Download presentation
Presentation is loading. Please wait.

1
Global Health. (Chpt 8) Unit 4. AOS 1.
 Unit 4. AOS 1.")
2
Key Knowledge and Key Skills. Key knowledge: Characteristics of developed and developing countries, Similarities and differences in health status and human development between developing countries and Australia in relation to morbidity, mortality, life expectancy, burden of disease and Human Development Index. The impact of these differences on health and devel. Key skills: Use, interpret and analyse data to draw informed conclusions about the health status and human development of developing countries compared to Australia

3
Something to think about.. If we could turn the population on Earth into a community of 100 people, keeping the proportions the same as we have today, it would look something like this: 50 would be female 50 would be male 26 would be children There would be 74 adults, 8 of whom would be 65 and older There would be: 60 Asians 15 Africans 14 people from the Americas 11 Europeans 33 Christians 22 Muslims 12 people who would not be aligned with a religion 83 would be able to read and write; 17 would not 7 would have a university degree 22 would own or share a computer 77 people would have a place to shelter them from the wind and the rain, but 23 would not 1 would be dying of starvation 15 would be undernourished 21 would be overweight 13 people would have no clean, safe water to drink 21 people would struggle to live on less than $1.25 a day

4
Global Health. Global health-refers to the health of populations in a worldwide context that goes beyond the perspectives and concerns of individual countries. Global health is about an international collaborative approach to achieving equity in health for all people worldwide.

5
Developing vs Developed countries. To determine whether a country is developed or developing, the following data is used: Morbidity Mortality Life expectancy Burden of disease Human Development Index http://www.youtube.com/watch?v=qb-3Ri5G2j4 http://www.youtube.com/watch?v=qb-3Ri5G2j4 You will need to be able to define these and identify and explain the differences seen in this data between developed and developing countries.

6
Developed countries Developed countries (also known as industrialised countries) are those with a well developed industry, mining or agriculture sectors, and which, therefore, enjoy a healthy economy based on trade. The gross domestic product (GDP) is a good indicator of how developed a country is. GDP= The total value of goods and services produced by a country in a year. Developed countries will have a high GDP.
 is a good indicator of how developed a country is. GDP= The total value of goods and services produced by a country in a year. Developed countries will have a high GDP..")
7
GDP per capita (per person)
")
8
Developed countries Developed countries also usually experience: longer life expectancy higher literacy and higher immunisation rates. What might be some reasons for the above trends?? As a result of their successful economies, developed countries usually have established healthcare and education systems in place which lead to the above. Examples of developed countries include Australia, New Zealand, the United States of America, Canada, Italy, Sweden, the United Kingdom and Japan, to name a few.

9
Characteristics of developed countries

10
Developing countries Developing countries, as the description suggests, are less developed and generally have a low gross domestic product. They have less access to technology, and have poor industry and limited trade arrangements. These nations tend to be characterised by: High rates of poverty Colonisation and international trade arrangements, War, conflict or natural disasters

11
Developing countries Compared to developed countries, developing countries experience: Shorter life expectancy Higher morbidity rates Lower literacy Lower immunisation rates. Factors that contribute to the characteristics of developing countries include: Low-income economy due to the export of relatively few agricultural or mineral products Limited healthcare facilities Low literacy rates And little in the way of social security systems

12
Developing countries Developing countries include: Afghanistan Bangladesh Cambodia China Guatemala Kenya Mozambique The Philippines Thailand Vanuatu Zimbabwe

13
World Health Organisation (WHO) Strata levels The WHO has divided the countries into 3 main categories: High mortality developing countries Low-mortality developing countries Developed countries. For analytical purposes only, WHO has further divided the countries into 5 mortality strata based on the country’s level of child and adult mortality.

14
(WHO) Strata levels Which strata levels do you think developed and developing countries fall under??
 Strata levels Which strata levels do you think developed and developing countries fall under")
15
Classification of Strata levels Strata A= Developed country Strata B & C= Difficult to label as these countries have low mortality but still face a number of barriers to their health status and economic development. Strata D & E= Developing countries.

