Download presentation
Presentation is loading. Please wait.

1
HELP! Is it Aphasia, Apraxia, Dysarthria or ALL of the Above??!!
Jamie L. Johnson, MA L/CCC-SLP University of Kansas Hospital September 24, 2015

2
During this session, participants will actively participate in discussing:
Different types of aphasia and dysarthria. Define dysarthria and apraxia. Evaluation in the acute and outpatient settings will be identified. The role of the SLP in education with family/friends for carryover into the home and community will briefly be discussed.

3
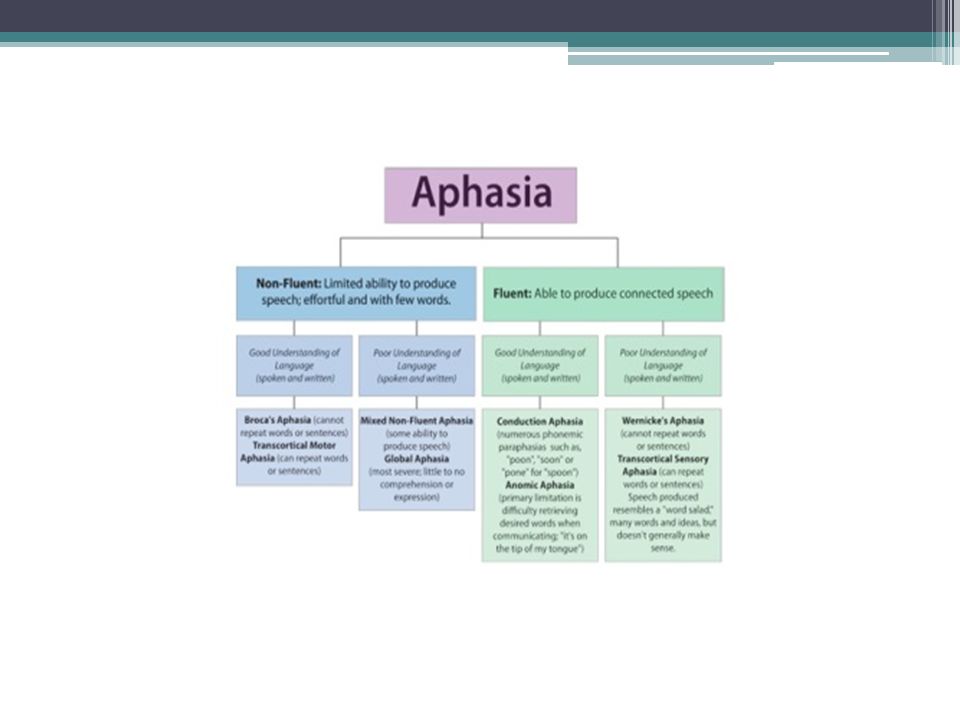
Aphasia National Aphasia Association

4
Aphasia Evidence Map

5
Standardized Evaluations
Purpose: Assess 4 modalities Classification Prognostic statement Treatment

6
Fluency Non-fluent 0-5 words Borderline fluent 6-8 words

7
Fluency Average of 3 longest phrases in response to
What happened to you Description of picture (cookie theft) Response to emotional question-”Tell me about your family.” “Do you remember what happened on 911?”
 Response to emotional question- Tell me about your family. Do you remember what happened on 911")
8
Standardized Evaluations
Classification WAB BDAE Non-classification MTDDA PICA Functional Assessment of Communication Skills for Adults (ASHA FACS) CADL Communication Effectiveness Index (CETI)-caregiver
 CADL. Communication Effectiveness Index (CETI)-caregiver.")
9
Screening Tests Frenchay Aphasia Screening Test (FAST)
Ullevaal Aphasia Test (UAST)
")
10
Others: ADP Boston Naming Test

