Download presentation
Presentation is loading. Please wait.

1
Pharmacy Quality Commitment A Way to Improve Patient Safety
Confidential Training Welcome to Pharmacy Quality Commitment Confidential Training brought to you by the Alliance for Patient Medication Safety – a federally listed Patient Safety Organization or PSO.

2
Agenda Overview of 2005 Patient Safety Act Discussion of Patient Safety Organizations Pharmacy Quality Commitment Quality Supervisor Quality Related Event (QRE) Quality Assurance (QA) Continuous Quality Improvement (CQI) Patient Safety Work Product (PSWP) We will discuss the patient safety act, briefly touch on what a Patient Safety Organization is and then dive into what Pharmacy Quality commitment is and how to implement it in your pharmacy First lets go over some acronyms and defintions that will be used in this presentation Quality Supervisor – the person in the pharmacy in charge of quality assurance and PQC Quality Related Event QRE – In the PQC program a QR is any breakdown in quality or error that occurs in the dispensing process whether it reached the patient or not Quality Assurance – refers to a program to ensure quality Continuous Quality Improvement – similar to quality assurance but note the word continuous Patient Safety Work product (PSWP) this refers to any and all of the data that is collected. It also refers to any work that results from analytics of the data – all your quality assurance work.
 this refers to any and all of the data that is collected. It also refers to any work that results from analytics of the data – all your quality assurance work.")
3
“We must accept human error as inevitable – and design around that fact.”
-Dr. Donald M. Berwick Former Administrator, Centers for Medicare and Medicaid Services (CMS) In the last years the attitude towards errors in healthcare providers has undergone a huge transformation
 In the last years the attitude towards errors in healthcare providers has undergone a huge transformation.")
4
Institute of Medicine Reports – there is a problem!
The Focus on Quality Institute of Medicine Reports – there is a problem! To Err is Human: Building a Safer Health System (1999) 7,000 deaths from medication errors Crossing the Quality Chasm: A New Health System for the 21st Century (2001) Patient Safety: Achieving a New Standard for Care (2003) Need for an information infrastructure Preventing Medication Errors: Quality Chasm Series (2006) At least 1.5 million ADEs occur each year The Institute of Medicine Reports showed we had a problem. Healthcare was NOT as safe as people thought. While there were many other studies that showed a need for an overhaul of the current safety program A red flag was raised. It pointed out that problems that exist which cause mistakes to inevitably occur are systems problems. Even if you remove the person who made an error, if the system remains the same, the next individual is set up to make the same mistake as well. Although we’ve recognized for years now the concept of systems problems, it is a slow change for all of health care to recognize that the system could be at fault and not the individual. These reports and others have had a huge impact on the way the healthcare industry and the public now perceives the safety of healthcare. They opened the door for frank discussions about errors in healthcare.
 7,000 deaths from medication errors. Crossing the Quality Chasm: A New Health System for the 21st Century (2001) Patient Safety: Achieving a New Standard for Care (2003) Need for an information infrastructure. Preventing Medication Errors: Quality Chasm Series (2006) At least 1.5 million ADEs occur each year. The Institute of Medicine Reports showed we had a problem. Healthcare was NOT as safe as people thought. While there were many other studies that showed a need for an overhaul of the current safety program A red flag was raised. It pointed out that problems that exist which cause mistakes to inevitably occur are systems problems. Even if you remove the person who made an error, if the system remains the same, the next individual is set up to make the same mistake as well. Although we’ve recognized for years now the concept of systems problems, it is a slow change for all of health care to recognize that the system could be at fault and not the individual. These reports and others have had a huge impact on the way the healthcare industry and the public now perceives the safety of healthcare. They opened the door for frank discussions about errors in healthcare.")
5
Patient Safety and Quality Improvement Act of 2005
Provided for the creation of Patient Safety Organizations (PSOs) and establishes Network Patient Safety Databases (NPSD). Patient Safety Act GOALS: Encourage Promote Share As a result of the reports and increasing public pressure the Patient Safety and Quality Improvement Act of 2005 was signed. The patient safety and quality improvement act was passed and provided for the creation of patient safety organizations (PSOs). It was an incredible step because it addressed the fear of healthcare of exposing collected patient safety data and established a framework for the future for all healthcare providers to share de-identified information across the board through a “Network of Patient Safety Databases” (NPSD). The goals of the Patient Safety Act are; To encourage the expansion of voluntary, provider-driven initiatives to improve the safety of health care To promote rapid learning about the underlying causes of risks and harms in the delivery of health care To share those findings widely, thus speeding the pace of improvement It was the intention of the legislation to encourage reporting by providing protections for quality assurance data and subsequent work with that data and for the PSOs to share anonymous data so that the entire healthcare community can learn from the huge body of information!
 and establishes Network Patient Safety Databases (NPSD). Patient Safety Act GOALS: Encourage. Promote. Share. As a result of the reports and increasing public pressure the Patient Safety and Quality Improvement Act of 2005 was signed. The patient safety and quality improvement act was passed and provided for the creation of patient safety organizations (PSOs). It was an incredible step because it addressed the fear of healthcare of exposing collected patient safety data and established a framework for the future for all healthcare providers to share de-identified information across the board through a Network of Patient Safety Databases (NPSD). The goals of the Patient Safety Act are; To encourage the expansion of voluntary, provider-driven initiatives to improve the safety of health care. To promote rapid learning about the underlying causes of risks and harms in the delivery of health care. To share those findings widely, thus speeding the pace of improvement. It was the intention of the legislation to encourage reporting by providing protections for quality assurance data and subsequent work with that data and for the PSOs to share anonymous data so that the entire healthcare community can learn from the huge body of information!")
6
Patient Safety Organizations: protect your QA data
PSOs are federally listed non-governmental organizations that collect QA data from members Operate independently, without a relationship to regulatory and/or accrediting bodies Benefits only extend to member pharmacies Duties to maintain confidentiality and security Duties to analyze data and provide feedback So…now healthcare providers (like pharmacists) could collect study and analyze AND “protect” their quality improvement data by working with a PSO. PSOs are non governmental organizations that get “reveiwed” by and listed by the Agency for Healthcare Reseach and Quality. The operate independently and contract with healthcare organizations. They are required to maintain strict Confidentiality and security and have a duty to analyze the clients data and provide feedback.
 could collect study and analyze AND protect their quality improvement data by working with a PSO. PSOs are non governmental organizations that get reveiwed by and listed by the Agency for Healthcare Reseach and Quality. The operate independently and contract with healthcare organizations. They are required to maintain strict Confidentiality and security and have a duty to analyze the clients data and provide feedback.")
7
Includes protections from:
PSO Protections Includes protections from: Discovery or Subpoena or FOI request or Evidence Federal, State, or local civil, criminal, or administrative subpoena or order, including disciplinary proceeding Limited disclosures allowed for certain criminal proceedings. If you are uncertain, an attorney should be consulted to help protect your privileges and rights. The data collected and analyzed, the resulting quality assurance work, all falls under Patient Safety work product – all is protected which includes protections from discovery, subpoena, or freedom of information requests.

