Download presentation
Presentation is loading. Please wait.

1
HPB DAY

2
Plan today 4 cases4 cases ImagesImages Present range of approachesPresent range of approaches DiscussionDiscussion

3
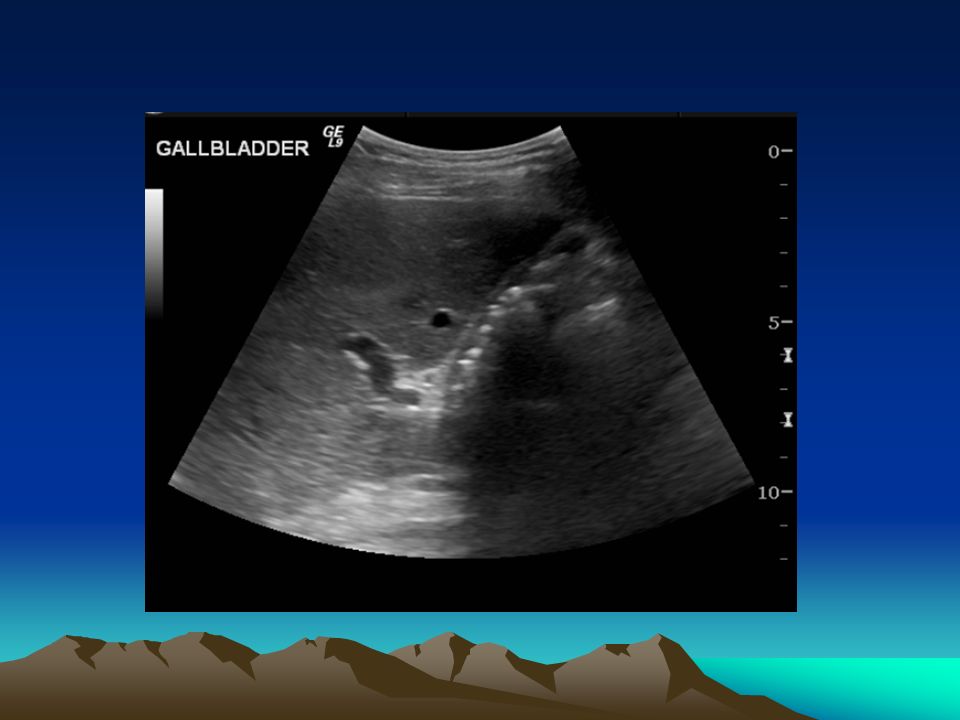
38 year old female, 6 month history of recurrent attacks of severe epigastric pain -> back. Possibly dark urine at times USS…

