Download presentation
Presentation is loading. Please wait.

1
MEDICAL PARASITOLOGY & ENTOMOLOGY LECTURER: SR. NORAZSIDA RAMLI

2
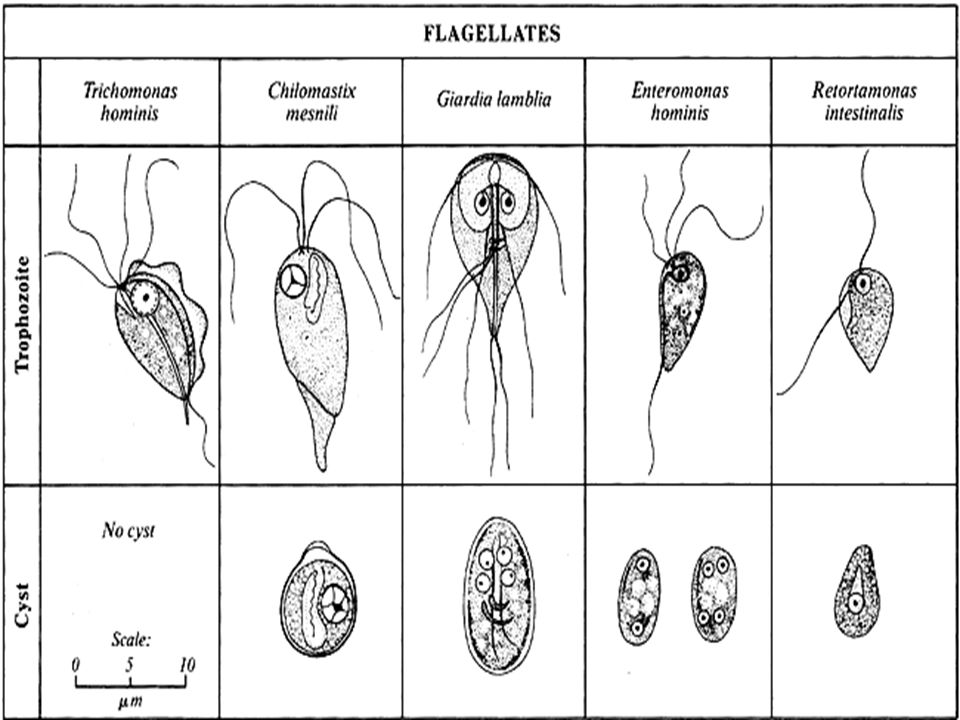
INTESTINAL FLAGELLATES Giardia lamblia (pathogenic) Chilomastix mesnili (non-pathogenic) Enteromonas hominis (non-pathogenic) Retortamonas intestinalis (non-pathogenic) Trichomonas hominis (non-pathogenic) Dientamoeba fragilis (non-pathogenic)
 Chilomastix mesnili (non-pathogenic) Enteromonas hominis (non-pathogenic) Retortamonas intestinalis (non-pathogenic) Trichomonas hominis (non-pathogenic) Dientamoeba fragilis (non-pathogenic)")
4
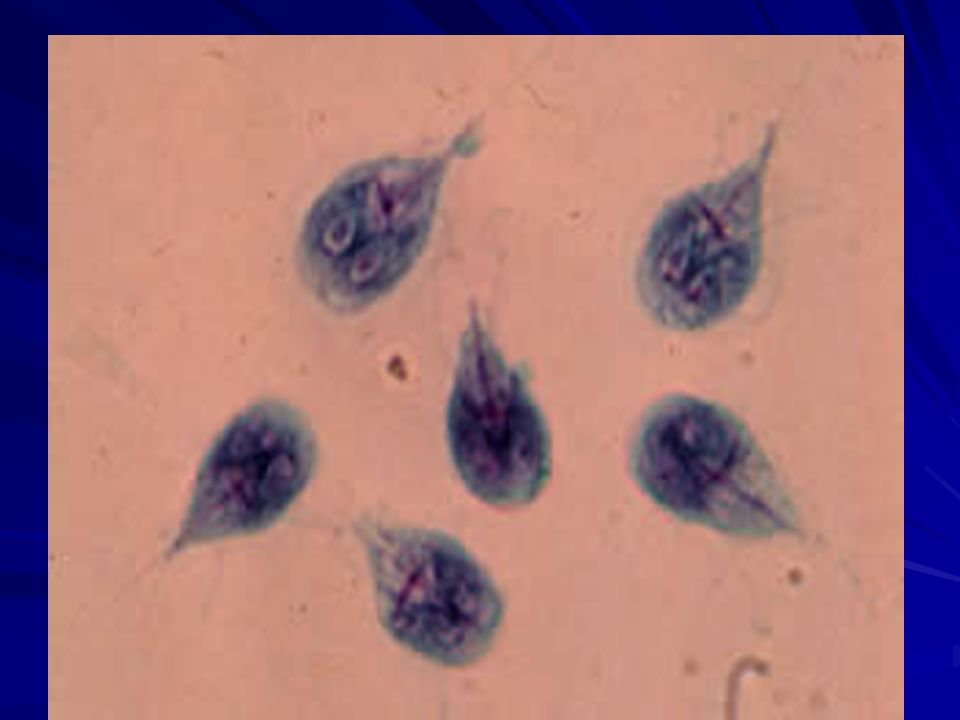
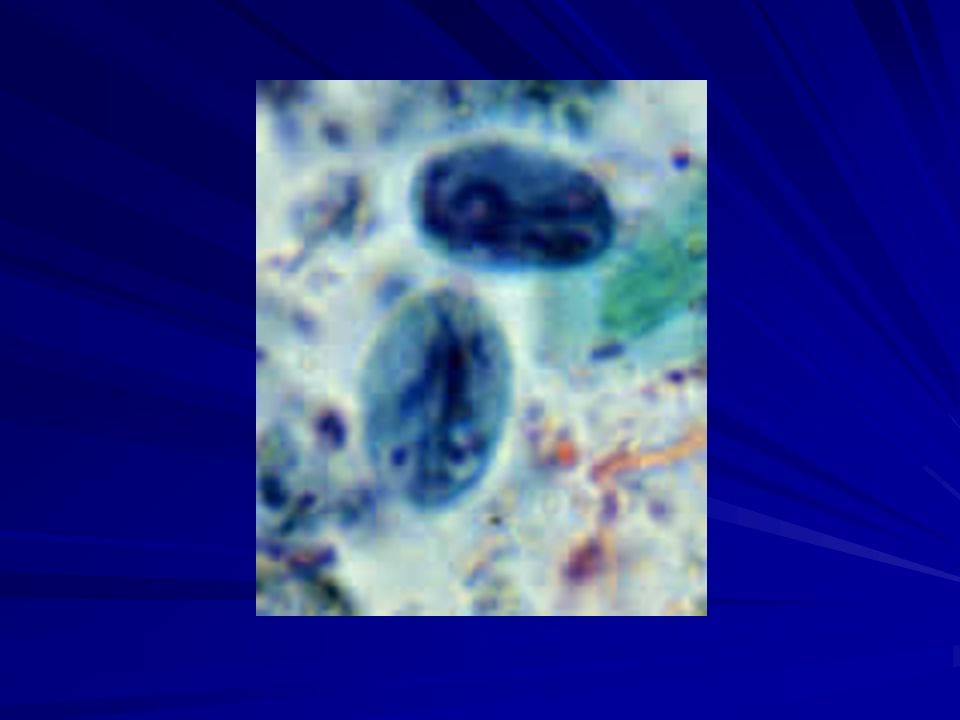
Giardia lamblia Also known as G. intestinalis or G. duodenalis. Diseases: Giardiasis, lambliasis, flagellate diarrhea. Geographic distribution: world wide, more prevalence in warm climates. Consist of 2 stages: 1)trophozoite 2)cyst Trophozoite: 9-20µm in length, 5-15µm in width, oval to pear shaped, 2 nucleus, Cyst: 8-18µm in length, 7-10µm in width, oval, more eccentric karyosome, 4 median bodies (mature cyst), 4 nucleus (mature cyst).