8
What data is “discoverable”
PSO privileges do not protect: Patient's medical record Billing and discharge information Any other original patient or provider record Prescription vials, labels, dispensing documents Information collected, maintained, or developed separately, or exists separately, from a patient safety evaluation system PSO privileges do not protect the public record (read the first two)
")
9
Pharmacies need to have a program in place
Good business sense = protect patients AND business State CQI laws (13 states) CMS Requirement – 3rd Party Contracts Accreditation and Credentialing programs have CQI requirements Good Business sense – best offense is a good defense. Better to be able to say you have a safe medication safety program rather than say you just “careful”. Even better to work with a PSO - if you have a PSO then you can protect that patient safety data. State Laws – 11 states have CQI Laws CMS Requirement Pharmacies participating in Medicare Part D (each a “Pharmacy”) are required to sign certain attestations to satisfy mandatory compliance requirements related to guidance from the Centers for Medicare and Medicaid Services (“CMS”). CMS has set forth express guidance, logged in the Federal Register in 42 C.F.R. Parts 422 and 423, requiring Medicare Plan sponsors, or their delegates to demonstrate compliance with certain requirements in order to participate in the Medicare Part D Program. The Pharmacy’s quality assurance measures and systems must include all policies, procedures and disclosure protocols required by applicable federal and state laws, including but not limited to CMS regulations and guidance related to quality assurance measures and systems to assure continuous quality improvement. The Pharmacy’s continuous quality improvement (“CQI Program”) certification (“Certification”) is specifically used to attest that Pharmacy’s CQI Program meets all applicable laws including, without limitation, the requirements set forth by CMS Accreditation – Lots of talk about Accreditation and credentialing lately ACPE, Joint Commission, PCAB compounding, ACCP and URAC Reimbursement strategies looming on the horizon – they are in place in hospital settings, coming soon to pharmacies ALSO Public Initiatives Partnership for Patients and other groups
 CMS Requirement – 3rd Party Contracts. Accreditation and Credentialing programs have CQI requirements. Good Business sense – best offense is a good defense. Better to be able to say you have a safe medication safety program rather than say you. just careful . Even better to work with a PSO - if you have a PSO then you can protect that patient safety data. State Laws – 11 states have CQI Laws. CMS Requirement. Pharmacies participating in Medicare Part D (each a Pharmacy ) are required to sign certain attestations to satisfy mandatory compliance requirements related to guidance from the Centers for Medicare and Medicaid Services ( CMS ). CMS has set forth express guidance, logged in the Federal Register in 42 C.F.R. Parts 422 and 423, requiring Medicare Plan sponsors, or their delegates to demonstrate compliance with certain requirements in order to participate in the Medicare Part D Program. The Pharmacy’s quality assurance measures and systems must include all policies, procedures and disclosure protocols required by applicable federal and state laws, including but not limited to CMS regulations and guidance related to quality assurance measures and systems to assure continuous quality improvement. The Pharmacy’s continuous quality improvement ( CQI Program ) certification ( Certification ) is specifically used to attest that Pharmacy’s CQI Program meets all applicable laws including, without limitation, the requirements set forth by CMS. Accreditation – Lots of talk about Accreditation and credentialing lately. ACPE, Joint Commission, PCAB compounding, ACCP and URAC. Reimbursement strategies looming on the horizon – they are in place in hospital settings, coming soon to pharmacies. ALSO Public Initiatives. Partnership for Patients and other groups.")
10
What is a Medication Error?
The National Coordinating Council for Medication Error Reporting and Prevention (NCCMERP) Entire dispensing process Agency for Health Research and Quality (AHRQ) Incident = reaches patient Near miss Unsafe Condition Institute for Safe Medication Practices (ISMP) Error, Near miss and close call (error happened/not reached patient) Alliance for Patient Medication Safety (APMS) Quality-related event (incident, near miss and unsafe condition) What is a medication error? There is no nationally recognized definition of Error. Answer: A medication error is a breakdown or failure at any point in the medication use process: the long chain of events that is necessary for a medication to be prescribed and used effectively by a patient. There could be problems in choosing the drug prescribed, in ordering the drug, dispensing it, administering it or monitoring the drug once it’s taken. There could also be problems when the patient does not take the drug as directed. The Alliance for Patient Medication Safety (APMS) refers to errors and near misses as quality related events. While the definitions differ slightly all are common in that they agree that reporting near misses can help to evaluate whether the roadblocks and capture processes put in place are working well.
 Entire dispensing process. Agency for Health Research and Quality (AHRQ) Incident = reaches patient. Near miss. Unsafe Condition. Institute for Safe Medication Practices (ISMP) Error, Near miss and close call (error happened/not reached patient) Alliance for Patient Medication Safety (APMS) Quality-related event (incident, near miss and unsafe condition) What is a medication error There is no nationally recognized definition of Error. Answer: A medication error is a breakdown or failure at any point in the medication use process: the long chain of events that is necessary for a medication to be prescribed and used effectively by a patient. There could be problems in choosing the drug prescribed, in ordering the drug, dispensing it, administering it or monitoring the drug once it’s taken. There could also be problems when the patient does not take the drug as directed. The Alliance for Patient Medication Safety (APMS) refers to errors and near misses as quality related events. While the definitions differ slightly all are common in that they agree that reporting near misses can help to evaluate whether the roadblocks and capture processes put in place are working well.")
11
“No news” is NOT “good news”
Near miss capture = successful ability to avoid disaster What you do not measure, you cannot manage Errors are considered “normal” pathology. Humans are going to make mistakes, lets try to set up the processes to minimize the repercussions of those mistakes. Do not be lulled into thinking that because you are not capturing near misses that you do not make mistakes. The complex nature of the healthcare industry makes an error free environment just not possible. We must be on alert to search for opportunities to correct in our workflow and processes that which is not optimal. There is a maxium in business: We must Measuring to Manage - What You Do Not Measure, You Cannot Manage “No news is NOT good news” it just means you just don’t know! Near misses considered evidence of successful ability to avoid disaster

