Download presentation
Presentation is loading. Please wait.

1
Domyung Paek Seoul National University World Health Organization
Asbestos in Europe Domyung Paek Seoul National University World Health Organization

2
Table 1. Early developments of the asbestos industry.
[Information from Stover Publishing Co., 1953, p. 4–6; Selikoff and Lee, 1978, p. 17–18] 1857– First packings and flat seals using asbestos. First bonded and molded asbestos product for heat insulation. 1866– Start of systematic asbestos textile processing in Italy. 1868– First U.S. use of asbestos in roofing felt and cement. Asbestos paper first made in the United States. Concept of asbestos-containing magnesia insulation developed. Asbestos textile processing began in Canada. First spinning of crocidolite in Republic of South Africa. First asbestos-containing woven brake bands made in England. Wet machine process of making asbestos cement developed. Method for manufacturing asbestos-cement panels developed. Flat asbestos-cement board manufactured in the United States. Asbestos first used as brake lining. Asbestos-containing molded clutch facing developed. Asbestos-cement pipe industry began in the United States. Technique for spraying asbestos developed in England. 1940s Asbestos-cement pipe introduced into England. Spraying asbestos on deckheads and bulkheads began in British naval ships.

5
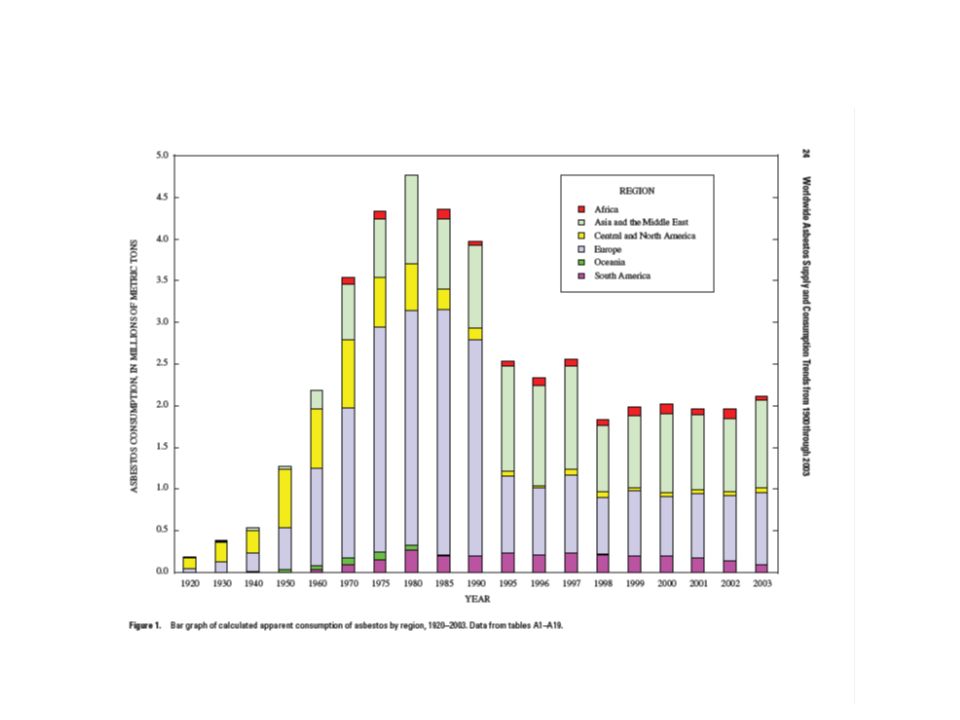
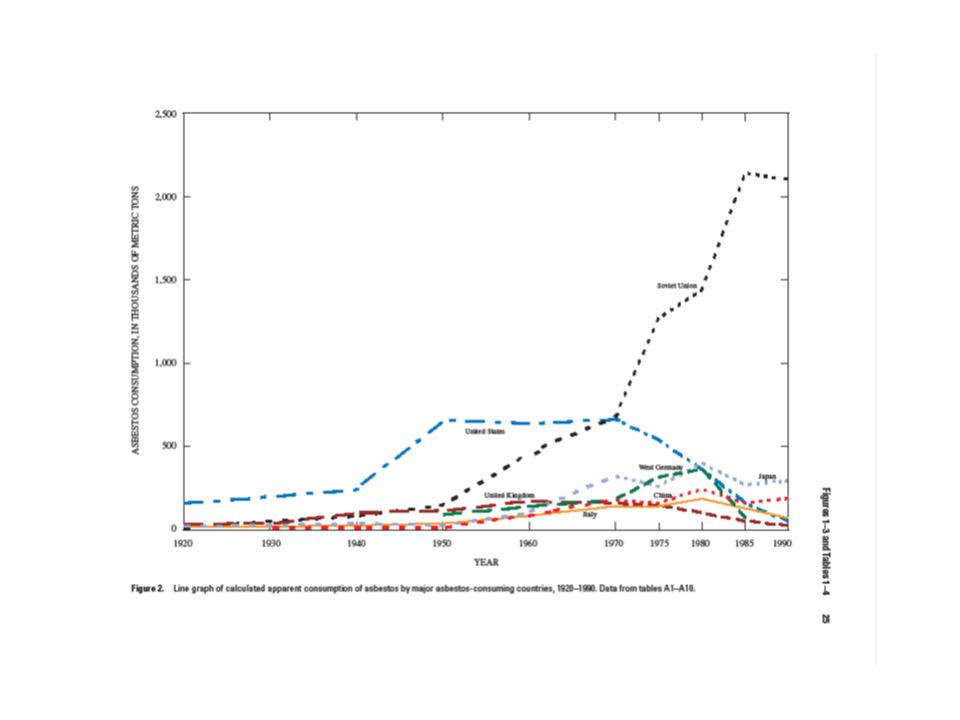
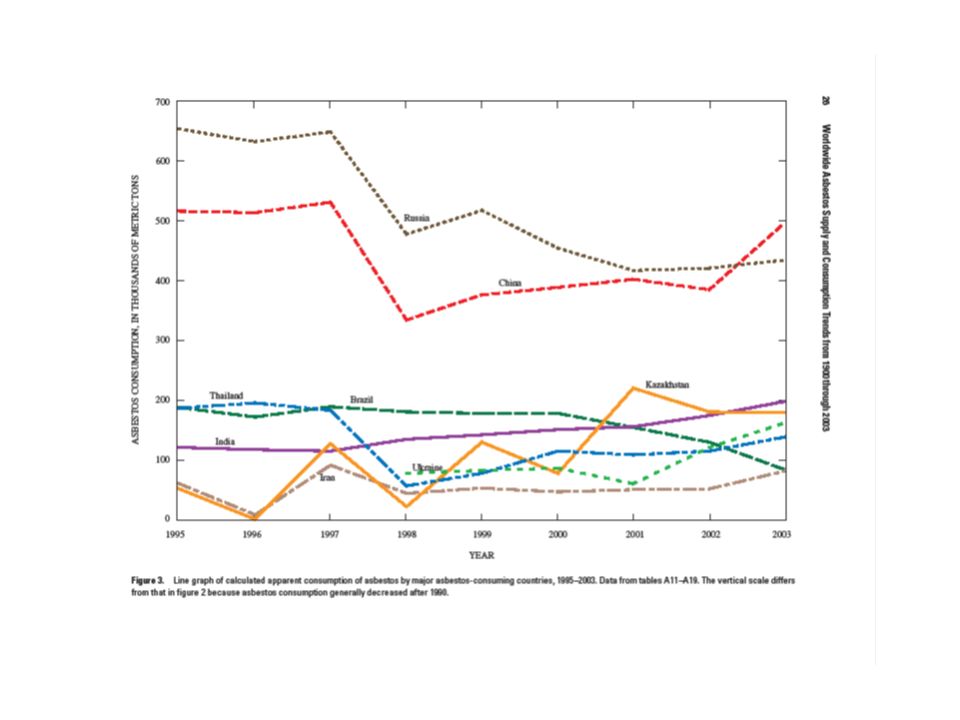
Asbestos Production & Export
Russia China Canada 335,000 Kazakhstan 180,000 Brazil ,000 Zimbabwe 130,000 Greece ,000 Swaziland ,000 India ,000 South Africa ,000 Japan ,000 Colombia ,000 United States ,000 Bulgaria ,000 Other countries 20,000 TOTAL ,130,000 (Year 2000)
")
8
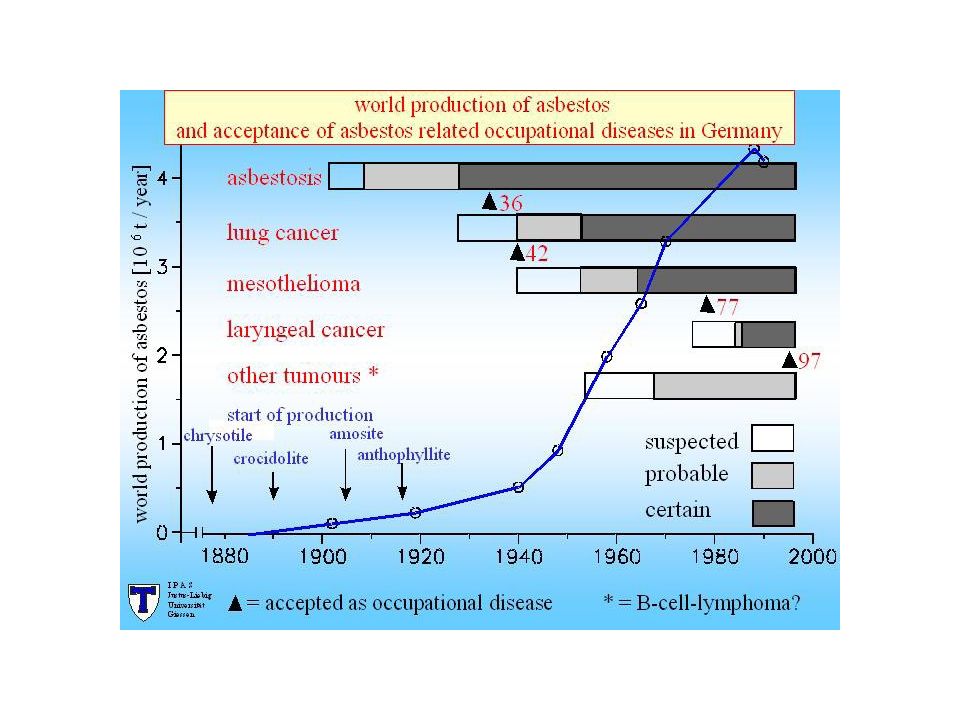
Recognition & Control of Asbestos Hazards
1924 – Asbestosis report by William Cook in BMJ (UK) 1931 – Asbestos Industry Regulation (UK) 1936 – Asbestosis Comp (Germany) 1940 – Controlling dust in Asbestos processing factories (Germany) 1942 – Lung cancer (w. asbestosis) Comp (Germany) 1955 – Lung cancer w/o asbestosis by Richard Doll who believed the risk was eliminated in 30’s and gone 1959 – Mesothelioma case report from SA 1969 – Asbestos regulation in UK (MAC) 1972 – Central registry for asbestos exposed workers (Germany) 1973 – Protection against health impairing mineral dust (Germany) 1977 – Mesothelioma Comp (Germany) 1979 – Ban on the processing of sprayed asbestos (Germany) 1993 – General Ban of Asbestos use (Germany) 1997 – Laryngeal Cancer Comp (Germany) 1999 – General Ban of Asbestos use (UK)
