Download presentation
Presentation is loading. Please wait.

1
Congestive Heart Failure ADOPTED FROM: Jarrod Eddy, PGY2 Internal Medicine Sub-I Lecture Series ADOPTED FROM: Jarrod Eddy, PGY2 Internal Medicine Sub-I Lecture Series

3
Congestive Heart Failure Clinical presentation of disease NOT a diagnosis in and of itself Differential includes –Underlying cardiovascular disease –Precipitating factors Clinical presentation of disease NOT a diagnosis in and of itself Differential includes –Underlying cardiovascular disease –Precipitating factors

4
Predisposing Cardiac Diseases Myocardial infarction Chronic ischemia Cardiomyopathy Arrhythmias Diastolic dysfunction Valvular diseases –Aortic Stenosis –Mitral Stenosis –Mitral Regurgitation Myocardial infarction Chronic ischemia Cardiomyopathy Arrhythmias Diastolic dysfunction Valvular diseases –Aortic Stenosis –Mitral Stenosis –Mitral Regurgitation

5
Cardiac Physiology (remember this?) CO = SV x HR HR: parasympathetic and sympathetic tone SV: preload, afterload, contractility CO = SV x HR HR: parasympathetic and sympathetic tone SV: preload, afterload, contractility
 CO = SV x HR HR: parasympathetic and sympathetic tone SV: preload, afterload, contractility CO = SV x HR HR: parasympathetic and sympathetic tone SV: preload, afterload, contractility")
6
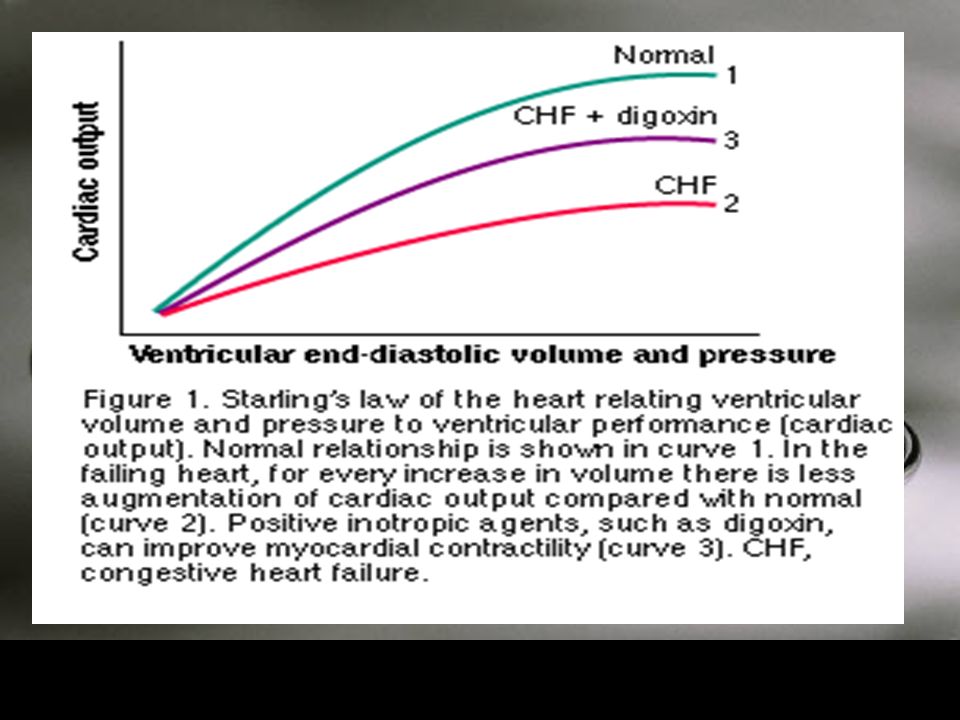
Preload Def: Passive stretch of muscle prior to contraction Measurement: Swan-Ganz –LVEDP Really a function of LVEDV Affected by compliance –Low compliance = higher LVEDP @ lower LVEDV –False high estimate of preload Frank-Starling right? Def: Passive stretch of muscle prior to contraction Measurement: Swan-Ganz –LVEDP Really a function of LVEDV Affected by compliance –Low compliance = higher LVEDP @ lower LVEDV –False high estimate of preload Frank-Starling right?