12
Swiss Cheese Effect = mistake/error Workflow Employees Equipment
Technology The Swiss Cheese Effect is one way of looking at any complex system such as the prescription filling process. In this example each slice of Swiss cheese represents a component of the prescription filling process, including pharmacy workflow, employees, equipment, technology, and other factors. We all have holes (make mistakes), but unlike the cheese our holes are constantly changing, opening, closing, and shifting location. This means we don’t make the same mistake each and every time. The mistake one person makes, may not be repeated again for another 5,000 prescriptions. A single hole (mistake) in any one slice (made by one person or one piece of equipment) does not normally cause an error, a bad outcome, or an adverse event. BUT, when the holes in many layers momentarily align, a situation arises that could allow an error to reach a patient- as depicted in this slide. (Click )The prescription filling process is designed with many layers so that a mistake can be caught before reaching the patient. Another way to look at it is that CQI programs help us to reduce the number of holes in our cheese, making it even more unlikely for a mistake to reach the patient.
, but unlike the cheese our holes are constantly changing, opening, closing, and shifting location. This means we don’t make the same mistake each and every time. The mistake one person makes, may not be repeated again for another 5,000 prescriptions. A single hole (mistake) in any one slice (made by one person or one piece of equipment) does not normally cause an error, a bad outcome, or an adverse event. BUT, when the holes in many layers momentarily align, a situation arises that could allow an error to reach a patient- as depicted in this slide. (Click )The prescription filling process is designed with many layers so that a mistake can be caught before reaching the patient. Another way to look at it is that CQI programs help us to reduce the number of holes in our cheese, making it even more unlikely for a mistake to reach the patient.")
13
Development of a CQI System: Blueprint
PLAN: Take a systems view (Policies and Procedures/Culture/Education) DO: Document all failures of quality (Collect the data) CHECK: Analyze data to identify opportunities to improve for the future (Review and meet with Staff) ACT: Implement changes (Educate staff on changes and test results) Repeat… The process improvement model most often used in healthcare is the PDCA method. This is the same model used in PQC. PLAN: Plan a change or test of how something works. Take a systems view, develop a policy and procedure decide what your goals are. DO: Carry out the plan. Document those failures of quality the errors that reach the patient AND the near misses CHECK: Look at the results. What did you find out? Analyze ACT: Decide what actions should be taken to improve. Implement those changes and follow up. Start again!
 DO: Document all failures of quality. (Collect the data) CHECK: Analyze data to identify opportunities to improve for the future. (Review and meet with Staff) ACT: Implement changes. (Educate staff on changes and test results) Repeat… The process improvement model most often used in healthcare is the PDCA method. This is the same model used in PQC. PLAN: Plan a change or test of how something works. Take a systems view, develop a policy and procedure decide what your goals are. DO: Carry out the plan. Document those failures of quality the errors that reach the patient AND the near misses. CHECK: Look at the results. What did you find out Analyze. ACT: Decide what actions should be taken to improve. Implement those changes and follow up. Start again!")
14
Pharmacy Quality Commitment®~ PQC
In store program pharmacies use in order to: Establish a quality conscious workflow Identify, collect, and report Quality Related Events (QREs) Analyze QREs to identify process improvement opportunities to improve workflow and decrease QREs The APMS PSO provides : Immediate access to the pharmacy’s reported patient safety data in chart and graph form Recommendations on best practices and workflow processes to help reduce medication errors, improve medication use, and enhance patient safety and health outcomes
 Analyze QREs to identify process improvement opportunities to improve workflow and decrease QREs. The APMS PSO provides : Immediate access to the pharmacy’s reported patient safety data in chart and graph form. Recommendations on best practices and workflow processes to help reduce medication errors, improve medication use, and enhance patient safety and health outcomes.")
15
PQC helps you….. Establish written CQI Policies and Procedures.
Ensure that staff CQI training and/or education is provided to all pharmacy personel Ensure that QREs are documented, reported, and analyzed WHY PQC??... PQC helps you establish a continuous quality improvement (CQI) program. After you log into the program you will see the Resource Area where all of the supporting documents and training can be found. PQC helps you…read slides Maintain security of patient safety data
 program. After you log into the program you will see the Resource Area where all of the supporting documents and training can be found. PQC helps you…read slides. Maintain security of patient safety data.")
16
CQI Verified Certificate
If you have completed the set up and trained the pharmacy the pharmacy will be able to generate a CQI verified certificate after it has reported QRE data using the online Quality Manager system at least one time per week for the last three consecutive weeks.

