Download presentation
Presentation is loading. Please wait.

2
Management Of AMI Does time matter?? What is the best strategy: PPCI Vs TT

3
Advise & Guidance & Lessons from NERMI and other MI Registries, Raouf Mahran,Prof.NHI.Imbaba.MRCP,DCM,DGM,LRCPS

5
Optimizing reperfusion Rapid delivery of reperfusion therapy is essential whether PPCI or thrombolytics Each of these reperfusion methods has its merits and shortcomings. The ideal reperfusion strategy would deliver rapid, complete and sustained reperfusion with normalization of micro- vascular flow.

6
Importance of Early Reperfusion Therapy in STEMI Outcomes Dependent Upon: Time to treatment-TIME IS STILL MUSCLE Early and full restoration in coronary blood flow Sustained restoration of flow

7
Prehospital Issues EMS –Emphasis on early defibrillation; AEDs; 911 dispatchers training & use of national protocols Chest Pain Evaluation & Treatment –Emphasis on giving chewable ASA, unless contraindicated & prehospital ECG & checklist Prehospital Fibrinolysis –Upgraded to a Class IIa (Level B) Recommendation Prehospital Destination Protocols –Where to transport STEMI patients-Have a plan in place –Special considerations Cardiogenic ShockCardiogenic Shock Fibrinolytic contraindicatedFibrinolytic contraindicated Antman et al. JACC 2004;44:675-7.

8
Achieve Coronary Patency Initial Reperfusion Therapy –Defined as the initial strategy employed to restore blood flow to the occluded coronary artery 4 Major Options: Pharmacological ReperfusionPharmacological Reperfusion PCIPCI Acute Surgical ReperfusionAcute Surgical Reperfusion Facilitated PCIFacilitated PCI Antman et al. JACC 2004;44:680.