11
SETTING DEPENDENT ACUTE INPATIENT REHAB OUTPATIENT SNF LTACH
HOME HEALTH

12
Standardized Evaluations
What do you use??

13
HOW ABOUT YOU Do you determine the type or classification of aphasia?

14
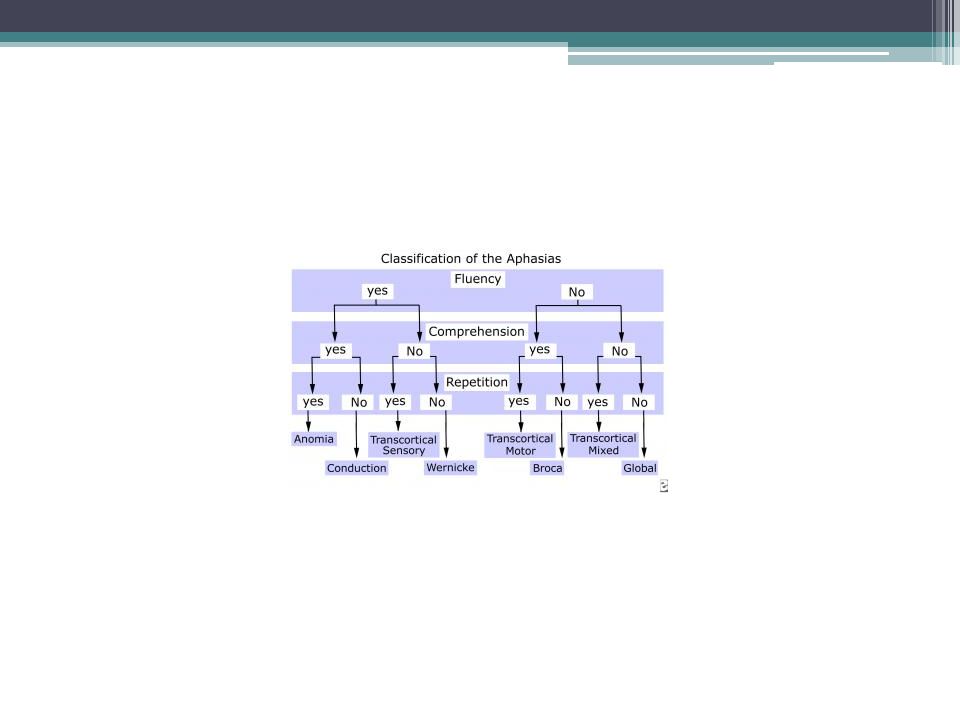
Type of Aphasia Fluent or Nonfluent Conversational Speech Auditory comprehension Repetition Naming Lesion Location Anomic Aphasia fluent Fluent, normal utterance length and well-formed sentences Good for everyday conversation, difficulty with complex syntax preserved Impairment is hallmark Acute – outside perisylvian zona (angular gyrus or inferior temporal region), chronic- perisylvian area, posterior tempolateral region Conduction Aphasia Fluent with normal utterance length but has paraphasias Good for casual conversation, difficult with complex syntax Impairment is hallmark, good spontaneous speech, paraphasias during repetition Always impaired Posterior perisylvian lesions affecting supramarginal gyrus in parietal lobe and arcuate fasciculus Transcortical sensory aphasia (TcSA) Fluent with normal utterance length, but semantic paraphasias, anomia Significantly impaired Preserved Severely impaired Extrasylvian regions involving POT junction region; posterior and deep to Wernicke’s area; sensory info doesn’t reach language areas Wernicke’s aphasia Fluent Fluent, easily articulated speech of normal utterance length, semantic and phonemic paraphasias, verbal output excessive and rapid but empty Severely impaired at single-word level, difficulty with complex syntax and multi-step commands, unaware of inability to produce coherent speech Significantly defective, cannot even repeat single words Paraphasic and severe anomia Large posterior perisylvian lesions encompassing Wernicke’s area and extending superiorly into inferior parietal region Transcortical motor aphasia (TcMA) Nonfluent Little attempt to produce spontaneous speech, mute, speech is reduced in length Good for most conversational interaction, difficulty with complex syntax Preserved, but absence of spontaneous speech Relatively preserved Extrasylvian regions of left frontal lobe; dorsolateral frontal lesions located anterior or superior to Broca’s area, supplementary motor areas, cingulate gyrus Broca’s aphasia Slow, halting speech production, utterances are of reduced length with simple grammar Good for conversational speech, difficulty with complex syntax Limited to single words and short phrases Impaired to some degree, especially for low frequency words Broca’s area causes transient disruption of speech production and fluency; persistent Broca’s aphasia from larger perisylvian lesions encompassing more of the left frontal lobe
, chronic- perisylvian area, posterior tempolateral region. Conduction Aphasia. Fluent with normal utterance length but has paraphasias. Good for casual conversation, difficult with complex syntax. Impairment is hallmark, good spontaneous speech, paraphasias during repetition. Always impaired. Posterior perisylvian lesions affecting supramarginal gyrus in parietal lobe and arcuate fasciculus. Transcortical sensory aphasia (TcSA) Fluent with normal utterance length, but semantic paraphasias, anomia. Significantly impaired. Preserved. Severely impaired. Extrasylvian regions involving POT junction region; posterior and deep to Wernicke’s area; sensory info doesn’t reach language areas. Wernicke’s aphasia. Fluent. Fluent, easily articulated speech of normal utterance length, semantic and phonemic paraphasias, verbal output excessive and rapid but empty. Severely impaired at single-word level, difficulty with complex syntax and multi-step commands, unaware of inability to produce coherent speech. Significantly defective, cannot even repeat single words. Paraphasic and severe anomia. Large posterior perisylvian lesions encompassing Wernicke’s area and extending superiorly into inferior parietal region. Transcortical motor aphasia (TcMA) Nonfluent. Little attempt to produce spontaneous speech, mute, speech is reduced in length. Good for most conversational interaction, difficulty with complex syntax. Preserved, but absence of spontaneous speech. Relatively preserved. Extrasylvian regions of left frontal lobe; dorsolateral frontal lesions located anterior or superior to Broca’s area, supplementary motor areas, cingulate gyrus. Broca’s aphasia. Slow, halting speech production, utterances are of reduced length with simple grammar. Good for conversational speech, difficulty with complex syntax. Limited to single words and short phrases. Impaired to some degree, especially for low frequency words. Broca’s area causes transient disruption of speech production and fluency; persistent Broca’s aphasia from larger perisylvian lesions encompassing more of the left frontal lobe.")
19
GLOBAL APHASIA VERBAL EXPRESSION COMPREHENSION REPETITION WRITING
NON-FLUENT Severely Impaired *Automatic speech may be preserved COMPREHENSION REPETITION Impaired WRITING READING COMPREHENSION LARGE LEFT DOMINANT LESION Involving Broca’s and Wernicke’s areas