16
Example question. Mexico is an example of a country in strata B where Uganda is in strata E. Why are there differences in terms of the strata countries are categorised into?

17
WHO regions The World Health Organization has also grouped countries into areas, known as the 6 WHO regions. These regions are based on geographical location and, therefore, each region may include both developing and developed countries. The six WHO regions are: 1 Western Pacific Region (e.g. Australia, NZ, PNG). 2 African Region (e.g. Kenya, Ethiopia). 3 Region of the Americas (e.g. Canada, USA, Brazil). 4 Eastern Mediterranean Region (e.g. Iraq, Jordan, Afghanistan). 5 European Region (e.g. UK, Germany, Hungary). 6 South-East Asia Region (e.g. India, Thailand).
. 2 African Region (e.g. Kenya, Ethiopia). 3 Region of the Americas (e.g. Canada, USA, Brazil). 4 Eastern Mediterranean Region (e.g. Iraq, Jordan, Afghanistan). 5 European Region (e.g. UK, Germany, Hungary). 6 South-East Asia Region (e.g. India, Thailand)..")
18
WHO regions

19
Note.. While the WHO regions are not required for the study of VCE Health and Human Development, knowledge of them will be very useful in assisting in the interpretation of data throughout the following chapters. You will however need to have a good understanding of the stratum levels.

20
The influence of colonialism, trade and debt Colonialism, trade and debt all play a role in contributing to the poverty and lower economic growth or income of developing countries. http://www.youtube.com/watch?v=ZUthgEXJugQ http://www.youtube.com/watch?v=ZUthgEXJugQ Colonialism- when a powerful country takes over a less powerful country and begins to rule that country. The country will generally take control of the resources, labour, and markets. (Taking most of the country’s income resulting in poverty for some developing countries)
.")
21
The influence of colonialism, trade and debt Trade- Is the export of goods. Many developing countries are dependent on exports for income. Developing countries generally have a small range of agricultural or mineral products for export. Debt-International debt has become a serious concern for many developing countries Debt is a barrier to many developing countries in being able to improve their health and education systems. Many developing countries are forced to spend more on repaying debt than on essential services. It is a constant cycle for many developing countries.

22
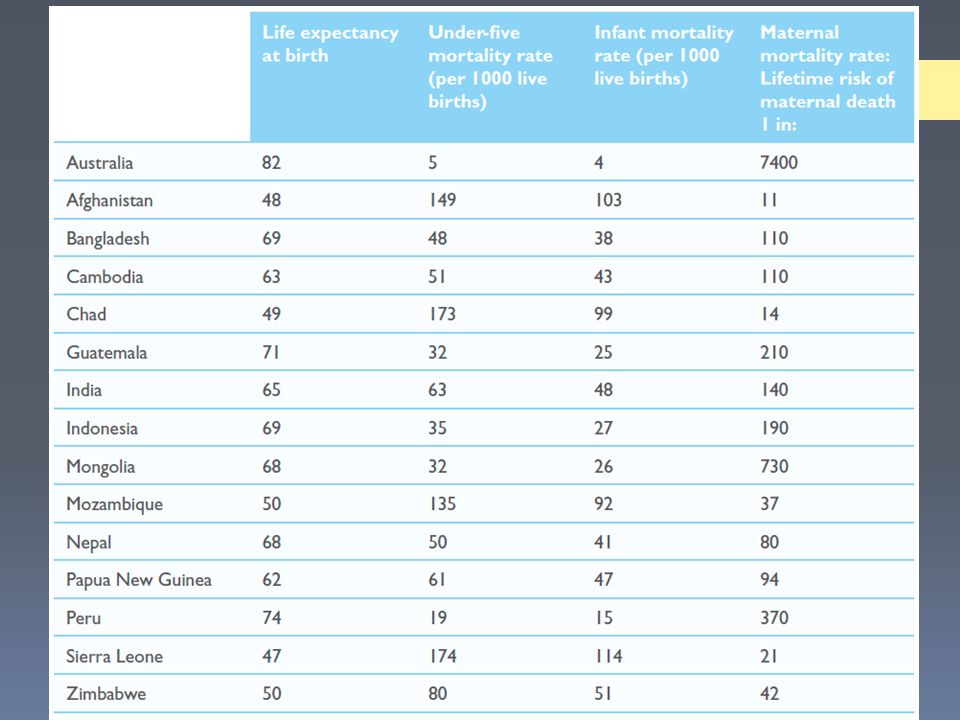
Comparing the health status of developing countries to Australia Measurements to identify the similarities and differences between Australia and developing countries: Life expectancy Mortality rates (under-five, infant and maternal) Morbidity Burden of disease The Human Development Index
 Morbidity Burden of disease The Human Development Index")
23
Life expectancy Life expectancy- an indication of how long a person can expect to live. Life expectancy at birth refers to the number of years a newborn child could be expected to live, based on current mortality rates for that country. For example, infants born in Australia in the year 2010 have an average life expectancy of 82 years. Whilst infants born in India have an average life expectancy of 65. http://gamapserver.who.int/gho/interactive_charts/mbd/life_expectancy/ atlas.html http://gamapserver.who.int/gho/interactive_charts/mbd/life_expectancy/ atlas.html