 1931 – Asbestos Industry Regulation (UK) 1936 – Asbestosis Comp (Germany) 1940 – Controlling dust in Asbestos processing factories (Germany) 1942 – Lung cancer (w. asbestosis) Comp (Germany) 1955 – Lung cancer w/o asbestosis by Richard Doll who believed the risk was eliminated in 30’s and gone – Mesothelioma case report from SA – Asbestos regulation in UK (MAC) 1972 – Central registry for asbestos exposed workers (Germany) 1973 – Protection against health impairing mineral dust (Germany) 1977 – Mesothelioma Comp (Germany) 1979 – Ban on the processing of sprayed asbestos (Germany) 1993 – General Ban of Asbestos use (Germany) 1997 – Laryngeal Cancer Comp (Germany) 1999 – General Ban of Asbestos use (UK)")
12
Asbestosis Comp History Exam Lung Function Chest x-ray Additional Exam
Work Smoking, alcohol Complaint (hoarseness) Exam Lung Function Chest x-ray Additional Exam Schedule 12-36/60 months 15 years after first exposure or when 45 years old ILO 1/1 profusion compensable w/o functional impairment since 1993 in Germany Respiratory Rehabilitation in outpatient clinics
 Exam. Lung Function. Chest x-ray. Additional Exam. Schedule 12-36/60 months. 15 years after first exposure or when 45 years old. ILO 1/1 profusion compensable w/o functional impairment since 1993 in Germany. Respiratory Rehabilitation in outpatient clinics.")