20
BROCA’S APHASIA VERBAL EXPRESSION: COMPREHENSION: REPETITION WRITING
NON-FLUENT (4words or less) Slow effortful Perseverations “Telegraphic speech” COMPREHENSION: Relatively preserved REPETITION Poor WRITING Parallels expression READING COMPREHENSION Relatively spared ANTERIOR PORTION OF THE LEFT HEMISPHERE
 Slow effortful. Perseverations. Telegraphic speech COMPREHENSION: Relatively preserved. REPETITION. Poor. WRITING. Parallels expression. READING COMPREHENSION. Relatively spared. ANTERIOR PORTION OF THE LEFT HEMISPHERE.")
21
TRANSCORTICAL MOTOR APHASIA
VERBAL EXPRESSION NON-FLUENT AUDITORY COMPREHENSION: Intact REPETITION SIMILAR TO BROCA’S WITH ABILITY TO REPEAT Anterior and Superior to Broca’s area Watershed, borderzones

22
*MIXED NON-FLUENT Resembles Broca’s but auditory comprehension below 50 percentile. Auditory comprehension too good to be Global

23
WERNICKE’S APHASIA VERBAL EXPRESSION COMPREHENSION REPETITION
FLUENT Jargon, non-sensical words, rapid rate Retain sentences but lack meaning May speak with no insight into errors COMPREHENSION poor REPETITION Temporo-parietal involving Wernicke’s area and adjacent white matter

