Download presentation
Presentation is loading. Please wait.

1
Physiology of Lower Urinary Tract Function (including Neurogenic Bladder) Eric S. Rovner, M.D. Professor of Urology Medical University of South Carolina

2
Outline l Physiology of Micturition Micturition cycle Neurologic factors Pharmacology l Neurogenic Bladder Lesions above pons Lesions below pons above sacral SC Lesions of sacral SC and peripheral NS

3
Ideal Plumbing Requirements for a Terrestrial l Store a reasonable amount of urine at a pressure < kidney filtration pressure (25 to 40 cm H 2 O) l Rapid on-demand emptying
 l Rapid on-demand emptying")
4
l The micturition cycle: Filling/Storage Emptying Micturition Cycle: Simplified* *Wein

5
Bladder Filling and Urine Storage Requirements: l Reservoir: Accommodation of increasing volumes of urine u At a low intravesical pressure (compliance) u With appropriate sensation Absence of involuntary bladder contractions u Overactivity l Outlet: A bladder outlet that is closed at rest and remains so during increases in intra-abdominal pressure
 u With appropriate sensation Absence of involuntary bladder contractions u Overactivity l Outlet: A bladder outlet that is closed at rest and remains so during increases in intra-abdominal pressure")
6
Urine Emptying Requirements: l Reservoir: Coordinated bladder contraction of adequate magnitude (or other increase in pressure) l Outlet: Absence of anatomic obstruction Concomitant lowering of resistance at the level of: u Smooth muscle of bladder neck and proximal urethra u Striated muscle that surrounds urethra
 l Outlet: Absence of anatomic obstruction Concomitant lowering of resistance at the level of: u Smooth muscle of bladder neck and proximal urethra u Striated muscle that surrounds urethra")
7
Voiding Dysfunction* l Pathophysiology simplified All voiding dysfxn is sub-classified as abnormality of: u Filling/storage: Bladder Urethra Both u Emptying: Bladder Urethra Both Key factors: Bladder Smooth sphincter Striated sphincter Sensation *Wein

8
Voiding dysfunction l Because of urethra Too weak: u SUI (sphincteric) Too strong u BOO/retention/DESD l Because of the bladder Too weak u Detrusor underactivity (retention) Too strong u Detrusor overactivity ( OAB/UUI) l Because of both (MIXED)
 Too strong u BOO/retention/DESD l Because of the bladder Too weak u Detrusor underactivity (retention) Too strong u Detrusor overactivity ( OAB/UUI) l Because of both (MIXED)")
9
“I am not certain why humans or animals are continent of urine and feces and I am not convinced that anyone really knows.” J. Berry, 1961 (Berry Prosthesis)
.")
10
Physiology of Urinary Continence Continence = urethral closure forces > bladder expulsive forces Bladder Urethra > 1.Sphincters 2.Connective tissue 3.Urethral mucosa 1.Intravesical (IBC’s, compliance) 2.Extravesical (abdominal, etc.) = Continence
 2.Extravesical (abdominal, etc.) = Continence")
11
Micturition reflex at sacral SC: Coordination/influenced by higher centers

12
What defines neurogenic voiding dysfunction? l Abnormality in storage or voiding function of the bladder as a result of a neurologic disturbance l Must be confirmed by objective evidence of a nervous system disorder