14
Lung Cancer Comp Same with asbestosis screening
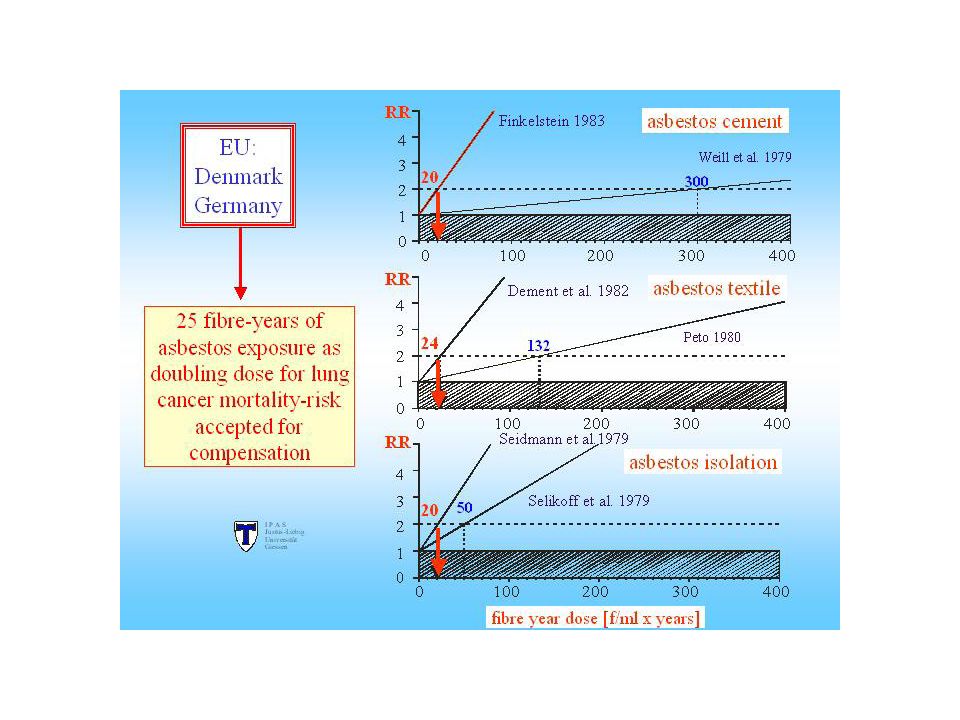
Compensable in most countries via two different pathways either in connection with asbestosis (bridging symptom) or with intense exposure (Helsinki criteria or threshold of 25 fiber/ml*year) At least 1 year in major exposure 5-10 years in moderate exposure Exposure calculated as at least 25 fiber/cc*year About of 10% of lung cancer in general population
 or with intense exposure (Helsinki criteria or threshold of 25 fiber/ml*year) At least 1 year in major exposure years in moderate exposure. Exposure calculated as at least 25 fiber/cc*year. About of 10% of lung cancer in general population.")