17
How to Start? A. Commitment to program (already have!)
B. Create culture of safety C. Develop Policy & Procedures/Standardization D. Institute process for collection, analysis and improvement cycle As Quality Supervisor you are in charge of implementing a CQI program in your pharmacy First you must commitment to program – you are here so hopefully A is checked off (A) Next is to create a culture of safety in your pharmacy - which we will discuss in the next 3 slides…(B) (C) You need to adopt QA policies and procedures, understand the Patient Safety Evaluation System (PSES) and Standardization (PQC program provides) And lastly (D)institute a process for collection analysis and improvement cycle – this part is the hardest part really as it is up to you to keep it going! So lets go through those next steps quickly.
 Next is to create a culture of safety in your pharmacy - which we will discuss in the next 3 slides…(B) (C) You need to adopt QA policies and procedures, understand the Patient Safety Evaluation System (PSES) and Standardization (PQC program provides) And lastly. (D)institute a process for collection analysis and improvement cycle – this part is the hardest part really as it is up to you to keep it going! So lets go through those next steps quickly.")
18
B. Create a Culture of Safety
For a continuous quality improvement program a positive safety culture must exist.

19
Culture of Safety Admit the possibility of failure even with familiar
well-designed processes Treat all errors/near misses as a symptom of system wide problem Use all errors/near misses as a learning opportunity Encourage and reward error and near-miss reporting The culture of safety comes from the top down. Staff must understand that to increase flow of information available for learning, encourage and reward error and near miss reporting. Leaders recognize that the value of remaining fully informed about safety is far greater than any perceived benefit from disciplinary action.

20
Discussing Errors Negative Positive Dwells on the past
Threatening, insulting, punitive Focuses on WHO made an error Concludes erring individual has character flaws they need to correct Individuals won’t willingly participate Positive Looks to the future Open, blame-free, non-punitive Focuses on HOW or WHAT in the system allowed error to occur Realizes error is a reality and recognizes the opportunities to improve for the future Creates blame-free, shame-free environment When discussing errors and near misses in your pharmacy, there are positive and negative techniques that can be employed. Which side of the slide has your pharmacy been on? Which side of the slide would you like your pharmacy to be on?