24
CONDUCTION APHASIA VERBAL EXPRESSION COMPREHENISON REPETITION RARE
FLUENT Word finding Paraphasic errors COMPREHENISON Relatively intact REPETITION Poor RARE ARCUATE FASCICULUS AND LEFT PARIETAL

25
TRANSCORTICAL SENSORY APHASIA
VERBAL EXPRESSION FLUENT Echolalia COMPREHENSION SIMILAR TO WERNICKE’S- EXCEPT STRONG ABILITY TO REPEAT REPETITION: Intact Watershed PCA/MCA territories, borderzones Spares Wernicke’s area

26
*MIXED TRANSCORTICAL APHASIA
COMBINATION OF THE TWO TRANSCORTICAL APHASIAS AUDITORY COMPREHENSION AND EXPRESSION SEVERELY IMPAIRED REPETITION INTACT

27
ANOMIC APHASIA VERBAL EXPRESSION COMPREHENSION REPETITION MILD FORM
FLUENT Word Finding problems Circumlocutes COMPREHENSION Intact USE OF NON-SPECIFIC WORDS SUCH AS “THING” REPETITION MILD FORM +Awareness

28
CROSSED APHASIA LANGUAGE CENTER NO IN EXPECTED HEMISPHERE
EX. RIGHT-HANDED PERSON WITH R CVA WITH APHASIA

29
Reading and Writing Alexia Alexia with Agraphia Agraphia

30
Paraphasias Neologism Perseveration Circumlocutions Literal/Phonemic
Verbal/Semantic Neologism Perseveration Circumlocutions

31
SUBCORTICAL APHASIA THALAMUS INTERNAL CAPSULE BASAL GANGLIA
MIRROR CORTICAL LESION APHASIAS CAN CO-OCCUR WITH CORTICAL APHASIAS

32
PRIMARY PROGRESSIVE APHASIA
GRADUAL LOSS OF LANGUAGE- PRESERVED MEMORY, VISUAL PROCESSING AND PERSONALITY- UNTIL THE END BEGINS WITH WORD FINDING PROGRESSES TO IMPAIRED GRAMMAR AND COMPREHENSION DYSARTHRIA AND APRAXIA MAY ACCOMPANY *STRUCTURAL & PHYSIOLOGICAL ABNORMALITIES IN LEFT HEMISPHERE (FRONTAL, PARIETAL AND TEMPORAL. NOT DUE TO NEOPLASTIC, VASCULAR OR METABOLIC ETIOLOGIES NOR INFECTION Semantic variant Logopenic variant Non-fluent Agrammatic variant

33
INSULA “The Role of the insula in Speech and Language Production” Oh, A. et al. Brain and Language 135 (2014) “Prime real estate” Responsible for articulatory control Direct connections to Broca’s area Higher order cognitive aspects of speech-language fMRI-exp/rec and production/ perception=Bilateral ant insula Speech perception Left dorsal mid- insula Expressive language tasks activated left ventral mid=insula Mid Insula plays different roles in S/L processing