trophozoite 2)cyst Trophozoite: 9-20µm in length, 5-15µm in width, oval to pear shaped, 2 nucleus, Cyst: 8-18µm in length, 7-10µm in width, oval, more eccentric karyosome, 4 median bodies (mature cyst), 4 nucleus (mature cyst)..")
5
G. Lamblia (trophozoite) K= karyosome Nu=nucleus MB=median body Fg=flagellaAx=axoneme AD=adhesive disk
 K= karyosome Nu=nucleus MB=median body Fg=flagellaAx=axoneme AD=adhesive disk.")
8
G. Lamblia (cyst) Nu=nucluesK=karyosomeAx=axoneme MB=median body CW=cyst wall
 Nu=nucluesK=karyosomeAx=axoneme MB=median body CW=cyst wall")
12
Life Cycle

13
Infective stage: cyst Acquired by ingestion passage through stomach small intestine duodenum large intestine pass in stool environment. Duodenum= excystation occurs trophozoite multiply itself by longitudinal binary fission (approximately 8 hours intervals). Large intestine= encystation occurs. Both trophozoite and cyst can be found in the feces.
. Large intestine= encystation occurs. Both trophozoite and cyst can be found in the feces..")
14
Transmission & Pathogenesis The most pathogenic intestinal flagellate. Distribution: world wide Found in the gastrointestinal tracts of a variety of mammals, including man. Habitat: ponds, lakes, stream. Resistant to chlorine. Filtration is necessary to eliminate contamination.

