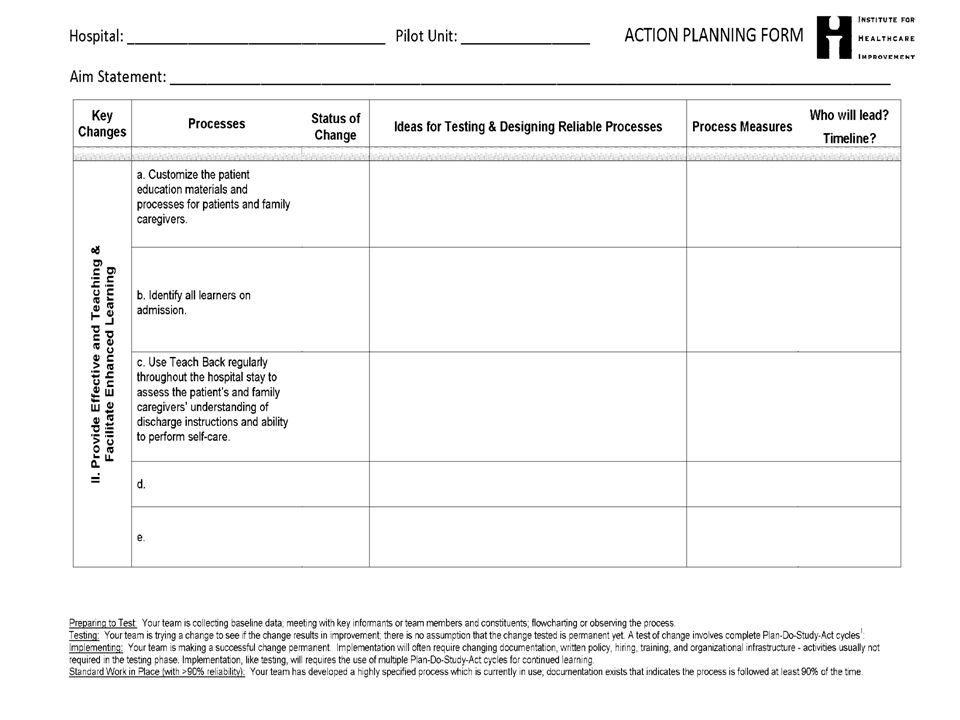
Your Turn to Plan Create your initial action plan using the ACTION PLANNING FORM Document plans for your first test of changes using the PDSA FORM

17
AP SD PDSA Worksheet Team Name: _ _________________ Cycle start date: _________ Cycle end date: __________ PLAN: Area to work on: Describe the change you are testing and state the question you want this test to answer (If I do x will y happen?) What do you predict the result will be? What measure will you use to learn if this test is successful or has promise? Plan for change or test : who, what, when, where Data collection plan : who, what, when, where DO: Report what happened when you carried out the test. Describe observations, findings, problems encountered, special circumstances. STUDY: Compare your results to your predictions. What did you learn? Any surprises? ACT: Modifications or refinements for the next cycle; what will you do next?

19
What is one new thing you learned today that you would like to test?

Similar presentations


>")


 Hospital/ED Schedule Patient Appointment.>")








![[Hospital Name | Presenter name and title | Date of presentation]](/19/5722524/big_thumb.jpg "[Hospital Name | Presenter name and title | Date of presentation]>")