7
Afterload Def: Force opposing/stretching muscle after contraction begins Measurement: SVR Really a function of: –SVR –Chamber radius (dilated cardiomyopathies) –Wall thickness (hypertrophy) Def: Force opposing/stretching muscle after contraction begins Measurement: SVR Really a function of: –SVR –Chamber radius (dilated cardiomyopathies) –Wall thickness (hypertrophy)
 –Wall thickness (hypertrophy) Def: Force opposing/stretching muscle after contraction begins Measurement: SVR Really a function of: –SVR –Chamber radius (dilated cardiomyopathies) –Wall thickness (hypertrophy)")
8
Contractility Def: Normal ability of the muscle to contract at a given force for a given stretch, independent of preload or afterload forces In other words: –How healthy is your heart muscle? Ischemia, Hypertrophy (?), Muscle loss Def: Normal ability of the muscle to contract at a given force for a given stretch, independent of preload or afterload forces In other words: –How healthy is your heart muscle? Ischemia, Hypertrophy (?), Muscle loss
, Muscle loss Def: Normal ability of the muscle to contract at a given force for a given stretch, independent of preload or afterload forces In other words: –How healthy is your heart muscle. Ischemia, Hypertrophy ( ), Muscle loss.")
9
Classifying Heart Failure Anatomically –Left versus Right Physiologically –Systolic versus Diastolic Functionally –How symptomatic is your patient? Anatomically –Left versus Right Physiologically –Systolic versus Diastolic Functionally –How symptomatic is your patient?

10
Left versus Right Failure Left Heart Failure - Dyspnea - Dec. exercise tolerance - Cough - Orthopnea - Pink, frothy sputum Left Heart Failure - Dyspnea - Dec. exercise tolerance - Cough - Orthopnea - Pink, frothy sputum Right Heart Failure - Dec. exercise tolerance - Edema - HJR / JVD - Hepatomegaly - Ascites

11
Systolic versus Diastolic Systolic– “can’t pump” –Aortic Stenosis –HTN –Aortic Insufficiency –Mitral Regurgitation –Muscle Loss Ischemia Fibrosis Infiltration Systolic– “can’t pump” –Aortic Stenosis –HTN –Aortic Insufficiency –Mitral Regurgitation –Muscle Loss Ischemia Fibrosis Infiltration Diastolic- “can’t fill” –Mitral Stenosis –Tamponade –Hypertrophy –Infiltration –Fibrosis

12
Physical Exam no distress at rest, except for feeling uncomfortable when lying flat for more than a few minutes Decreased pulse pressure cool peripheral extremities and cyanosis of the lips and nail beds Increased jugular venous pressure Rales Hepatomegaly Peripheral edema no distress at rest, except for feeling uncomfortable when lying flat for more than a few minutes Decreased pulse pressure cool peripheral extremities and cyanosis of the lips and nail beds Increased jugular venous pressure Rales Hepatomegaly Peripheral edema

13
Clinical Data CXR –Kerley’s lines : A and B –Pulmonary Edema –Cephalization –Pleural Effusions (bilateral) EKG –Left atrial enlargement –Arrhythmias –Hypertrophy (left or right) CXR –Kerley’s lines : A and B –Pulmonary Edema –Cephalization –Pleural Effusions (bilateral) EKG –Left atrial enlargement –Arrhythmias –Hypertrophy (left or right)
 EKG –Left atrial enlargement –Arrhythmias –Hypertrophy (left or right) CXR –Kerley’s lines : A and B –Pulmonary Edema –Cephalization –Pleural Effusions (bilateral) EKG –Left atrial enlargement –Arrhythmias –Hypertrophy (left or right)")
14
Cardiomyopathy Pulmonary Edema

15
Clinical Data HEART SOUNDS!!! Systolic Murmurs –Mitral Regurg –Aortic Stenosis Diastolic Murmurs –Mitral Stenosis –Aortic Insufficiency S3: Rapid filling of a diseased ventricle HEART SOUNDS!!! Systolic Murmurs –Mitral Regurg –Aortic Stenosis Diastolic Murmurs –Mitral Stenosis –Aortic Insufficiency S3: Rapid filling of a diseased ventricle