9
Trials/Consensus??? PPCI Vs TT Which is best for our patients?

10
Limitations of current reperfusion therapy Thrombolytics Drug failure (30%) Re-infarction Bleeding Primary PCI Inevitable delay Availability Operator dependent Should we combine therapies?
 Re-infarction Bleeding Primary PCI Inevitable delay Availability Operator dependent Should we combine therapies")
11
Primary PCI vs Thrombolysis in STEMI: Meta-analysis (23 RCTs, N=7739) Adapted with permission from Keeley EC, et al. Lancet. 2003;361:13-20. PCI Thrombolytic therapy 0 5 10 25 15 20 Frequency (%) Short-term Outcomes (4-6 weeks) Death P =.0002 NonfatalMI P <.0001 RecurrentIschemia Hemor-rhagicStroke MajorBleed P =.032 Death, Nonfatal Reinfarction, or Stroke P <.0001 Bonferroni correction 6 variables: p <0.0083
 Short-term Outcomes (4-6 weeks) Death P =.0002 NonfatalMI P <.0001 RecurrentIschemia Hemor-rhagicStroke MajorBleed P =.032 Death, Nonfatal Reinfarction, or Stroke P <.0001 Bonferroni correction 6 variables: p <")
14
Analysis:Of 6763 pts,3383 randomised to FL,and 3380 to PCI. Median presentation time delay,was not different.140 m,in PCI& 143m for FL.11%. Result: 1)PCI was associated with: 37% reduction in 30 days mortality. 2)Reinfarction occurred in 6.7 % of FL pts, and in only 2.4% of PCI patients. **European heart journal(2006)27,779-788.Author:Eric Boersma,et al.Analysis:Of 6763 pts,3383 randomised to FL,and 3380 to PCI. Median presentation time delay,was not different.140 m,in PCI& 143m for FL.11%. Result: 1)PCI was associated with: 37% reduction in 30 days mortality. 2)Reinfarction occurred in 6.7 % of FL pts, and in only 2.4% of PCI patients. **European heart journal(2006)27,779-788.Author:Eric Boersma,et al. PPCI versus in-hospital fibrinolysis(FL), in AMI.
PCI was associated with: 37% reduction in 30 days mortality. 2)Reinfarction occurred in 6.7 % of FL pts, and in only 2.4% of PCI patients. **European heart journal(2006)27, Author:Eric Boersma,et al.Analysis:Of 6763 pts,3383 randomised to FL,and 3380 to PCI. Median presentation time delay,was not different.140 m,in PCI& 143m for FL.11%. Result: 1)PCI was associated with: 37% reduction in 30 days mortality. 2)Reinfarction occurred in 6.7 % of FL pts, and in only 2.4% of PCI patients. **European heart journal(2006)27, Author:Eric Boersma,et al. PPCI versus in-hospital fibrinolysis(FL), in AMI..")
15
Analysis:7084 underwent primary PCI;3078 PHT,and 16043 IHT. Result;primary PCI was associated with lower mortality than IHT at 30 days (4.9%) Vs (11.4%),plus reduced duration of hospital stay,readmission,and reinfarction. **JAMA,October 11-2006-vol 296,No 14 1749.Author:U Analysis:7084 underwent primary PCI;3078 PHT,and 16043 IHT. Result;primary PCI was associated with lower mortality than IHT at 30 days (4.9%) Vs (11.4%),plus reduced duration of hospital stay,readmission,and reinfarction. **JAMA,October 11-2006-vol 296,No 14 1749.Author:U Long term outcome of Primary PCI VS Prehospital(PHT) and In hospital thrombolysis (IHT),for patients with ST MI.
 Vs (11.4%),plus reduced duration of hospital stay,readmission,and reinfarction. **JAMA,October vol 296,No Author:U Analysis:7084 underwent primary PCI;3078 PHT,and IHT. Result;primary PCI was associated with lower mortality than IHT at 30 days (4.9%) Vs (11.4%),plus reduced duration of hospital stay,readmission,and reinfarction. **JAMA,October vol 296,No Author:U Long term outcome of Primary PCI VS Prehospital(PHT) and In hospital thrombolysis (IHT),for patients with ST MI..")
16
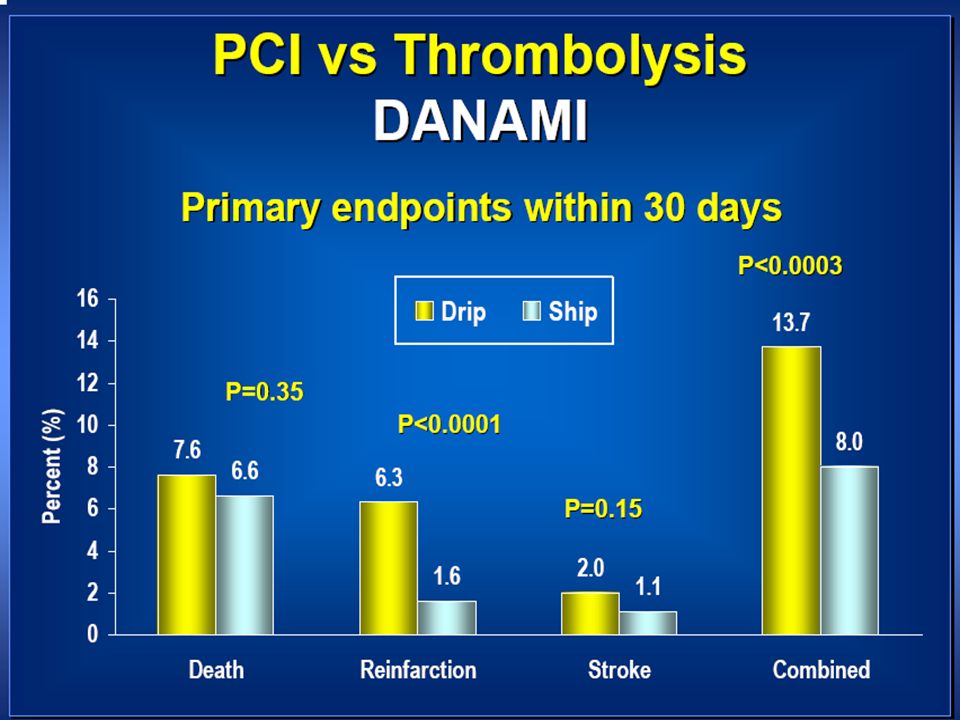
Methods: 225 pts were assigned to recive PPCI& 226 pts to accelerated TPA: (15 mg bolus,then infusion of 0.75mg/kg for 30m, then 0.5 mg/kg for 60 minutes.) Results: composite end points were reduced in PPCI 10.7% when compared to17.7%(TT) At 6 weeks. At 6 month it was 12.4%(PPCI) Vs 19.9%(T.T) **JAMA,April 17.2002-volume 287,No.15 1943. thrombolytic therapy (TT) Vs primary PCI for AMI,To hospitals without on site Cardiac surgery.
 Vs 19.9%(T.T) **JAMA,April volume 287,No thrombolytic therapy (TT) Vs primary PCI for AMI,To hospitals without on site Cardiac surgery..")
17
Way of Nature Eventful Progress from Drip To Ship

18
Type of Reperfusion Therapy for STEMI Patients IV Lytic PPCI Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5 Patients, % 6.9 38.8 47.0 22.7

22
NSTEMI and STEMI: Findings in 2,072,715 Patients STEMI NSTEMI Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5 Patients, % n=938,675 n=1,134,040 missing 354,435 patients from NRMI 1 59.1 37.3 40.9 62.7

23
STEMI : Absence of Initial Reperfusion Therapy Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5 Patients, % Immediate CABG – Range 0.9 % - 1.7 % 37.0 45.3

24
Absence of Reperfusion: Influence of Age Year of Discharge ≤ 65 Yrs > 65 Yrs NRMI 2 NRMI 3 NRMI 4 NRMI 5 Patients, % 58.8 53.2 30.9 22.9

