Download presentation
Presentation is loading. Please wait.

1
Authors: Col. Assoc.Prof. Jiri Pasta, MD, PhD. Katerina Buusova Smeckova, MD, MBA Jaroslav Madunicky, MD Eva Vyplasilova, MD Department of Ophthalmology of the First Faculty of Medicine of Charles University and Central Military Hospital, Prague None of the authors has a financial interest on the presented data.

2
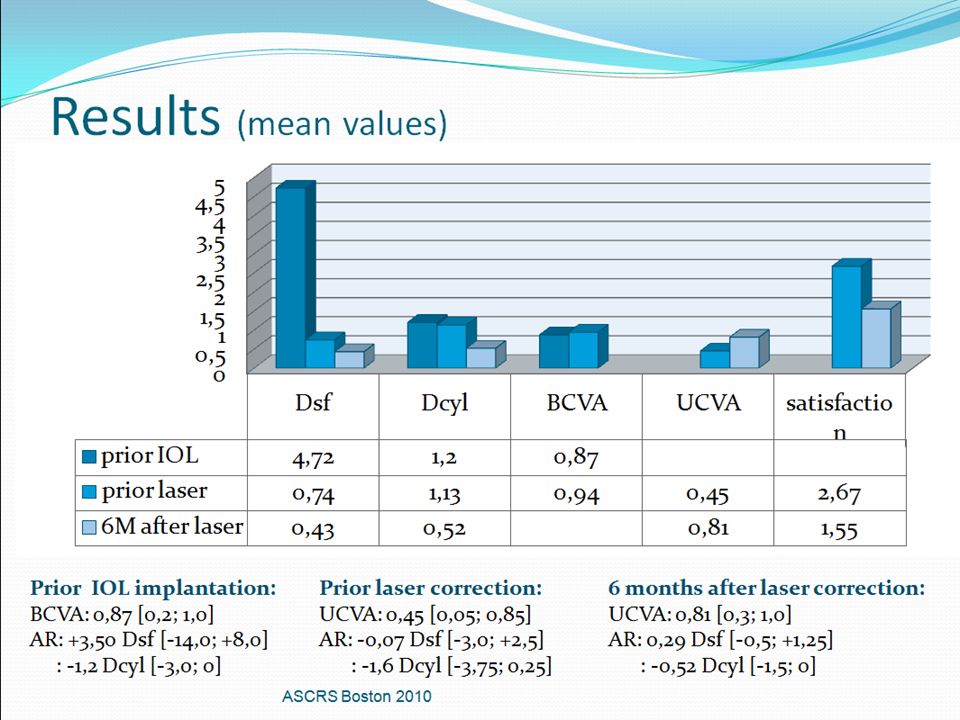
Purpose Retrospective study of 17 patients (25 eyes) who under came premium IOL implantation since 2007 and consequently a laser correction (PRK) of the residual refractive error (cylindrical and spherical). Change in the refractive error (Dsf and Dcyl) and uncorrected visual acuity was compared with the results of the patient satisfaction survey. ASCRS Boston 2010
 and uncorrected visual acuity was compared with the results of the patient satisfaction survey. ASCRS Boston")
3
Setting / Venue 17 patients (10 women, 7 men) Mean age: 46 let [23 ; 62 ] Mean Dsf preop: hyperopes: +4,46 Dsf [+1,5; +8,0] myopes: -7,88 [-14,0; -1,75] Mean Dcyl: -1,2 Dcyl [-3,0;0] preop Mean BCVA preop: 0,87 [0,2; 1,0] Mean AR: +4,25 Dsf [-13,5 ;+9,75] -1,21 Dcyl [-3,25;+3,5] 6 patients with light amblyopia, 1 patient with the senile cataract, 1 patient with the traumatic cataract All laser corrections were performed on VISX STAR S4 IR. ASCRS Boston 2010
![Setting / Venue 17 patients (10 women, 7 men) Mean age: 46 let [23 ; 62 ] Mean Dsf preop: hyperopes: +4,46 Dsf [+1,5; +8,0] myopes: -7,88 [-14,0; -1,75] Mean Dcyl: -1,2 Dcyl [-3,0;0] preop Mean BCVA preop: 0,87 [0,2; 1,0] Mean AR: +4,25 Dsf [-13,5 ;+9,75] -1,21 Dcyl [-3,25;+3,5] 6 patients with light amblyopia, 1 patient with the senile cataract, 1 patient with the traumatic cataract All laser corrections were performed on VISX STAR S4 IR.](http://images.slideplayer.com/25/8014989/slides/slide_3.jpg "ASCRS Boston")
4
Methods: Prior the premium IOL implantation and laser treatment BCVA and autorefractometry measurements were performed. Both anterior and posterior segment were evaluated. Standard cataract / RLE surgery was performed-Infinity phaco, incision 2,2mm, one surgeon, in the case of the higher astigmatism incision in the K max, no relaxation incisions. Patients were treated with VISX Star S4 IR and PRK method. Uncorrected visual acuity and autorefractometry measurements were performed 1, 3 and 6 months postoperatively. Satisfaction was evaluated with a questionnaire. Patients were asked about their vision, night vision problems, overall satisfaction, eye dryness problems, if they would undertake the procedure once again and if they would recommend it to their friend. Patients were asked to list advantages and disadvantages of the procedure. ASCRS Boston 2010

6
Patient satisfaction survey I. Has your vision improved after the laser enhancement? Do you need to wear glasses after the laser enhancement? ASCRS Boston 2010

7
Patient satisfaction survey II. Do you have problems with dry eye? After the IOL implantation After the laser enhancement ASCRS Boston 2010

9
Patient satisfaction survey IV. How would you evaluate your overall vision? How would you evaluate your night vision? 2,7 after IOL 1,5 after bioptics 2,4 after IOL 1,8 after bioptics ASCRS Boston 2010 1=the best5=the worst

10
Patient satisfaction survey V. What kind of advantages and disadvantages did the laser enhancement brought to you? Advantages Disadvantages No need for glasses Headache reduction Freedom in sport activities Pain, unpleasant feelings Prolonged recovery, as well as ability to return completely to working process Dry eye syndrome Delayed ability to focus, longer reaction time Additional costs ASCRS Boston 2010

11
Comparison of possible astigmatism correction means ASCRS Boston 2010

12
Conclusion BIOPTICS seems to be safe and undepreciated alternative to the other astigmatic correction means (glasses, toric contact lenses, astigmatic keratotomy and the toric IOL implantation). Patient satisfaction is high. Final vision quality is influenced by the preoperative functional properties of the eye. ASCRS Boston 2010

Similar presentations







 for Keratoconus (KC) with Simultaneous Collagen Cross-linking (CXL) Using High-Resolution Excimer.>")