24
Life expectancy Activity 8.2 (pg 281) Country Year Life expectancy at birth Life expectancy at 60 Afghanistan19904914 20126016 Cambodia19905417 20127224 China19906918 20127519 Ghana19905716 20126217 India19905715 20126417 Kenya19905817 20125918 Pakistan19906017 20126517 Sudan19905516 20126317 Australia19907421 20128125
 Country Year Life expectancy at birth Life expectancy at 60 Afghanistan Cambodia China Ghana India Kenya Pakistan Sudan Australia")
25
Infant morality rates (IMR) Infant mortality rates refer to the number of deaths that occur in the first year of life. They are reported by the actual number of deaths per 1000 live births. Australia, like many other developed countries, has a low IMR compared to many developing countries. In 2010, the IMR in Australia was 4 per 1000 live births compared to 114 per 1000 live births in Sierra Leone in the same year. This relatively low IMR contributes to Australia’s life expectancy.

26
Infant morality rates (IMR)
")
27
Under-five mortality rates (U5MR) Refers to the number of deaths that occur in the first five years of life. They are reported by the actual number of deaths per 1000 live births. Every year, across the world, 7 million children die before their fifth birthday. Australia has a much lower U5MR than developing countries. In 2010: In Australia the U5MR was 5 per 1000 live births. In Sierra Leone, the U5MR was 174 per 1000 live births.

28
Actual number of under 5 MR (2010)
")
29
Under-five mortality rates (U5MR) The leading causes of U5MF differ significantly between countries. For example, in Australia in 2010, the leading cause of U5MR was congenital abnormalities (24%). In Sierra Leone, the leading cause of U5MR was malaria and pneumonia (23% and 17% respectively) What may be some reasons for this??
. In Sierra Leone, the leading cause of U5MR was malaria and pneumonia (23% and 17% respectively) What may be some reasons for this .")
30
Maternal mortality (MM) Complications arising during pregnancy and childbirth lead to the deaths of many women in developing countries. This is largely due to their lack of access to medical care at this time. E.g. In Afghanistan only 36% of pregnant women receive antenatal care during their pregnancy and only 24% have trained attendants at the birth. In contrast, close to 100% of women in Australia receive excellent antenatal care and have highly skilled attendants at birth It is this care that will provide women with immunisations, promote the importance of good nutrition, hygiene and adequate rest; and are likely to detect potential complications.