25
Absence of Reperfusion: Influence of Gender Year of Discharge Males Females NRMI 2 NRMI 3 NRMI 4 NRMI 5 Patients, % 54.4 46.8 40.1 32.0

26
Hours (Median) 2.0 1.6 Symptom to Door Times: STEMI Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5
 Symptom to Door Times: STEMI Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5")
27
Door to Balloon Times Among Patients Transferred in NRMI 4 Door to Data: 50 th : 9 Min. 25 th : 4 Min. 75 th : 16 Min. Data to Cath Lab Arrival: 50 th : 132 Min. 25 th : 88 Min. 75 th : 219 Min. Cath Lab to Balloon: 50 th : 37 Min. 25 th : 28 Min 75 th : 50 Min. 9 132 37 Total Door 1 to Balloon Time: 185 minutes (25 th : 137; 75 th : 276) Percent of Patients with Door to Balloon Time < 90 Min = 3.0% Sample Size: 1,346; Time Period: January 2002 – December 2002
 Percent of Patients with Door to Balloon Time < 90 Min = 3.0% Sample Size: 1,346; Time Period: January 2002 – December")
28
Times to Treatment in Transfer Patients Undergoing PPCI for AMI: NRMI 3/4 Analysis Nallamothu, Circulation. 2005; 111:761-767 Analysis of 4278 pts transferred for PPCI Analysis of 4278 pts transferred for PPCI Initial Door to Balloon InflationTime

29
Door to Drug Times - Median Values 40 30 46 33 Year of Discharge NRMI 2NRMI 3NRMI 4 NRMI 5 Minutes (Median) Transfer Non-transfer
 Transfer Non-transfer")
30
Door to Balloon Times According to Time of Day Minutes (Median) Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5 103 130 114 80 99 92
 Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI")
31
Door to Balloon Times According to Workday 125 75 100 98 On-Hours Off-Hours Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5 Minutes (Median) No Transfers
 No Transfers")
32
Minutes (Median) 93 62 Door-to-Balloon Times Year of Discharge 120 96 Door to Balloon Door to Cath NRMI 2 NRMI 3 NRMI 4 NRMI 5
 Door-to-Balloon Times Year of Discharge Door to Balloon Door to Cath NRMI 2 NRMI 3 NRMI 4 NRMI 5")
33
Percent of Patients Door-to-Balloon Time < 90 Minutes 29.8% 44.8% Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5

34
NRMI Survey 2004 (1994-2003), Door to Balloon Times are in excess of guidelines: (often for patients presenting directly to PCI hospitals and almost invariable when a transfer is required) STEMI: Transfer Status PTCA Door-to-balloon times for primary PTCA patients, by primary transfer status. Gibson, CM Am Heart J 2004;148:S29–33. NRMI 1 NRMI 2 NRMI 3 NRMI 4 NRMI transfer-in patients NRMI non-transfer-in patients 180 90

35
Reinfarction Rates - STEMI Patients 3.8 % 2.0% 2.7 % 1.4 % Year of Discharge NRMI 2 NRMI 3 NRMI 4 NRMI 5

36
Median LOS (Days) Median Length of Stay: By Reperfusion Therapy 8.3 7.0 2.8 3.0 Year of Discharge NRMI 1 NRMI 2 NRMI 3 NRMI 4 NRMI 5
 Median Length of Stay: By Reperfusion Therapy Year of Discharge NRMI 1 NRMI 2 NRMI 3 NRMI 4 NRMI 5")
37
Deaths in hospital, % PPCI IV Lytic Mortality During Hospitalization by Reperfusion Therapy 3.8 % 3.7 % 5.5 % 8.6 % Year of Discharge NRMI 1 NRMI 2 NRMI 3 NRMI 4 NRMI 5

40
“Time is Muscle”: PTCA GUSTO-IIb and NRMI-2 registry 27.000 pt Strong relationship between the “door to balloon” time and mortality. Cannon et al, JAMA 2000; 283: 2941

43
NERMI: Conclusions STEMI patients represent a decreasing proportion of those presenting with AMI (37%) There has been little improvement in increasing the proportion of patients who receive some form of early reperfusion therapy (37%). Women and the elderly are less likely to receive early reperfusion therapy. Primary PCI now exceeds lytic therapy as the mode of early reperfusion.

44
NERMI: Conclusions Symptom to door times are declining but still remain too long (1.6 hrs) Door to drug times have declined over time from 40-46 minutes to 30-33 minutes and are not affected by inter-hospital transfer. Door to balloon times have decreased from a median of 120 to 96 minutes and are profoundly affected by transfer and time of day. Less than half of patients achieve a door to balloon time of < 90 minutes and even for non-transfers the rates is only 53%.

Similar presentations




































 Between Symptom Onset and Treatment GUSTO III 95-97 GUSTO III 95-97 InTIME II 97-99 InTIME II 97-99 ASSENT.>")