34
MANY FACES OF APHASIA

36
Differential Diagnosis
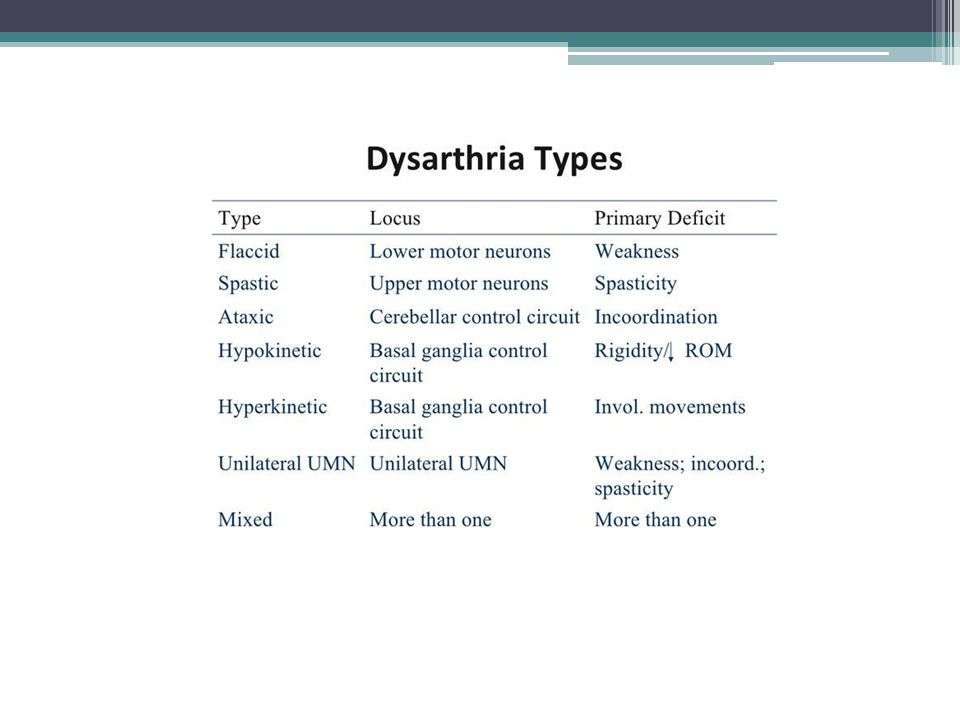
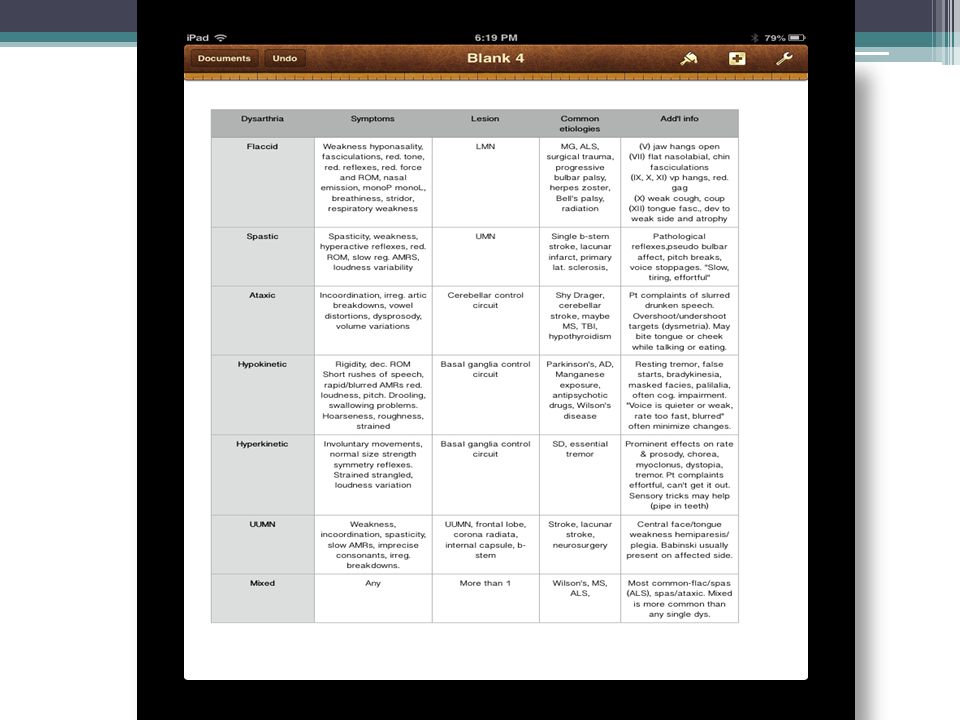
Motor Speech Disorders: Dysarthria Weakness/paralysis, incoordination, rigidity, involuntary movement Apraxia Motor planning problem Absence of weakness Initiation, groping, revisions, inconsistent