13
Patterns of Neurogenic dysfunction l Often predicted by level of injury/disease l However, limited by Complete/Incomplete Description of sx’s is often poor (sensory loss) “….the bladder is an unreliable witness” Other co-morbidities (diabetes, CHF, etc.) Other pelvic disease (POP, SUI, BPH, etc.)
 ….the bladder is an unreliable witness Other co-morbidities (diabetes, CHF, etc.) Other pelvic disease (POP, SUI, BPH, etc.)")
14
Incidence of Bladder Dysfunction l Spinal cord injury (8k new/yr) 70%–80% l Multiple sclerosis (400k) 50%–80% l Lumbo-sacral DDD27%-92% (60-90% overall prevalence with 5% sciatica) l Radical pelvic surgery16%-20% l Parkinson’s disease15%–35% l Diabetes (17,000,000) 10%–30% l CVA (540k new/yr) 10%–15%
 70%–80% l Multiple sclerosis (400k) 50%–80% l Lumbo-sacral DDD27%-92% (60-90% overall prevalence with 5% sciatica) l Radical pelvic surgery16%-20% l Parkinson’s disease15%–35% l Diabetes (17,000,000) 10%–30% l CVA (540k new/yr) 10%–15%")
15
Central Nervous System Cortex, Basal Ganglia, Cerebellum -Frontal lobes and cingulate gyrus -Voluntary initiation of voiding -Inhibition of reflex voiding activity - Supra-pontine structures are generally inhibitory on the LUT -Injuries (CVA, etc.) release this inhibition -detrusor overactivity, and clinical sxs of urgency, frequency, incontinence
 release this inhibition -detrusor overactivity, and clinical sxs of urgency, frequency, incontinence")
16
Central Nervous System: Pons Coordination of sphincter and bladder - Afferent input (ascending and descending) -bladder wall and supra-pontine centers - Efferent outflow (descending) -sacral spine - somatic - parasympathetic centers for voiding -T-L spine -sympathetic nerves for accomodation Injuries separating Pons from LUT(SCI, MS) : reflex voiding patterns and uncoordinated voiding
 -bladder wall and supra-pontine centers - Efferent outflow (descending) -sacral spine - somatic - parasympathetic centers for voiding -T-L spine -sympathetic nerves for accomodation Injuries separating Pons from LUT(SCI, MS) : reflex voiding patterns and uncoordinated voiding")
17
Supra-sacral spinal injury/disease l Functional Abnormality Depends on u chronology, type of lesion u completeness Neurogenic Detrusor Overactivity Striated sphincter dysynergia u If above T6 (Sympathetic Outflow Tract) Smooth sphincter dysynergia Autonomic dysreflexia
 Smooth sphincter dysynergia Autonomic dysreflexia")
18
Infrasacral Injury/Disease l Clinical Presentation Urge/frequency or urinary retention +/- straining to void Usually continent l Most common urodynamic abnormality Detrusor areflexia Normal innervation of the striated sphincter Normal smooth sphincter function Irritative lesions- detrusor overactivity

19
Goals of NGB Evaluation l Accurate diagnosis characterization of voiding dysfunction (NGB) u Reassess as needed recognition of concomitant non-neurogenic VD u BPH, SUI, etc. l Assess prognosis Urological u Neurological l Direct management

20
Neurourologic Evaluation l History l Physical examination neurologic examination l PVR l Creatinine l U/A, C&S l +/- Upper tract study l +/- Urodynamic study l +/- Cystoscopy

21
Urodynamics: Utility in prognosis and treatment in NGB LUTS and PE do not correlate well with of type, extent or level of injury/disease…..or UDS findings LUTS and PE do not correlate well with prognosis or “danger” to upper tracts (but UDS does!!!!) In SCI/MS, level of injury not always predictive of UDS* u Correlation of neuro imaging and UDS not exact l Therefore management often dictated by UDS *Weld and Dmochowski, 2000
 In SCI/MS, level of injury not always predictive of UDS* u Correlation of neuro imaging and UDS not exact l Therefore management often dictated by UDS *Weld and Dmochowski, 2000")
23
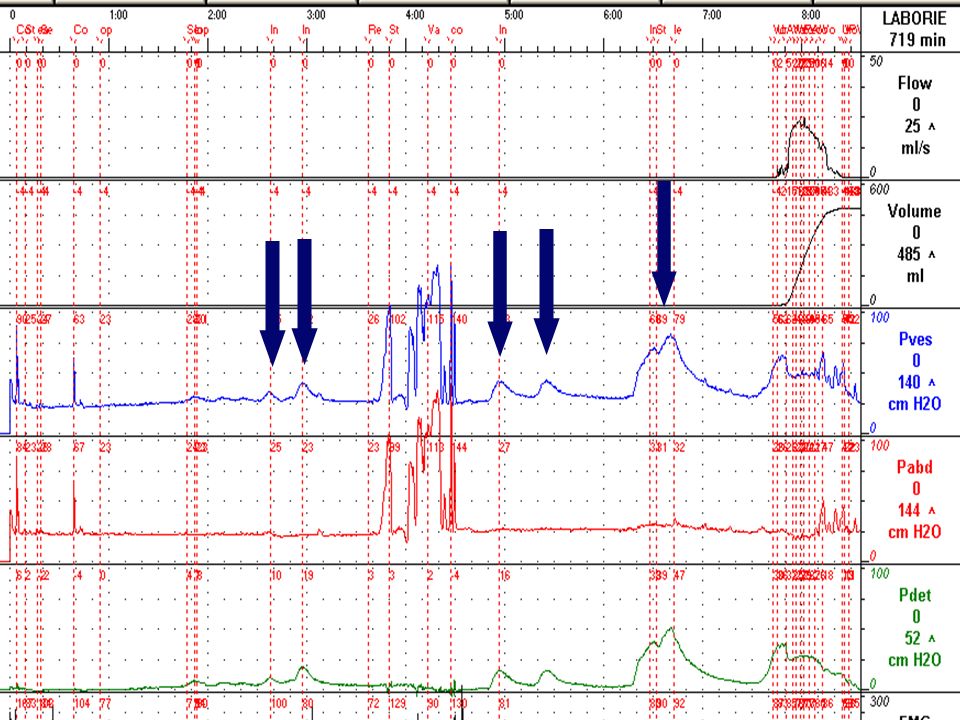
Detrusor overactivity with UI Valsalva induced DO with UI MS with sx’s of SUI with urge +/- UUI SUI