15
Transmitted via: water, foods (fruits and raw vegetables), person to person contact (oral-anal sexual practices). Incubation period bout 2-3 weeks get symptoms: watery foul-smelling diarrhea, abdominal cramps, flatulence, anorexia, and nausea. Also have fat-soluble deficiencies, folic acid deficiencies, hypoproteinemia with hypogammaglobulinemia and structural changes in intestinal villi.

16
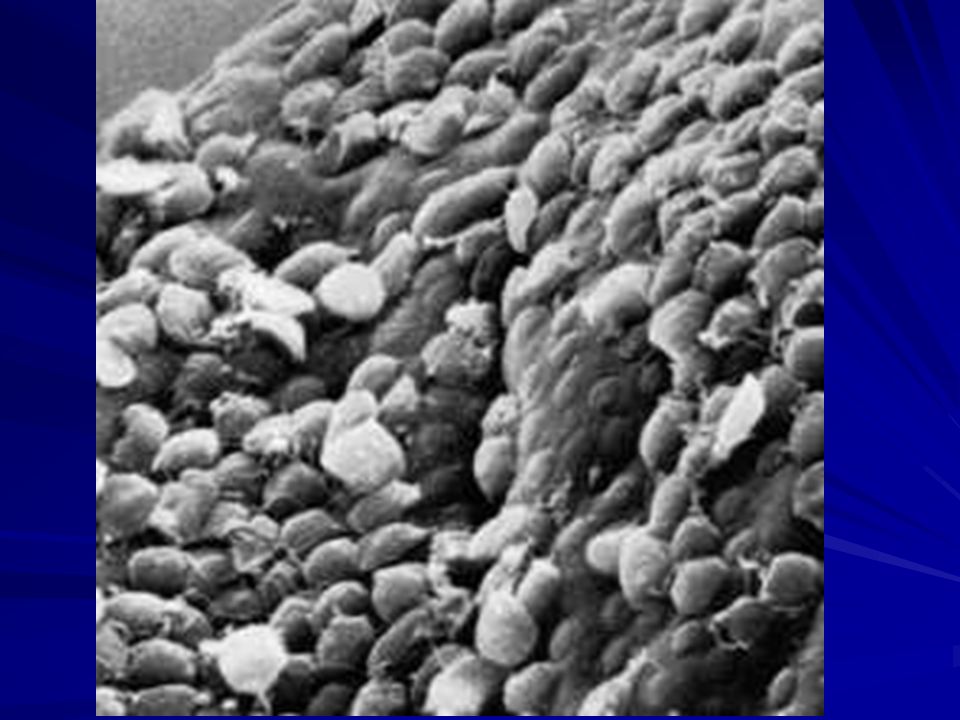
Severe cases: get malabsorption syndrome and steatorrhea, and weight loss. Patient r often, however asymptomatic. How d parasite attaches to the intestinal mucosa? By the sucking disc/adhesive disc located on the ventral side of the cell.

18
Severe cases Attachment of trophozoites to the brush border could produce a mechanical irritation or mucosal injury. In addition, normal villus structure is affected in some patients. For example, villus blunting (atrophy) and crypt cell hypertrophy and an increase in crypt depth have been observed to varying degrees. The increase in crypt cells will lead to a repopulation of the intestinal epithelium by relatively immature enterocytes with reduced absorptive capacities. An increased inflammatory cell infiltration in the lamina propria has also been observed and this inflammation may be associated with the pathology. Giardia infection can also lead to lactase deficiency as well as other enzyme deficiencies in the microvilli. This reduced digestion and absorption of solutes may lead to an osmotic diarrhea and could also explain the malabsorption syndromes. Thus far, no single virulence factor or unifying mechanism explains the pathogenesis of giardiasis
 and crypt cell hypertrophy and an increase in crypt depth have been observed to varying degrees. The increase in crypt cells will lead to a repopulation of the intestinal epithelium by relatively immature enterocytes with reduced absorptive capacities. An increased inflammatory cell infiltration in the lamina propria has also been observed and this inflammation may be associated with the pathology. Giardia infection can also lead to lactase deficiency as well as other enzyme deficiencies in the microvilli. This reduced digestion and absorption of solutes may lead to an osmotic diarrhea and could also explain the malabsorption syndromes. Thus far, no single virulence factor or unifying mechanism explains the pathogenesis of giardiasis.")
19
Laboratory diagnosis -Differentiation is based on morphological examination of fecal preparations. Microscopic examination Serological assays Immunofluoresence methods Enzyme immunoassays