31
Maternal mortality (MM) Poor nutrition and continuing to work long hours before and after the birth also contribute to the high MM rate in developing countries. Rest is strongly encouraged and many women in Australia take time off in the lead up to the birth and a minimum 6 weeks off to recover after giving birth. As a result, the MM rate in Australia in 2010 was 8 per 100 000 live births. Would women in developing countries have these same rights??

33
Maternal Mortality http://www.youtube.com/watch?v=ayY-vSCr1Kg http://www.youtube.com/watch?v=ayY-vSCr1Kg

34
Causes of Mortality (Death) According to WHO, the leading causes of death in developing countries are associated with under nutrition. Causes of death such as perinatal conditions, diarrhoeal disease and infectious and parasitic diseases are also common causes of death in many developing countries. Perinatal condition- A condition effecting the baby in the period shortly before or after birth (up to 28 days after).
..")
35
Causes of Mortality Globally, the 5 leading causes of death are: Ischaemic heart disease Cerebrovascular disease Lower respiratory infections Chronic obstructive pulmonary disease Diarrhoeal diseases What do you think the 6 th leading cause may be?? HIV/AIDS is the 6 th leading cause of death globally.

36
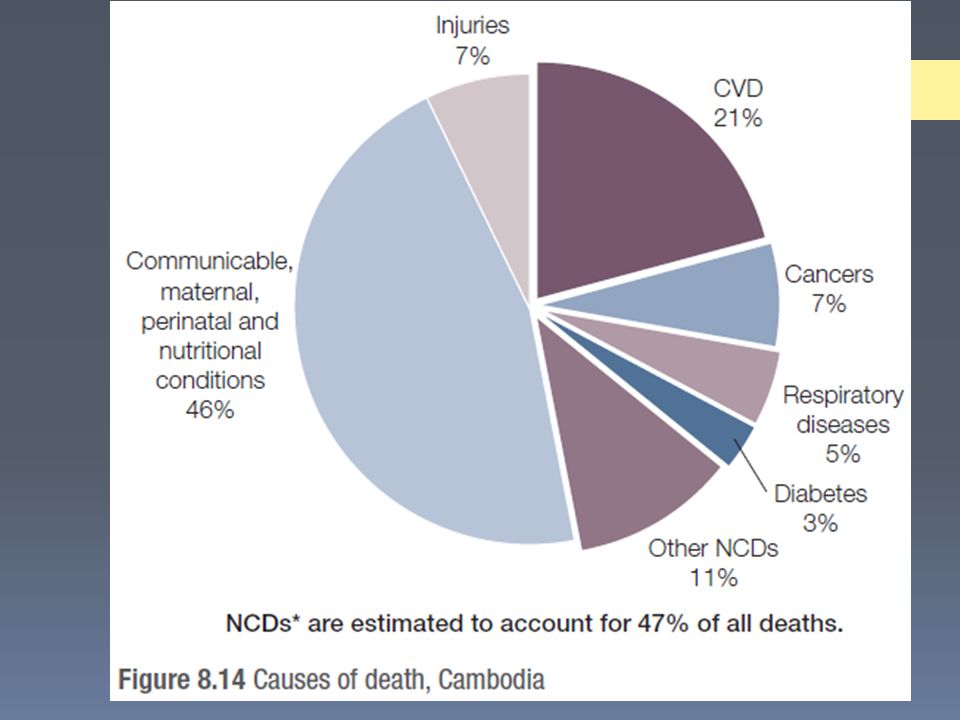
Causes of Mortality The 5 leading causes of global death are similar to Australian’s leading causes of death, however diarrhoea and HIV/AIDS are not common causes of death in Australia. Many developing countries are now also experiencing an increase in the number of deaths from non-communicable conditions, such as cancer and cardiovascular disease. What may be some reasons behind this change?