5
USS… Lap chole…

6
Hepatobiliary Pathology Or how I learned to stop worrying and love the gallstone…

7
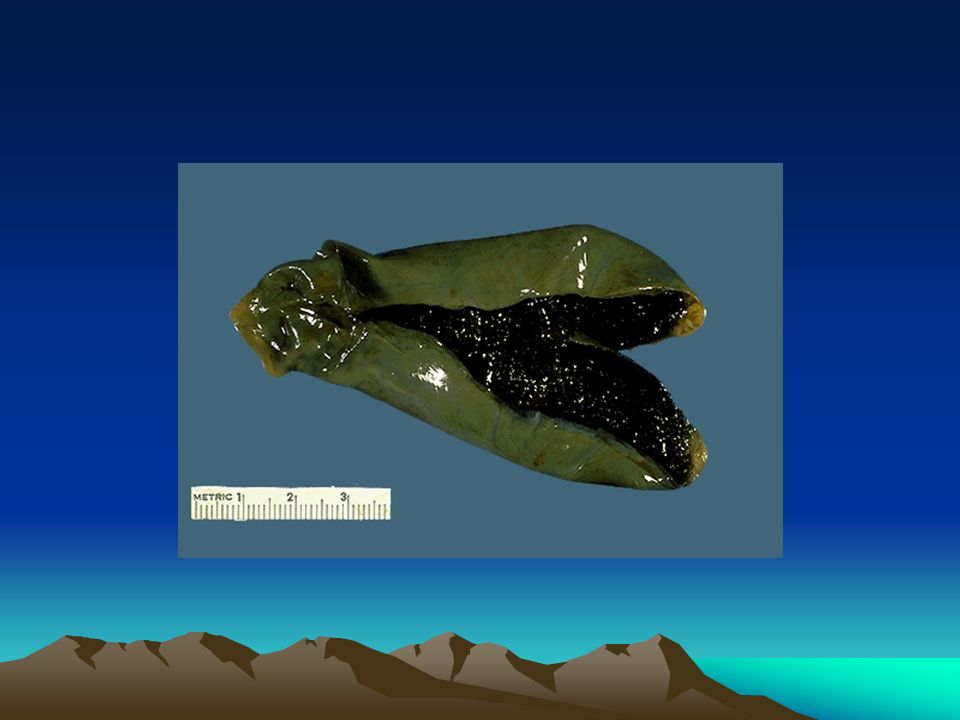
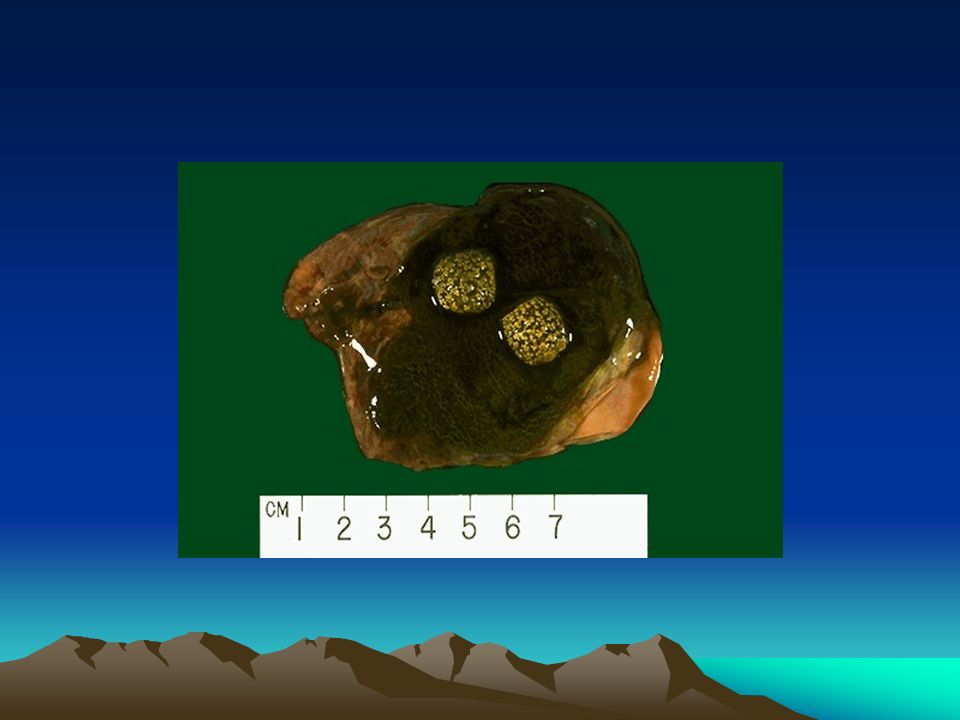
Cholesterol Stones Hypersecretion of cholesterol Decreased bile salt secretion Odd gallbladder Old, female, pregnant, obesity, rapid weight loss, ethnicity,impaired GB motility e.g. parenteral nutrition