18
Mesothelioma Comp Same with asbestosis screening
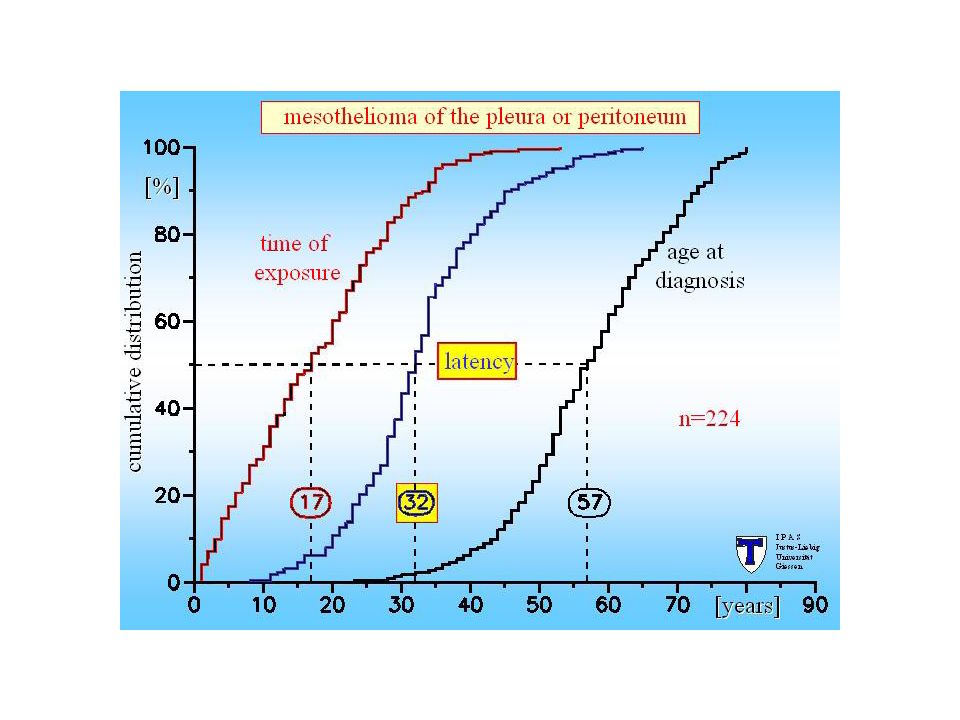
Long latency period and registration needs Without sign of disease With occupational disease such as asbestosis or pleural lesions Hard to diagnose because of pathologic variety, and some countries have mesothelioma panels Almost exclusively due to asbestos, and in all the Europe, even modest exposure (a few weeks) to asbestos dust is sufficient for recognition
 to asbestos dust is sufficient for recognition.")
23
Ecological association between asbestos-related diseases and historical asbestos consumption: an international analysis Ro-Ting Lin, Ken Takahashi, Antti Karjalainen, Tsutomu Hoshuyama, Donald Wilson, Takashi Kameda, Chang-Chuan Chan, Chi-Pang Wen, Sugio Furuya, Toshiaki Higashi, Lung-Chang Chien, Megu Ohtaki Lancet 2007; 369: 844–49

24
Laryngeal Cancer Comp 1997, Germany based on increased risk even after controlling other factors Not yet universal CORRESPONDENCE Does Asbestos cause laryngeal cancer? Dr Maher El Alami Queens Medical Centre, Nottingham, UK Clin. Otolaryngol. 2004, 29, 285

25
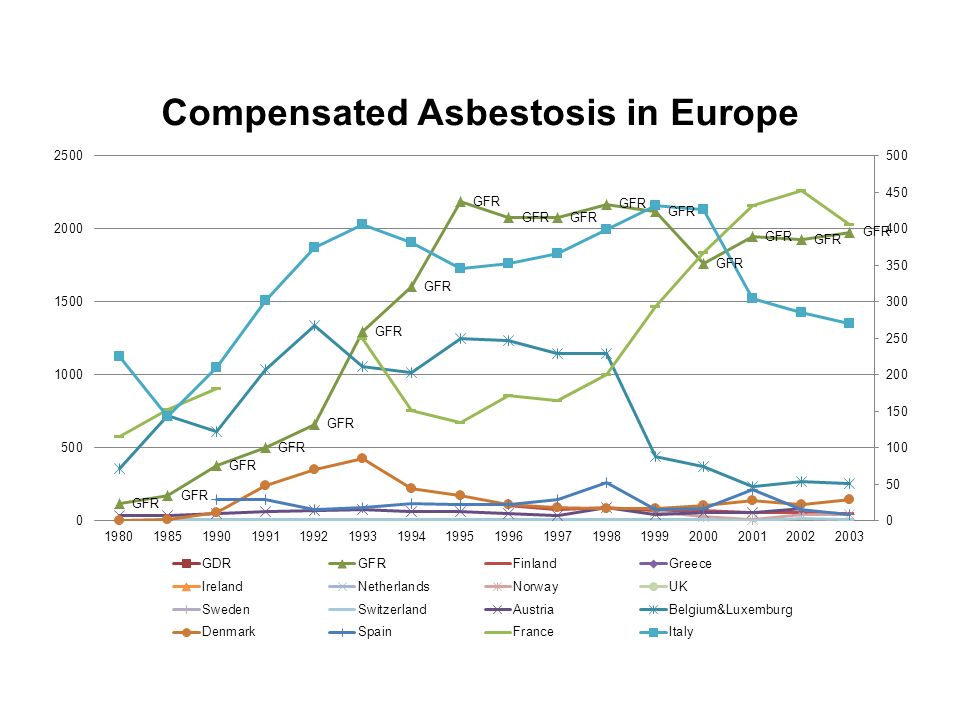
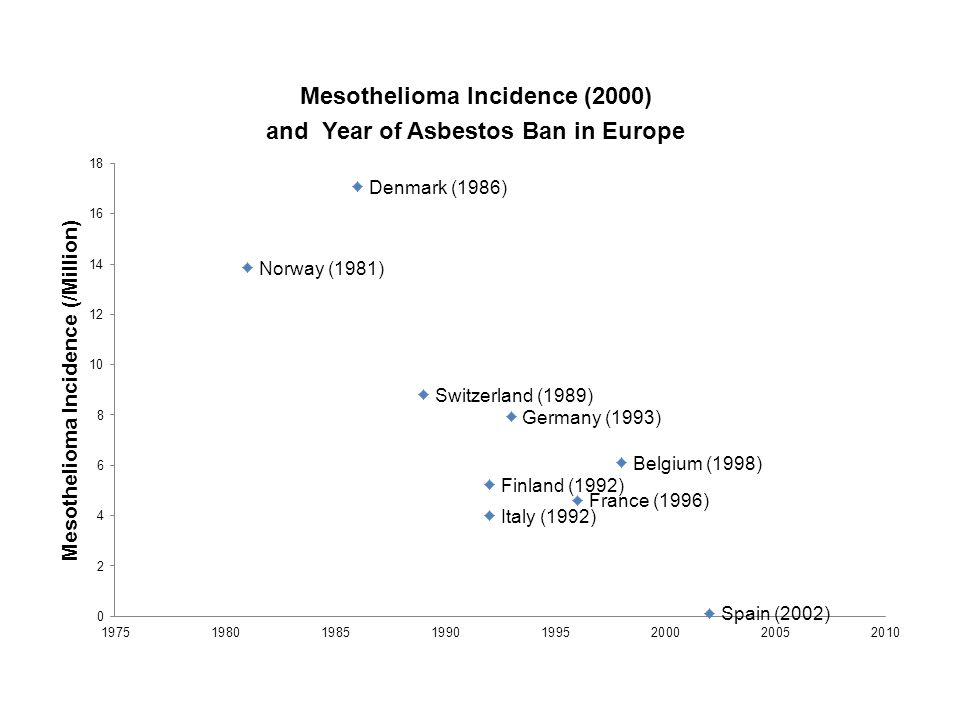
Year of Ban Country Mesothelioma Incidence 1981 Norway 13.8 1986 Denmark 17.1 Sweden 1989 Switzerland 8.8 1990 Austria 1991 Netherlands 1992 Finland 5.2 Italy 4.0 1993 Germany 7.9 1996 France 4.6 1998 Belgium 6.1 1999 UK 2000 Ireland 2002 Spain 0.1 2005 Greece

27
Post-hoc comments 30’-60’: asbestos risk believed to be controllable
Technical professionals’ approach (medical inspectors and hygienist) Most dangerous risks including cancer was thought to be eliminated in 30’s by regulation, only appear due to the long latency Still setting TLV based on asbestosis risk not cancer risk 60’-70’: hazards beyond the heavily exposed during production First extended to the end-users Then community risks reported and media attention brought Calling for ban and industry propaganda
 Most dangerous risks including cancer was thought to be eliminated in 30’s by regulation, only appear due to the long latency. Still setting TLV based on asbestosis risk not cancer risk. 60’-70’: hazards beyond the heavily exposed during production. First extended to the end-users. Then community risks reported and media attention brought. Calling for ban and industry propaganda.")