41
Causes of death-Zimbabwe

42
Causes of Mortality This narrowing in the gap between communicable and non communicable (NC) causes are due to a change in lifestyle behaviours. According to WHO, in developing countries, NC conditions such as depression and heart disease are fast replacing the traditional infectious diseases and under nutrition. Of all deaths, NC diseases were estimated to account for 35 million-double the number of communicable diseases, maternal and perinatal conditions and nutritional deficiencies combined Of the NC diseases, cardiovascular disease and cancer caused the greatest number of deaths

43
Causes of Mortality Most deaths from non-communicable diseases occur in low- and middle-income countries and tend to occur at early ages in these countries compared to high-income countries.

44
Causes of Mortality http://www.youtube.com/watch?v=p4FERTJHjD4 http://www.youtube.com/watch?v=p4FERTJHjD4

45
Causes of Mortality Once they reach adulthood, people from developing and developed countries die from some of the same causes. The main difference is the proportions of the population who are affected. In developing countries, more people die from infectious and parasitic diseases than cancer. In developed countries, only a few people die from infectious and parasitic diseases, with cancer and circulatory diseases far more common.

46
Global deaths by age and region.

47
http://www.who.int/mediacentre/factsheets/fs310/en/index1.ht ml http://www.who.int/mediacentre/factsheets/fs310/en/index1.ht ml

48
Morbidity Morbidity-refers to ill health caused by a disease or illness in an individual, or levels of ill health in a population. Morbidity is often measured in terms of prevalence and incidence. Much of the data collected on morbidity is reflected by the burden of disease.

49
Burden of disease and disability The term burden of disease refers to the impact of a particular disease in relation to healthy life lost due to ill health and disability or death experienced by a country’s population. It is measured using the Disability Adjusted Life Year or DALY One DALY = 1 lost year of healthy life due to premature death. There are significant differences in the leading causes of disease burden between countries. In the African region, HIV/ AIDS, lower respiratory infections and diarrhoeal disease are the leading causes of burden of disease. In Australia some of the leading causes of disease, injury and disability are ischaemic heart disease, stroke, depression, lung cancer, dementia, diabetes mellitus, asthma, osteoarthritis and road trauma.

50
Burden of disease and disability Developing countries: Much of the burden of disease is related to under nutrition and infectious diseases-affecting many millions of people each year. Reproductive ill health is a leading cause of disease burden for women in developing countries, much of which is avoidable with proper medical care. The devastating effects of landmines play a significant role in the death and disability of many people also Developed countries: In Australia, one of the leading causes of disability disease burden is mental illness, which comprises 30% of the total. Key knowledge: Similarities and differences in relation to burden of disease health between developing countries and Australia.

51
Burden of disease and disability In countries like Cambodia, the effects of landmines from years of war continue to be felt

52
Burden of disease and disability

53
Non-Communicable diseases Non-communicable diseases (NCDs), also known as chronic diseases- they are not passed from person to person, not contagious. There are four main types of non communicable diseases: Cardiovascular diseases (heart attacks and stroke) Cancers Chronic respiratory diseases (such as chronic obstructed pulmonary disease and asthma) Diabetes NCD’s cause of more than 36 million deaths each year and nearly 80% of these deaths occur in low- or middle income countries; CVD-causes 17 million deaths annually Cancers- causes 7.6 million deaths annually Chronic respiratory diseases- causes 4.2 million deaths Diabetes- causes 1.3 million deaths annually
 Cancers Chronic respiratory diseases (such as chronic obstructed pulmonary disease and asthma) Diabetes NCD’s cause of more than 36 million deaths each year and nearly 80% of these deaths occur in low- or middle income countries; CVD-causes 17 million deaths annually Cancers- causes 7.6 million deaths annually Chronic respiratory diseases- causes 4.2 million deaths Diabetes- causes 1.3 million deaths annually.")
54
Non-Communicable diseases NCD’s are a result of the damage caused to the body from biological risk factors (blood pressure, body weight, blood cholesterol levels, blood glucose levels, age and gender) and behavioural factors (diet, physical activity levels, tobacco use and alcohol use) or a combination of these. Many low- and middle-income countries are now facing a ‘double burden’ of disease. This means that while they continue to deal with the problems of communicable (infectious) disease and under nutrition, they are experiencing a rapid increase in non-communicable diseases (in particular obesity and HIV/AIDS.
 disease and under nutrition, they are experiencing a rapid increase in non-communicable diseases (in particular obesity and HIV/AIDS..")
55
Obesity Obesity is a major risk factor for a number of other non communicable diseases in particular diabetes, ischaemic heart disease, certain cancers Increases in the prevalence of obesity globally will impact on the leading causes of mortality and disease burden in the future Worldwide obesity has more than doubled since 1980 and, according to WHO, more than 40 million children under the age of five were overweight in 2010 and most of these live in developing countries. Overweight and obesity are the fifth leading risk for global deaths and at least 2.8 million adults die each year as a result of being overweight or obese.