40
Apraxia of Speech Messages from the brain to the mouth are disrupted, and the person cannot move his or her lips or tongue to the right place to say sounds correctly, even though the muscles are not weak. Apraxia can occur in conjunction with dysarthria or aphasia Caused by damage to the parts of the brain that control coordinated muscle movement

41
Signs or Symptoms of Apraxia of Speech
Know what words they want to say, but their brains have difficulty coordinating the muscle movements necessary to say all the sounds in the words. Individuals with apraxia may demonstrate: Difficulty imitating and producing speech sounds Sound distortions, substitutions, and/or omissions Inconsistent speech errors Groping of the tongue and lips to make specific sounds and words Slow speech rate Impaired rhythm and prosody (intonation) of speech Better automatic speech than purposeful speech Inability to produce any sound at all in severe cases. Frustrating
 of speech. Better automatic speech than purposeful speech. Inability to produce any sound at all in severe cases. Frustrating.")
43
The faces of…dysarthria?......apraxia?

44
G CODES Modifier Impairment NOMS
0% WNL 7 1-20% MIN 6 MILD 5 40-60% MILD-MOD 4 60-80% MODERATE 3 80-99% MOD-SEVERE 2 100% SEVERE 1

45
NOMS MOTOR SPEECH LEVEL 1: The individual attempts to speak, but speech cannot be understood by familiar or unfamiliar listeners at any time. LEVEL 2: The individual attempts to speak. The communication partner must assume responsibility for interpreting the message, and with consistent and maximal cues, the patient can produce short consonant-vowel combinations or automatic words that are rarely intelligible in context. LEVEL 3: The communication partner must assume primary responsibility for interpreting the communication exchange, however, the individual is able to produce short consonant-vowel combinations or automatic words intelligibly. With consistent and moderate cueing, the individual can produce simple words and phrases intelligibly, although accuracy may vary. LEVEL 4: In simple structured conversation with familiar communication partners, the individual can produce simple words and phrases intelligibly. The individual usually requires moderate cueing in order to produce simple sentences intelligibly, LEVEL 5: The individual is able to speak intelligibly using simple sentences in daily routine activities with both familiar and unfamiliar communication partners. The individual occasionally requires minimal cueing to produce more complex sentences/messages in routine activities, although accuracy may vary and the individual may occasionally use compensatory strategies. LEVEL 6: The individual is successfully able to communicate intelligibly in most activities, but some limitations in intelligibility are still apparent in vocational, avocational, and social activities. The individual rarely requires minimal cueing to produce complex sentences/messages intelligibly. The individual usually uses compensatory strategies when encountering difficulty. LEVEL 7: The individual’s ability to successfully and independently participate in vocational, avocational, or social activities is not limited by speech production. Independent functioning

46
NOMS SPOKEN LANGUAGE COMPREHENSION
LEVEL 1: The individual is alert, but unable to follow simple directions or respond to yes/no questions, even with cues. LEVEL 2: With consistent, maximal cues, the individual is able to follow simple directions, respond to simple yes/no questions in context, and respond to simple words or phrases related to personal needs. LEVEL 3: The individual usually responds accurately to simple yes/no questions. The individual is able to follow simple directions out of context, although moderate cueing is consistently needed. Accurate comprehension of more complex directions/messages is infrequent. LEVEL 4: The individual consistently responds accurately to simple yes/no questions and occasionally follows simple directions without cues. Moderate contextual support is usually needed to understand complex sentences/messages. The individual is able to understand limited conversations about routine daily activities with familiar communication partners. LEVEL 5: The individual is able to understand communication in structured conversations with both familiar and unfamiliar communication partners. The individual occasionally requires minimal cueing to understand more complex sentences/messages. The individual occasionally initiates the use of compensatory strategies when encountering difficulty. LEVEL 6: The individual is able to understand communication in most activities, but some limitations in comprehension are still apparent in vocational, avocational, and social activities. The individual rarely requires minimal cueing to understand complex sentences. The individual usually uses compensatory strategies when encountering difficulty. LEVEL 7: The individual’s ability to independently participate in vocational, avocational, and social activities are not limited by spoken language comprehension. When difficulty with comprehension