21
Self Assessment Resources
ISMP Medication Safety Self Assessment Tool AHRQ Pharmacy Survey on Patient Safety Culture htpp:// Semi-quantitative measures of the “current state” in each pharmacy. A Pharmacy self assessment can be employed to determine the culture and strengths and weaknesses within your pharmacy - here are 2 links

22
C. Develop Policies and Procedures/ Standardization
APMS provides QA Policies, the Patient Safety Evaluation System and lots of resources such standardized pharmacy workflow, workflow checklists and best practice recommendations. The Quality Supervisor will review all of this and make sure the staff is trained.

23
QA Policies and Procedures (in Resource Area)
Policy: Pharmacy will actively participate in Continuous Quality Improvement Designate an individual or individuals responsible for monitoring CQI Program compliance Identify and document QREs Minimize impact of QREs on patients Analyze data collected in response to QREs to assess causes and any contributing factors Use the findings of the analysis to formulate an appropriate response and develop pharmacy systems and workflow processes designed to prevent QREs Provide ongoing education Procedures: Employee Training Identification and Documentation of Quality Related Events Root Cause Analysis (Investigative Analysis) Process Improvements Records We provide a template for QA Policies and Procedures in the Resource Area after you log into your PQC site. Basically it outlines the process you will follow in regard to your ongoing quality program.
 Process Improvements. Records. We provide a template for QA Policies and Procedures in the Resource Area after you log into your PQC site. Basically it outlines the process you will follow in regard to your ongoing quality program.")
24
Patient Safety Evaluation System(PSES) (in Resource Area)
Basically….Review and sign. Educate Staff – Powerpoint in Resource Area WHEN: When and how patient safety data enters the PSES space WHERE: Where it is protected – “where the dome covers” WHO: Who works with the data WHAT: What data needs to be reported and what applies to it HOW: How you report and handle the data (Mark it all CONFIDENTIAL Patient Safety Work Product) Lets take a look at the Patient Safety Evaluation System – it is also referred to as the “compliance plan” that describes how your patient safety is collected, stored and protected. It defines what you are going to catch, record and keep data safe within your safety system and your methods to report to a Patient Safety Organization. This is another document that you can find in the Resource Area after log in. You and the pharmacy team members just need to understand that it exists and what it means. There is a Powerpoint and short test that you can take to make sure you understand. You can have the staff take it and document it on the training verification log. Think of the PSES as an dome. The Compliance Plan To make sure that all the data collected is protected, the PSES documentation must be able to show that all events were reported to the PSES and the PSO - none were stored outside of the PSES. WHEN: How information enters the PSES (Patient Safety Evaluation System) and when it is transferred to the PSO or functionally transferred to the PSO WHERE: What processes, activities, physical space(s) and equipment comprise the PSES – where PSWP(patient safety work product) is kept. Is it separate from non-PSWP and secure? ( its all the space from the counter and back) WHO: Identification of personnel who, or categories of personnel which, need access to patient safety work product to carry out their duties as they relate to the PSES. WHAT: Identification of the category of PSWP to which access is needed and any conditions appropriate to access. HOW: Procedures the PSES uses to report information to a PSO or disseminate information outside of PSES.
 Lets take a look at the Patient Safety Evaluation System – it is also referred to as the compliance plan that describes how your patient safety is collected, stored and protected. It defines what you are going to catch, record and keep data safe within your safety system and your methods to report to a Patient Safety Organization. This is another document that you can find in the Resource Area after log in. You and the pharmacy team members just need to understand that it exists and what it means. There is a Powerpoint and short test that you can take to make sure you understand. You can have the staff take it and document it on the training verification log. Think of the PSES as an dome. The Compliance Plan. To make sure that all the data collected is protected, the PSES documentation must be able to show that all events were reported to the PSES and the PSO - none were stored outside of the PSES. WHEN: How information enters the PSES (Patient Safety Evaluation System) and when it is transferred to the PSO or functionally transferred to the PSO. WHERE: What processes, activities, physical space(s) and equipment comprise the PSES – where PSWP(patient safety work product) is kept. Is it separate from non-PSWP and secure ( its all the space from the counter and back) WHO: Identification of personnel who, or categories of personnel which, need access to patient safety work product to carry out their duties as they relate to the PSES. WHAT: Identification of the category of PSWP to which access is needed and any conditions appropriate to access. HOW: Procedures the PSES uses to report information to a PSO or disseminate information outside of PSES.")
25
This is the schematic that illustrates the Patient Safety Evaluation System