56
HIV/AIDS HIV/AIDS is a serious social, economic and medical issue in many developing countries and a significant cause of mortality and morbidity. Human immunodeficiency virus (HIV) causes damage to the body’s immune system and usually results in acquired immunodeficiency syndrome (AIDS). Those at greatest risk of contracting the virus are people in developing nations who are living in poverty, as they have little access to healthcare, education or information about HIV/AIDS. HIV/AIDS has the highest infection rate among people aged 15–49 years; however, the highest rate of mortality in developing countries are among the elderly and children. Why might this be?? HIV/AIDS is one of the factors contributing to ongoing poverty in developing countries
 causes damage to the body’s immune system and usually results in acquired immunodeficiency syndrome (AIDS). Those at greatest risk of contracting the virus are people in developing nations who are living in poverty, as they have little access to healthcare, education or information about HIV/AIDS. HIV/AIDS has the highest infection rate among people aged 15–49 years; however, the highest rate of mortality in developing countries are among the elderly and children. Why might this be . HIV/AIDS is one of the factors contributing to ongoing poverty in developing countries.")
57
HIV/AIDS

58
Human Development Index (HDI) The Human Development Index is a relatively new measure, introduced by the United Nations. The HDI is used to assess the health and developmental outcomes of a nation. The HDI identifies human development as being about enlarging people’s choices, allowing them to develop their full potential and lead productive, creative lives in dignity and in accordance with their needs and interests. The HDI is not a complete measure of human development; it does, however, provide a broader view of human progress and the complex relationship between income and wellbeing. Developing countries such as Guatemala and Mozambique have a low HDI, whereas Australia ranks fourth.

59
The future in Global Health What are the significant changes being seen? What may be reasons for these changes?

60
The future in Global Health

61
As could be seen in the previous diagram much of the global burden of disease in 1990 was due to respiratory infection, diarrhoeal disease and birth complications, a large percentage of which occurred in developing countries. The WHO has predicted that by 2030, developing countries will be further exposed to the double burden of disease. (Both communicable and non-communicable diseases) Conditions such as heart disease and depression are set to have an increasing impact due to changes in lifestyle behaviours, such as diet modification and an increase in the number of people smoking and consuming alcohol in developing countries. Expected changes can also be attributed to improvements in primary healthcare, such as education, immunisation and access to safe water and sanitation
 Conditions such as heart disease and depression are set to have an increasing impact due to changes in lifestyle behaviours, such as diet modification and an increase in the number of people smoking and consuming alcohol in developing countries. Expected changes can also be attributed to improvements in primary healthcare, such as education, immunisation and access to safe water and sanitation.")
64
Millenium Development goals. Millenium Development goals. http://www.youtube.com/watch?v=75G3CRJipeA http://www.youtube.com/watch?v=75G3CRJipeA

Similar presentations








>")



 Maternity and Infancy Dr. Dina Qahwaji.>")