16
Clinical Data Laboratory Data Chemistry –Renal Function: Be Wary BNP –Used in ER departments the world over –Good negative correlation –Need baseline for positivity –Pulmonary versus cardiac dyspnea Laboratory Data Chemistry –Renal Function: Be Wary BNP –Used in ER departments the world over –Good negative correlation –Need baseline for positivity –Pulmonary versus cardiac dyspnea

17
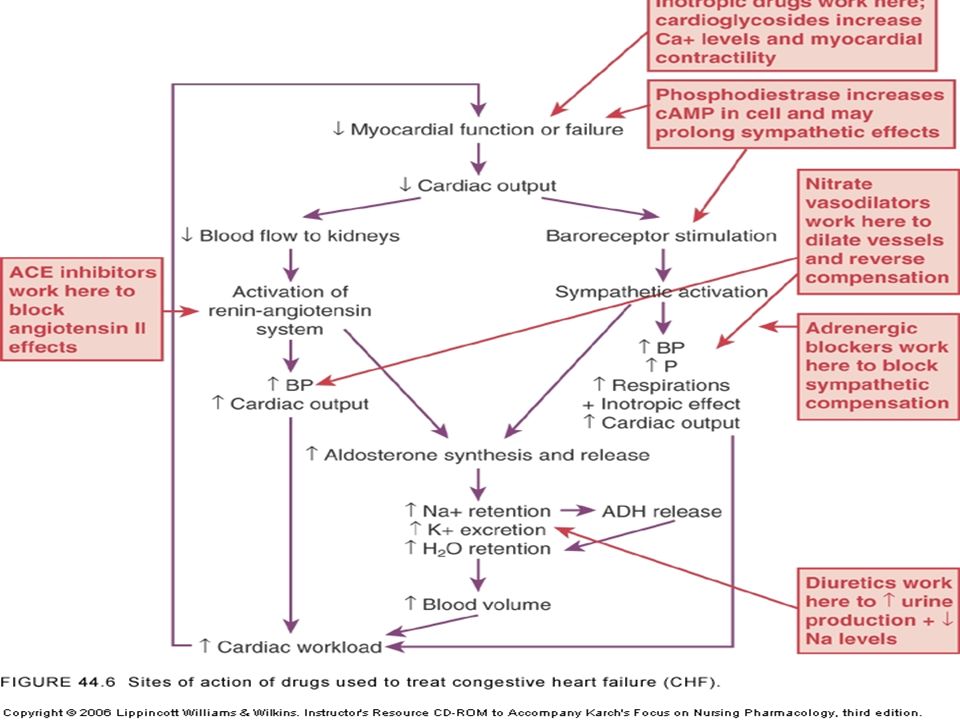
Treatment of CHF Treat Precipitating Factor(s)!!!! Adjust Heart Rate Decrease Preload Decrease Afterload Increase Contractility Increase Oxygenation Treat Precipitating Factor(s)!!!! Adjust Heart Rate Decrease Preload Decrease Afterload Increase Contractility Increase Oxygenation
!!!. Adjust Heart Rate Decrease Preload Decrease Afterload Increase Contractility Increase Oxygenation.")
19
Treatment of CHF Oxygen – nasal, BiPAP, intubation Morphine Preload Reduction –Loop diuretics –Nitrates –ACEi / ARB –Morphine Oxygen – nasal, BiPAP, intubation Morphine Preload Reduction –Loop diuretics –Nitrates –ACEi / ARB –Morphine