47
NOMS SPOKEN LANGUAGE EXPRESSION
LEVEL 1: The individual attempts to speak, but verbalizations are not meaningful to familiar or unfamiliar communication partners at any time. LEVEL 2: The individual attempts to speak, although few attempts are accurate or appropriate. The communication partner must assume responsibility for structuring the communication exchange, and with consistent and maximal cueing, the individual can only occasionally produce automatic and/or imitative words and phrases that are rarely meaningful in context. LEVEL 3 The communication partner must assume responsibility for structuring the communication exchange, and with consistent and moderate cueing, the individual can produce words and phrases that are appropriate and meaningful in context. LEVEL 4: The individual is successfully able to initiate communication using spoken language in simple, structured conversations in routine daily activities with familiar communication partners. The individual usually requires moderate cueing, but is able to demonstrate use of simple sentences (i.e., semantics, syntax, and morphology) and rarely uses complex sentences/messages. LEVEL 5: The individual is successfully able to initiate communication using spoken language in structured conversations with both familiar and unfamiliar communication partners. The individual occasionally requires minimal cueing to frame more complex sentences in messages. The individual occasionally self-cues when encountering difficulty. LEVEL 6: The individual is successfully able to communicate in most activities, but some limitations in spoken language are still apparent in vocational, avocational, and social activities. The individual rarely requires minimal cueing to frame complex sentences. The individual usually self-cues when encountering difficulty. LEVEL 7: The individual’s ability to successfully and independently participate in vocational, avocational, and social activities is not limited by spoken language skills. Independent functioning may occasionally include use of self-cueing.
 and. rarely uses complex sentences/messages. LEVEL 5: The individual is successfully able to initiate communication using spoken language. in structured conversations with both familiar and unfamiliar communication partners. The individual occasionally requires minimal cueing to frame more complex sentences. in messages. The individual occasionally self-cues when encountering difficulty. LEVEL 6: The individual is successfully able to communicate in most activities, but some. limitations in spoken language are still apparent in vocational, avocational, and social. activities. The individual rarely requires minimal cueing to frame complex sentences. The individual usually self-cues when encountering difficulty. LEVEL 7: The individual’s ability to successfully and independently participate in vocational, avocational, and social activities is not limited by spoken language skills. Independent. functioning may occasionally include use of self-cueing.")
48
NOMS READING WRITING

49
Education Family Training Staff Training Education materials Websites
Apps Home Programs Family/Caregiver’s role in Therapy in any setting

50
QUESTIONS???

51
REFERENCES Davis, G. (2007) Aphasiology: Disorders and Clinical Practice. pages Helm-Estabrooks, N. Albert, M.L., 1991, Manual of Aphasia and Aphasia Therapy. 2nd edition, Pro-Ed, Austin Texas. Johnson, A., Jacobson, B,(2006) Medical Speech Pathology: A Practitioner's Guide. Thieme Medical Publishers, New York, NY LaPointe, L. (2001 ) Aphasia and related Neurogenic Language Disorders. Thieme Medical Publishers, New York, NY Oh, A. et al. (2014) The Role of the Insula in Speech and Language Production Brain and Language. 135,
 Medical Speech Pathology: A Practitioner s Guide. Thieme Medical Publishers, New York, NY. LaPointe, L. (2001 ) Aphasia and related Neurogenic Language Disorders. Thieme Medical Publishers, New York, NY. Oh, A. et al. (2014) The Role of the Insula in Speech and Language Production Brain and Language. 135,")
Similar presentations










 Ling 411 – 05.>")



>")


![Disorders Fluent aphasias [3] Nonfluent aphasias [4] Pure aphasias [1] Watershed.](/14/4364138/big_thumb.jpg "Disorders Fluent aphasias [3] Nonfluent aphasias [4] Pure aphasias [1] Watershed.>")