26
You Can Fix the System No longer asking yourself this !
Organized workflow Use a systematic approach reduce the likelihood that a quality related event will be made “Now where was I?” Less likely to miss a step that could lead to an incident that reaches the patient Quality does not happen by chance, it is a result of quality habits Redundancy is positive Process ingrained Quality systems consist of an organized workflow. A systematic approach with checklists in place at each workflow station in the pharmacy, will reduce the likelihood that a mistake will be made. When you uncover weak spots in the dispensing process you can respond by Creating a system of double checks. These can be Will call checks and shift change checks. Develop a way to catch your errors and near misses and subsequently evaluation of those quality related events. (Think of the way the airline industry does it- they would never think of operating without checklists). When you operate this way, even if you are interrupted with a telephone call or a question, you are less likely to ask, “Now where was I?” You’re less likely to miss a step that could lead to an error. And if you do lose your place you can easily go back and go through the checklist to make sure. Quality does not happen by chance, it is a result of practicing your profession with quality habits. Complex systems can be more prone to accidents. In order to reduce accidents, systems can simplify and standardize the process, build in redundancy, and develop backup systems. Redundancy can be viewed as a negative word, but in these situations, redundancy is positive and helps reduce accidents or errors No longer asking yourself this ! 13
. When you operate this way, even if you are interrupted with a telephone call or a question, you are less likely to ask, Now where was I You’re less likely to miss a step that could lead to an error. And if you do lose your place you can easily go back and go through the checklist to make sure. Quality does not happen by chance, it is a result of practicing your profession with quality habits. Complex systems can be more prone to accidents. In order to reduce accidents, systems can simplify and standardize the process, build in redundancy, and develop backup systems. Redundancy can be viewed as a negative word, but in these situations, redundancy is positive and helps reduce accidents or errors. No longer asking yourself this ! 13.")
27
D. Institute process for collection, analysis and improvement cycle
Now we get to the Collection analysis and improvement cycle part of the program.

28
Collect! RECORD: Quality Related Events (QREs)
Incidents that reach the patient whether they caused harm or not Near Misses Unsafe Conditions Both are important to track and analyze Type, Who, What, Where, How, When and whether it reached the patient So what do you document? We are at the COLLECTION part of process for collection, analysis and improvement cycle This is a very important point. How many incidents that reach the patient cause harm? Very few. If they are all you track, then they will continue at that rate or slowly increase if systems to prevent them are not changed. However, if you track all QRE’s, incrementally change the systems, then QRE’s that reach the patient go down and even possibly away! APMS suggests that you track all major Quality Related Events. (Or QRE) A Quality Related Event is any failure of quality- sometimes it reaches a patient, and sometimes your system catches it before it reaches a patient, which is a near miss. Both errors and near misses are important to track and analyze in your pharmacy. Because your system caught a near miss, doesn’t mean it will be caught every time. By analyzing your data and determining where failures of quality are occurring, it allows you to identify areas in need of improvement to reduce the likelihood of the same thing happening again in the future. RECORD:
 A Quality Related Event is any failure of quality- sometimes it reaches a patient, and sometimes your system catches it before it reaches a patient, which is a near miss. Both errors and near misses are important to track and analyze in your pharmacy. Because your system caught a near miss, doesn’t mean it will be caught every time. By analyzing your data and determining where failures of quality are occurring, it allows you to identify areas in need of improvement to reduce the likelihood of the same thing happening again in the future. RECORD:")
29
#s and letters for easy recording
We provide an easy form for collecting. Here is a copy of the Daily Process Related Event Report Form. It is filled out from left to right using the menus found on the bottom of the form. #s and letters for easy recording

30
Completed Form Example
Fictional data for illustration purposes only Completed Form Example Here is one filled out. Left to right Menus on bottom.

31
Record QREs, THEN transfer to the internet to pharmacy’s PQC site
Go to Enter Username Enter Password

32
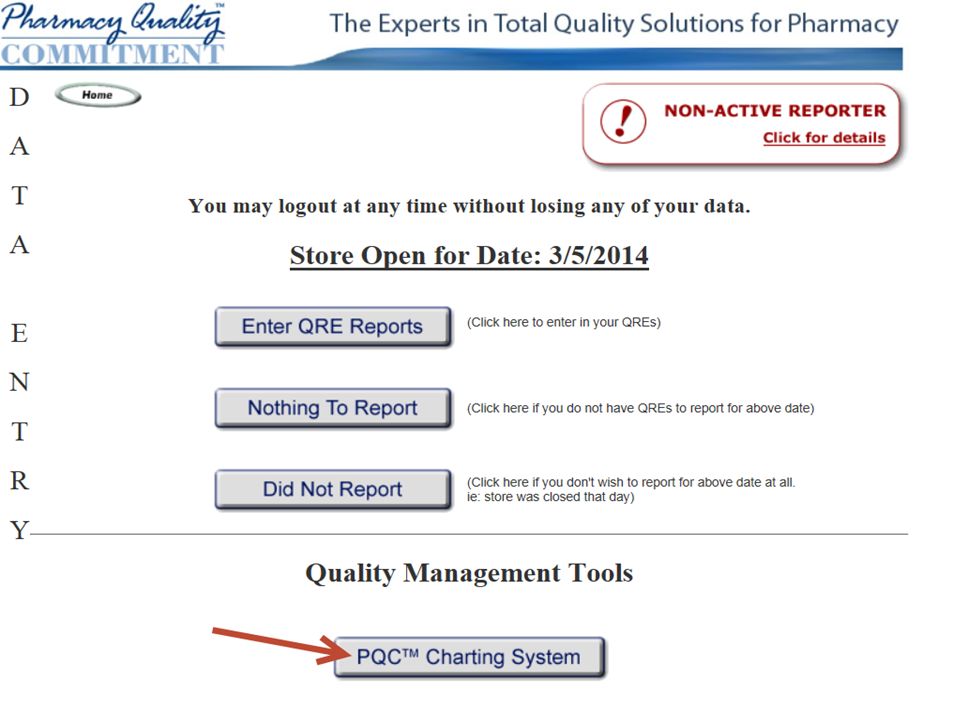
How do you enter the report?
To enter a report to the PSO go to Website Click on Login up at top upper right and log in