20
Treatment of CHF Afterload Reduction –IV NTG, Nitroprusside –Hydralazine –ACEi / ARB Ionotropic Support –Dopamine / Dobutamine –Amrinone / Milrinone –Digoxin (chronic) –Mechanical (ABP) Afterload Reduction –IV NTG, Nitroprusside –Hydralazine –ACEi / ARB Ionotropic Support –Dopamine / Dobutamine –Amrinone / Milrinone –Digoxin (chronic) –Mechanical (ABP)
 –Mechanical (ABP) Afterload Reduction –IV NTG, Nitroprusside –Hydralazine –ACEi / ARB Ionotropic Support –Dopamine / Dobutamine –Amrinone / Milrinone –Digoxin (chronic) –Mechanical (ABP)")
22
Treatment of CHF Beta-Blockers –Chronic > Acute –Carvedilol (Coreg), Metoprolol (Toprol XL) Fluid Balance –Restrict fluid / salt intake –Monitor I/Os and daily weight –Dialysis if needed Aspirin Beta-Blockers –Chronic > Acute –Carvedilol (Coreg), Metoprolol (Toprol XL) Fluid Balance –Restrict fluid / salt intake –Monitor I/Os and daily weight –Dialysis if needed Aspirin
, Metoprolol (Toprol XL) Fluid Balance –Restrict fluid / salt intake –Monitor I/Os and daily weight –Dialysis if needed Aspirin Beta-Blockers –Chronic > Acute –Carvedilol (Coreg), Metoprolol (Toprol XL) Fluid Balance –Restrict fluid / salt intake –Monitor I/Os and daily weight –Dialysis if needed Aspirin")
23
Precipitating Factors Infection Pulm Embolus Noncompliance Arrhythmia Myocardial Infarction Stress reaction Infection Pulm Embolus Noncompliance Arrhythmia Myocardial Infarction Stress reaction Sodium Intake Medications!!! Anemia Thyroid disorders Endocarditis

24
Admission Orders Admit: Telemetry or ICU EKG STAT, then daily x 3 days 2D Echo CXR Labs: BMP, CBC, CE x 3, Coags, LFTs, UA Pulse ox (ABG) Oxygen ASA 325mg PO daily Admit: Telemetry or ICU EKG STAT, then daily x 3 days 2D Echo CXR Labs: BMP, CBC, CE x 3, Coags, LFTs, UA Pulse ox (ABG) Oxygen ASA 325mg PO daily
 Oxygen ASA 325mg PO daily Admit: Telemetry or ICU EKG STAT, then daily x 3 days 2D Echo CXR Labs: BMP, CBC, CE x 3, Coags, LFTs, UA Pulse ox (ABG) Oxygen ASA 325mg PO daily")
25
Admission Orders Nitroglycerin –Paste: 1” ACW TID – Holding parameters –IV: 50mg in 250cc D5W – Titrate Morphine 1-5mg IV q10-20 min prn Lasix 20-200mg IV (q 6-8 hours) ACEi –Captopril 6.25-50mg PO q8h –Enalapril 2.5-20mg PO BID (0.625-2.5mg IV q6h) Hydralazine 10-100mg PO q6-8 h Nitroglycerin –Paste: 1” ACW TID – Holding parameters –IV: 50mg in 250cc D5W – Titrate Morphine 1-5mg IV q10-20 min prn Lasix 20-200mg IV (q 6-8 hours) ACEi –Captopril 6.25-50mg PO q8h –Enalapril 2.5-20mg PO BID (0.625-2.5mg IV q6h) Hydralazine 10-100mg PO q6-8 h
 ACEi –Captopril mg PO q8h –Enalapril mg PO BID ( mg IV q6h) Hydralazine mg PO q6-8 h Nitroglycerin –Paste: 1 ACW TID – Holding parameters –IV: 50mg in 250cc D5W – Titrate Morphine 1-5mg IV q10-20 min prn Lasix mg IV (q 6-8 hours) ACEi –Captopril mg PO q8h –Enalapril mg PO BID ( mg IV q6h) Hydralazine mg PO q6-8 h")
26
Admission Orders Beta Blocker –Probably not acutely –Start Coreg or Toprol XL prior to discharge Fluid Restrict 1000ml daily Low salt diet Daily patient weights Daily I/Os Beta Blocker –Probably not acutely –Start Coreg or Toprol XL prior to discharge Fluid Restrict 1000ml daily Low salt diet Daily patient weights Daily I/Os

27
Admission Orders Dobutamine 500mg in 250cc D5W –3-10ug/kg/min Digoxin –Probably not acutely –Titrate to effective dose prior to discharge IABP –Cardiogenic shock unresponsive to above tx Dialysis –Critical renal failure patients Dobutamine 500mg in 250cc D5W –3-10ug/kg/min Digoxin –Probably not acutely –Titrate to effective dose prior to discharge IABP –Cardiogenic shock unresponsive to above tx Dialysis –Critical renal failure patients

Similar presentations

 Brunner, ch. 30, pp. 824-840.>")








 Class IV: symptoms at rest Class III: symptoms on less-than-ordinary exertion Class.>")





. “Heart (or cardiac) failure is the pathophysiological state in which the heart is unable to pump blood at a rate commensurate.>")