30
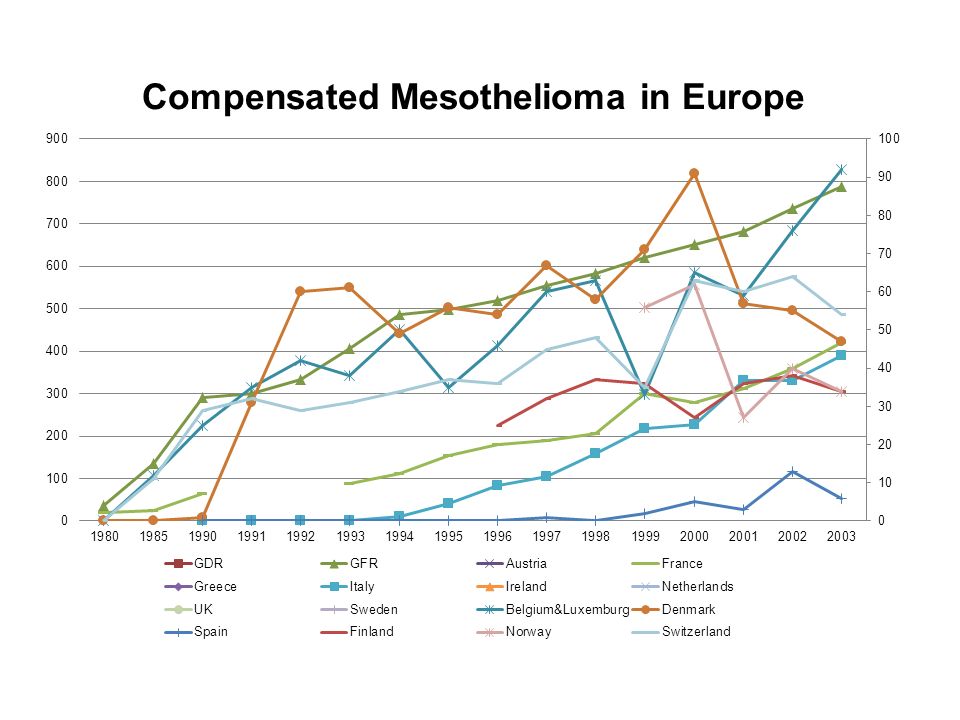
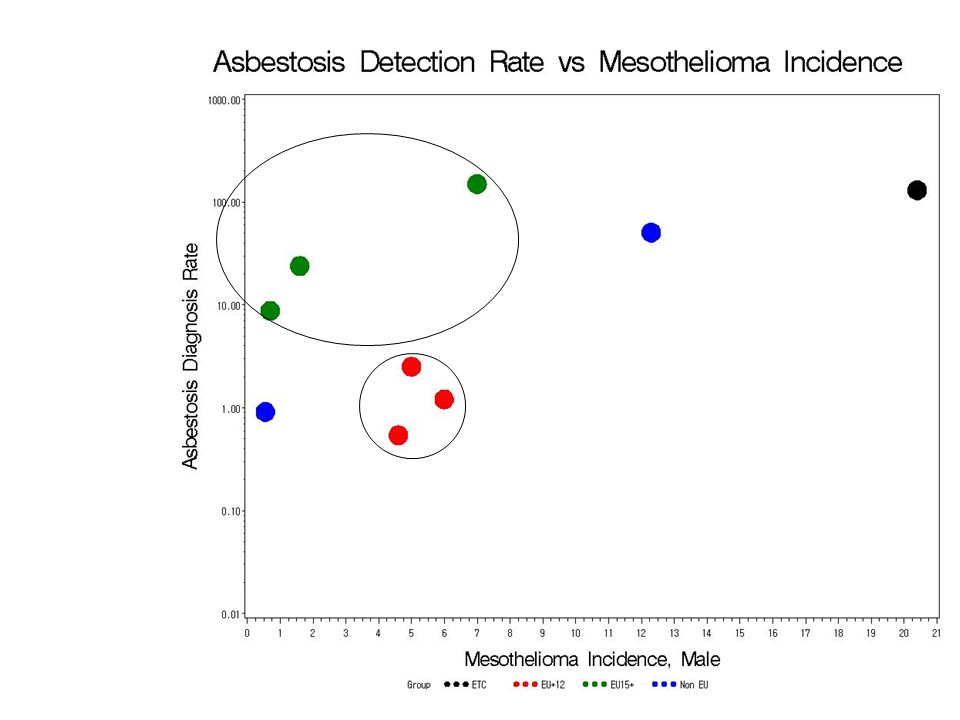
Asbestos and Mesothelioma in Europe
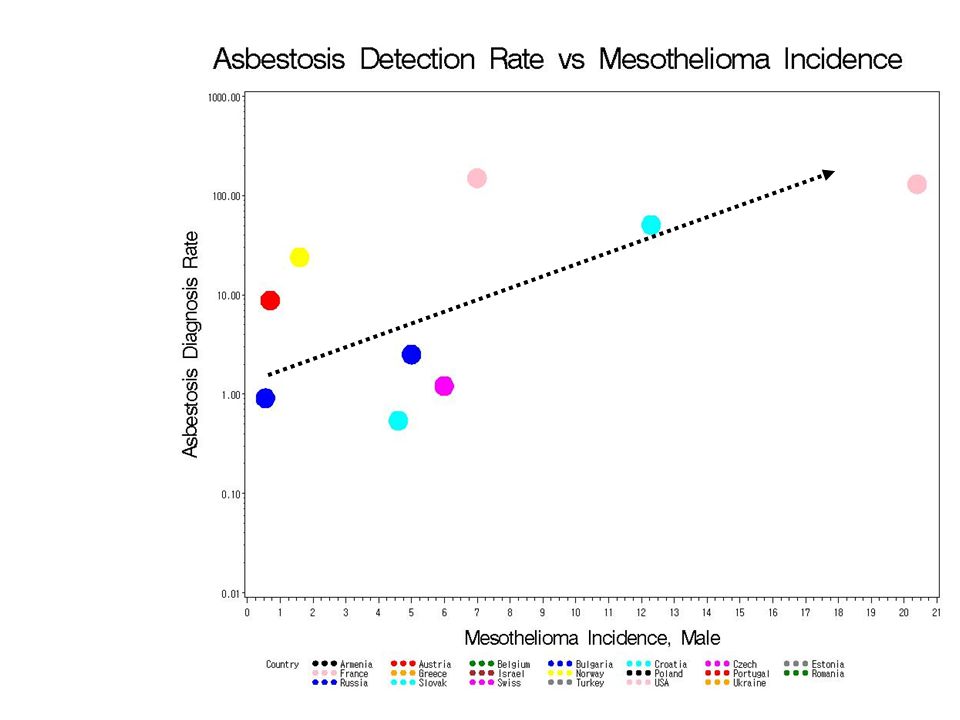
Mesothelioma incidence ↑ → Asbestosis detection rate ↑↑ EU15+ countries tend to have more asbestosis cases detected while with lower incidences of mesothelioma than EU+12 countries

31
Analysis of National H&S Program
Focus on Input-Output-Outcome linkage → Exp Assmnt, Dis Assmnt, and H&S Solution versus

32
Discussions (1) The H&S problem solving cycle is
not Exp Ass → Exp Reduction → Dis Reduction, but Exp Ass → Dis Detection → Exp Reduction. Here the core ideas of problem solving strategy should lie with how to link exposure assessment with disease detection, and also how to link disease detection to source control. Many countries still show high exposure assessment coverage with no or minimal disease detections, and high disease detection rate with no source controls.

33
Discussions (2) Differences in H&S among Euro member countries could be identified as expected from membership history. Problems of H&S usually drive the program as in the case of high mesothelioma incidence that leads to even higher detection of asbestosis, but country differences could be identified. Comparatively higher problems should be stressed and concerns be raised for each country until the lowest possible examples can be obtained. We need collective and comparative social issue making.

34
Discussions (3) Scope of the H&S program is important in that the coverage determines the detection rate of NIHL and pneumoconiosis, and for accidents, it determines the over-all accident rates of the society. Target priority may be important, but general universal acknowledgement of H&S values by the society is more fundamental to the effectiveness of the program. Risk population is at risk, not because of high risk works, but because of acceptance of high risks for that particular working population. Minority populations including non-standard workers and illegal migrant workers should be given particular considerations in this issue of the H&S program scopes.

Similar presentations