33
This will bring you to the Main Page
This will bring you to the Main Page. At the bottom of the page is the Resource Area – I have referred to this area several times. This is your library. It is where you can access the PQC Manual, the training, the forms and the newsletters. The information in the newsletters, trend data and best practice recommendations is devrived from the deidentified and aggregated reports of all of our pharmacies and examined for trending and lessons learned. For now, please turn your attention to the two grey buttons – it is here that you go to record a regular QRE or one related to compounding. There is a short powerpoint that goes into detail about the mechanics of reporting but I will demonstrate a quick overview right now. Click!

34
You have 3 choices. Record an event, report nothing or the 3rd choice SKIP the day ( did not report) If you have nothing to report that day choose nothing to report
 If you have nothing to report that day choose nothing to report.")
35
You will be asked to enter the number of prescriptions that you filled that day and click submit. This will CLOSE the store for the day.

36
If you have a QRE to record you click on Enter QRE Reports

37
An electronic form of the Process Related Event Report form will display. The red marks are where the drop down choices will appear. Fill out and submit.

39
Fictional data for illustration purposes only
The program takes all of the information that you report and display it in a variety of reports via charts and graphs. Here is a pie graph of TYPE of QRE reported. If you left click on one of the pieces of the display you get a spreadsheet view of it.

40
Review – to Report 1. Login 2. Enter report on correct day 3. Close your pharmacy each day (# of fills and refills) Many pharmacies have a technician enter the reports at the end of the week.

41
QRE’s We Collected QREs Now What?
You need to analyze to complete the cycle. Of course if you encounter a Quality Related Event that needs to be dealt with right away we know that it must be addressed immediately and not wait for the quarterly review.

42
How to analyze – questions to consider
Communication? Training provided? Had procedures been reviewed? Staffing? Work area? Policy & Procedure followed? When reviewing the data make sure that you examine the contributing factors Was communication between RPh and techs adequate? Was training provided, and monitored over time? Had procedures been reviewed to ensure a good match between people and tasks? Was there sufficient staff on hand for the workload at that time? Was the work area designed to support the function it was being used for? If Policy &Procedure were not used, what were the barriers to their usefulness to staff?

43
Intensive Investigation vs Root Cause Analysis
Peer Review – “Intensive Investigation” What happened? What happened on that particular day? Why did it happen? What made that particular day different? What usually happens? What should have happened according to policy and procedure? Fundamentally there are two types of retrospective analysis. 1. Intensive investigation and 2 Root Cause analysis. RCA is a formal rigorous structured diagnosis of a serious event or potential error Whereas Intensive Investigation is method that will be most useful for your CQI program Intensive Investigation gathers evidence of what happened with concise clear details and considers all the contributing factors. Its facutal,evidence-based, systems focused, non-puntive and quick minutes. Examine the process. Be sure to capture what actually happened, not what was supposed to have happened. Intensive Investigation vs Root Cause Analysis

45
Peer Review Gather Quality Related Event (QRE). Describe the QRE
WHAT happened? WHY? HOW? Identify possible failures in the systems. Identify possible contributing factors Where in workflow the QRE occurred Classify and record the causal factors and system failures. Identify improvement plans. What would prevent this error in the future? What will be monitored to assure that the corrective action is working? We provide many resources to help you tackle the peer review process from Peer review process forms to how to start a peer review process to how to hold a QA team meeting. All this can be found in the Resource Area after you log in. Gather Quality Related Event (QRE). Describe the QRE WHAT happened? WHY? HOW? Identify possible failures in the systems. (e.g. procedures, policies, equipment, workflow). Identify possible contributing factors. (e.g. environment and human performance factors). Where in workflow the QRE occurred. Classify and record the causal factors and system failures. Identify improvement plans. What would prevent this error in the future? What will be monitored to assure that the corrective action is working? Every pharmacy should have a current Quality Assurance Policy and Procedure that describes how the Peer Review process works, even in a small pharmacy with very few employees. The peer review work may be delegated to a pharmacist or experienced technician who has a special interest in safety and quality - the Quality Supervisor. The pharmacist-manager is ultimately responsible for the Continuous Quality Improvement program and for approving any corrective actions.
. Describe the QRE. WHAT happened WHY HOW Identify possible failures in the systems. (e.g. procedures, policies, equipment, workflow). Identify possible contributing factors. (e.g. environment and human performance factors). Where in workflow the QRE occurred. Classify and record the causal factors and system failures. Identify improvement plans. What would prevent this error in the future What will be monitored to assure that the corrective action is working Every pharmacy should have a current Quality Assurance Policy and Procedure that describes how the Peer Review process works, even in a small pharmacy with very few employees. The peer review work may be delegated to a. pharmacist or experienced technician who has a special interest in safety and quality - the Quality Supervisor. The pharmacist-manager is ultimately responsible for the Continuous Quality Improvement program and for approving any corrective actions.")
46
Remember