20
Treatment MetronidazoleQuinacrineTinidazoleFurazolidoneParomomycin

21
Prevention By avoidance of contaminated water. Filtration (this parasite resistant to chemicals such as chlorine). Protecting water supplies from reservoir hosts such as beavers, muskrats and voles. Exercising good personal hygiene. Safe sexual practices.
. Protecting water supplies from reservoir hosts such as beavers, muskrats and voles. Exercising good personal hygiene. Safe sexual practices..")
22
UROGENITAL FLAGELLATES

23
Trichomonas vaginalis Caused a sexually transmitted disease. Have only trophozoite stage. Trophozoite: 8-23µm in length, 5-12µm in width, rounded anterior end, tapered posterior end, 4-6 flagella (originate from the anterior end), undulating membrane shorter than T. hominis, usually with visible axostyle, granules near the axostyle, chromatin is evenly distributed, single nucleus. In wet preps exhibit a rapid, jerky motion.
, undulating membrane shorter than T. hominis, usually with visible axostyle, granules near the axostyle, chromatin is evenly distributed, single nucleus. In wet preps exhibit a rapid, jerky motion..")
24
T. Vaginalis trophozoite Fg=flagella Bb=basal body Nu=nucleusAx=axostyle um=undulating membrane Cy=cytostomal groove Cs=costa

26
(A) T. vaginalis parasite as seen in broth culture. The axostyle, undulating membrane, and flagella are clearly visible. 5 μm

27
(B) T. vaginalis on the surface of a vaginal epithelial cell prior to ameboid transformation. 5 μm
 T. vaginalis on the surface of a vaginal epithelial cell prior to ameboid transformation. 5 μm")
28
(C) Ameboid morphology of T. vaginalis as seen in cell culture. 5 μm
 Ameboid morphology of T. vaginalis as seen in cell culture. 5 μm")
29
Life cycle

30
LIFE CYCLE Women: Reside on the mucous membranes of the vagina. Feed on bacteria and white blood cells. Men: reside in the prostate gland or the urethral epithelium. Multiplication occurs by longitudinal binary fission.

31
Transmission/pathogenesis Transmitted by sexual contact. Infected person may be asymptomatic or, Women: burning, itching, irritation and produce o profuse foul-smelling, yellowish discharge, and also red lesions on the vaginal mucosa. Men: urethritis, severe cases prostate tenderness and swelling,

32
LABORATORY DIAGNOSIS Clinical Presentation Microscopic and Culture Techniques Antibody-Based Techniques DNA Techniques-PCR

33
Treatment Metronidazole, oral antibiotics for both partners. To avoid re-infection, any sexual partners must also be treated. Once successfully treated, T. vaginalis doesn't come back unless a new infection is acquired.

34
Prevention Avoidance of unprotected sex.

35
CASE STUDY A 24-year old hiker had recently returned from a camping trip to Colorado. While camping, she had obtained drinking water from an untreated stream. Several weeks after returning home, she presented to her family physician with profuse, watery diarrhea, cramphy abdominal pain, and foul-smelling flatulence. Stool specimens were negative for enteric bacterial pathogen, but wet mounts demonstrated binucleate pear-shaped trophozoites showing a “falling leaf” type of motility. A permanent trichrome stain confirmed the diagnosis.

36
Questions 1) What is the name of parasite causing the patient’s illness? What is the infectious stage of this parasite? 2) How does this parasite sometimes result in malabsorption? 3) How does this parasite avoid being dislodged by intestinal peristalsis? 4) How is this parasite transmitted? How can transmission be prevented? 5) How is this illness treated?
 How does this parasite sometimes result in malabsorption. 3) How does this parasite avoid being dislodged by intestinal peristalsis. 4) How is this parasite transmitted. How can transmission be prevented. 5) How is this illness treated .")
Similar presentations





 –Giardiasis. –Most distinctive of the flagellates. –Has both a trophozoite and cyst stage.>")










 Giardia lamblia ( 蓝氏贾第鞭毛虫 ) Intestinal flagellate Giardia lambilia lives in small intestine Giardiasis Diarrhea “traveler’s diarrhea”>")