24
Q Vol pVes pAbd pdet EMG 47 y.o. with Sx’s of SUI after Rad Hyst. PVR=175cc

25
Treatment Issues in NGB l Assessing Safety 1st Upper tracts Risk factors: compliance, UTI’s, VUR, etc Other l Relieving Symptoms 2nd Incontinence Frequency, urgency Other

26
Goals of Management l Upper Tract Preservation (or improvement) l Absence or control of infection l Continence l Reduce or eliminate impact on QOL l Make an acceptable solution for the patient Physically Economically Socially Culturally
 l Absence or control of infection l Continence l Reduce or eliminate impact on QOL l Make an acceptable solution for the patient Physically Economically Socially Culturally")
27
How to achieve goals l Adequate urine storage at low pressure l Adequate emptying in absence of obstruction l Adequate urethral closure forces (competence) l Selecting least invasive/expensive Rx option. l Individual management.

28
Rx of NGB Bladder Urethra All Rx either Δ urethral or Δ bladder pressure or both

29
Lesions above the pons CVA, brain tumor, etc. Usually: Clinical presentation: 1. frequency/urgency 2. incontinence 3. usually normal upper tracts Urodynamics: 1. detrusor overactivity 2. synergic sphincters 3. normal sensation 4. normal emptying

30
Treatment: Lesions above pons l Strategy: Reduce detrusor overactivity Sphincters are OK usually l Management: Behavioral modification Antimuscarinics Sacral neuromodulation Botulinum toxin A Augmentation cystoplasty

31
Lesions between pons and sacral spinal cord MS, SCI, transverse myelitis, etc. Clinical presentation: 1. frequency/urgency (if sensation) - overactivity vs. retention 2. incontinence (+/- awareness) 3. beware upper tracts Urodynamics: 1. detrusor overactivity - sometimes underactivity 2. dyssynergic sphincters 3. +/- sensation 4. abnormal emptying
 - overactivity vs. retention 2. incontinence (+/- awareness) 3. beware upper tracts Urodynamics: 1. detrusor overactivity - sometimes underactivity 2. dyssynergic sphincters 3. +/- sensation 4. abnormal emptying.")
32
Lesions between pons and sacral spinal cord MS, SCI, transverse myelitis, etc. l Strategy: 1. reduce detrusor overactivity (if present) 2. improve emptying (when problematic) 3. reduce storage pressure 4. protect upper tracts l Management: 1. Rx detrusor overactivity (drugs, Botox, etc.) 2. +/- CIC 3. +/- urinary diversion
 2. improve emptying (when problematic) 3. reduce storage pressure 4. protect upper tracts l Management: 1. Rx detrusor overactivity (drugs, Botox, etc.) 2. +/- CIC 3. +/- urinary diversion.")
33
Autonomic Hyperreflexia (Dysreflexia)
")
34
l THIS IS AN EMERGENCY l Lesions above T6-T8 Occurs after resolution of spinal shock u Often years later Must have viable distal SC l Assoc. with DSD

35
Autonomic Hyperreflexia (Dysreflexia) Precipitating factors: Any distention of rectum or LUT LUT instrumentation (UDS) Urinary catheter issue u Tube change u Obstructed catheter clot retention, etc. Long bone fracture Decubiti GI pathology Sexual activity Other

36
AH: Treatment l Find and reverse precipitating stimulus l Acute: Parenteral ganglionic blockers α blockers Others l Prophylaxis: Do procedures under spinal or general with careful monitoring ?????? Nifedipine 10–20 mg orally 30 minutes prior; SL during Chronic α blockade (i.e. terazosin)
.")
37
Lesions distal to the spinal cord Disc disease, radical pelvic surgery, diabetes etc. Usually: Presentation: 1. frequency, urgency +/- incontinence 2. +/- urinary retention, straining 3. upper tracts at risk Urodynamics: 1. detrusor overactivity or underactivity 2. impaired compliance, +/- contractility 3. normal sensation 4. no dyssynergia

38
Lesions distal to the spinal cord Disc disease, radical pelvic surgery, etc. Strategy: 1. improve emptying (when problematic) 2. reduce storage pressure 3. protect upper tracts Management: 1. Rx poor emptying +/- CIC 2. improve compliance
 2. reduce storage pressure 3. protect upper tracts Management: 1. Rx poor emptying +/- CIC 2. improve compliance.")
39
Infrapontine lesions: Chronic Risk Factor l High intravesical storage pressure

Similar presentations