47
Process Improvement form
Date _______________ Results of Peer Review Process Process/Issue Identified Root Cause Identified Action Planned Date to be implemented Follow up analysis scheduled Results found at follow-up Patient Safety Work Product Privileged and Confidential Inadmissible as evidence and not subject to Discovery * MARK all process improvement notes as PSWP and Secure this information in safe place in pharmacy or report directly to PSO An example of a form to use when analyzing, brainstorming and planning improvement steps. There are forms in the Resource Area as well.

48
Actions and Changes Ideally will prevent the same event or minimize its occurrence Physical rather than procedural Install speed bumps instead of relying on speed limit sign Permanent rather than temporary Replace equipment known to malfunction in the hands of “float” staff, instead of taping warnings or additional instructions on machine Proposed actions should not burden people’s memory (i.e., “pay more attention next time”)
")
50
Review 1. Positive Safety Culture 2. Patient Safety Evaluation System 3. Policies and Procedures 4. Collect Data 5. Analyze Data 6. Implement New Process with Training Your continuous quality improvement program will consist of these elements.

51
Implementation Select Quality Supervisor Review the training Log in
Main Page > CQI Compliance Program Certification Enrollment Complete Steps Continue to report/Analyze Now we get to what everyone is waiting for…how do I get this started in my pharmacy? First Select the qualtiy supervisor. This could be you or someone you designate. The QA should review the manual the materials and the training. The step by step process and checklist can be found on the Main Page after you log in. You go to the CQI Compliance Program certification enrollment area and complete the steps.

52
Remember this page – the main page after you log in
Remember this page – the main page after you log in? The resource area is where all the materials can be found, but the checklist is found up top ( see the blue and read writing?) Click on the blue writing to access the page.
 Click on the blue writing to access the page.")
53
This page has a series of 7 boxes that you mark completed when you have finished. Once you feel that you CQI program is established click the first box to complete. 2nd box: download, read, amend, accept and print your CQI Policies and procedures

54
The 3rd and 5th box have to do with training
The 3rd and 5th box have to do with training . First HIPPA HiTech – this is a powerpoint training provided to remind staff that we must safeguard the data collected and the new hi tech rules apply. The 5th box is very important to your pharmacy. It explains the Patient Safety Evaluation System – It defines what you are going to catch, record and keep data safe within your safety system and your methods to report to a Patient Safety Organization. Why is that so important? This compliance plan is the legal document that you would use to show that you have a safe place for your data. Please review and accept this document. The two training boxes have tests associated with them – one person in the pharmacy needs to take the test and pass for the Pending to turn to Completed. The tests can then be taken over and over again – an answer key is provided. The quality supervisor is expected to make sure that the staff understands these training module and records the training. You can have the staff review the powerpoint presentations and take the tests, do a group training or do a train the trainer. There is a training documentation form found in the resource area. Note the red circle – this is where we get the most calls. This will not turn to complete unless you have reported (either nothing or somehting) at least once a week for the last consecutive 3 weeks. Once you stop reporting it will switch from Complete to pending until you catch up
 at least once a week for the last consecutive 3 weeks. Once you stop reporting it will switch from Complete to pending until you catch up.")
55
The top box on this page reminds the pharmacy to know their state requirements. APMS cannot and does not report QREs to any entity. If you have a mandate to report a QRE you may decide not to report it or mark it removed from the PSO ( instructions on how to do this are in the Quality Supervisor materials) Finally once all the boxes are checked you will be able to print a CQI verified certificate. Now your set up of the CQI program is complete – You just need to continue to report analyze and make process changes if necessary. Questions?

56
Contact APMS Web site PQC Web site Tara Modisett Executive Director APMS For assistance or questions us at or Toll free (866) Thank you for listening. We are ready to answer any questions that you have. Please contact us by phone or .
 Thank you for listening. We are ready to answer any questions that you have. Please contact us by phone or .")
Similar presentations


>")



” for each unit where.>")
 Job Hazard Analysis Mishap reporting 1 This class is only intended to familiarize you with the programs in place.>")







 Training UC Irvine’s Injury and Illness Prevention Program www.ehs.uci.edu.>")



>")