8
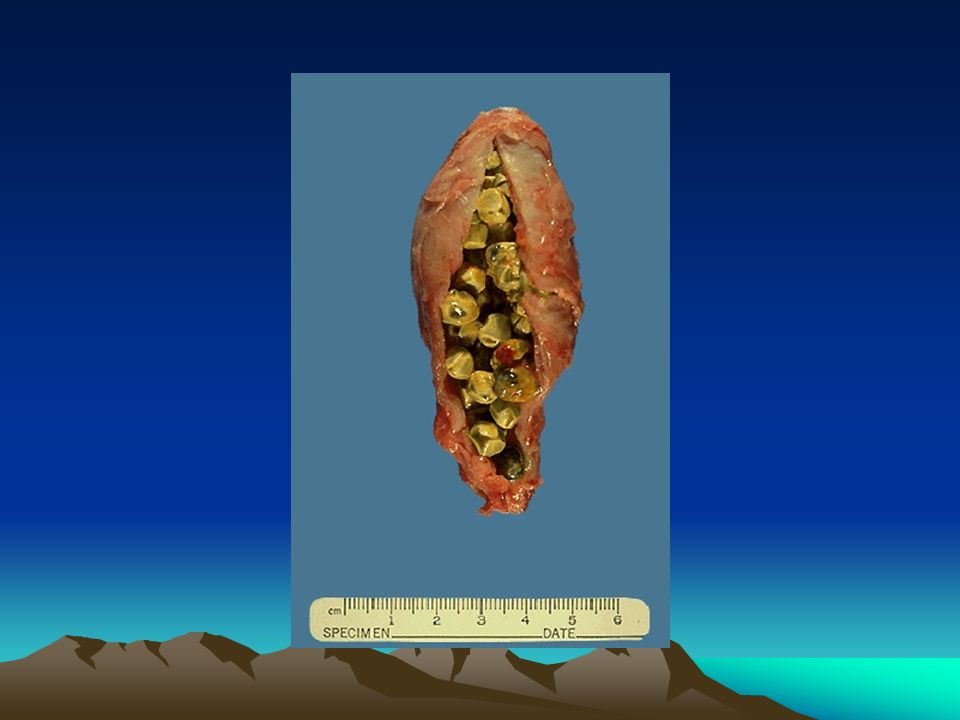
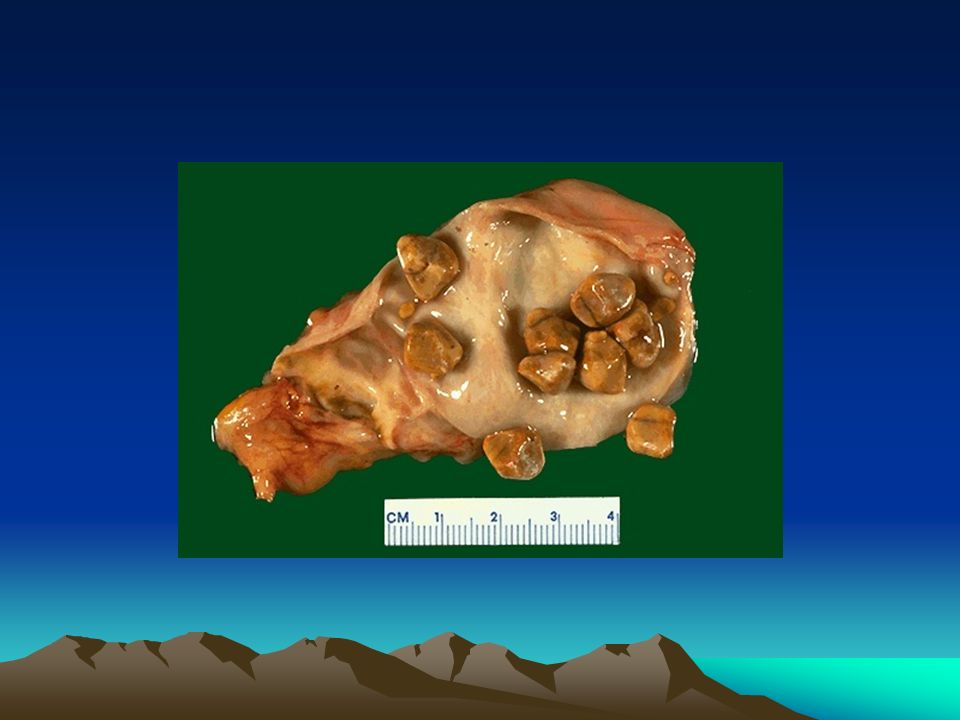
Pigment (haem) Stones Calcium bilirubinate Chronic haemolysis
 Stones Calcium bilirubinate Chronic haemolysis")
18
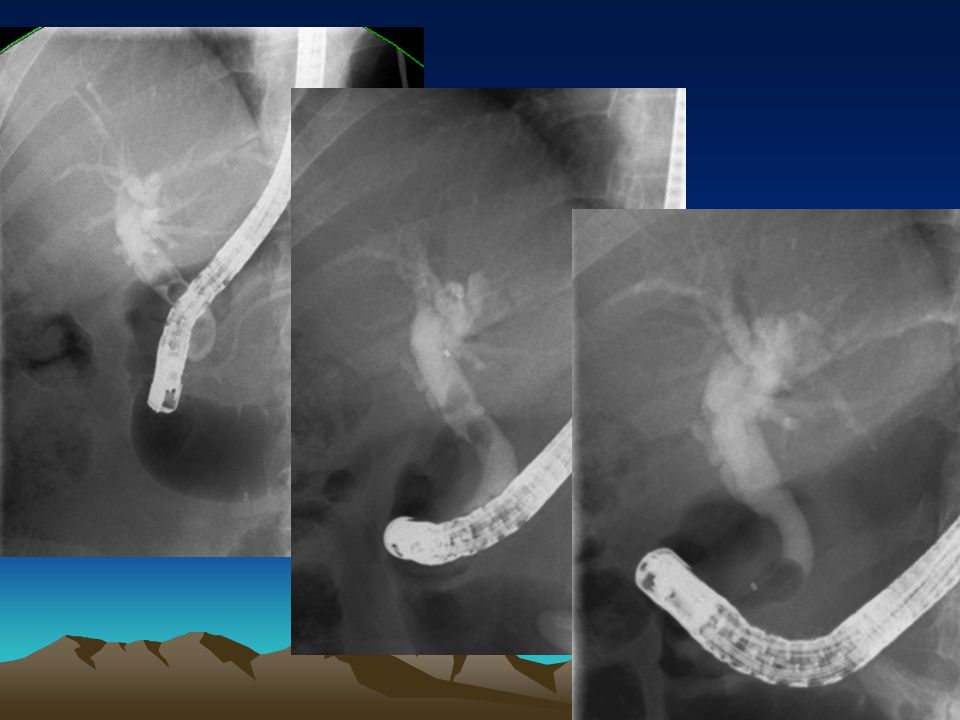
38 year old female, 6 month history of recurrent attacks of severe epigastric pain -> back. Possibly dark urine at times USS…USS… Lap chole…Lap chole… 5 days postop readmitted with severe abdominal pain….. Why, what investigationsWhy, what investigations

19
USS (CT) Unremarkable What else …
 Unremarkable What else …")
24
How might we identify preop which patients may harbour CBD stones….

25
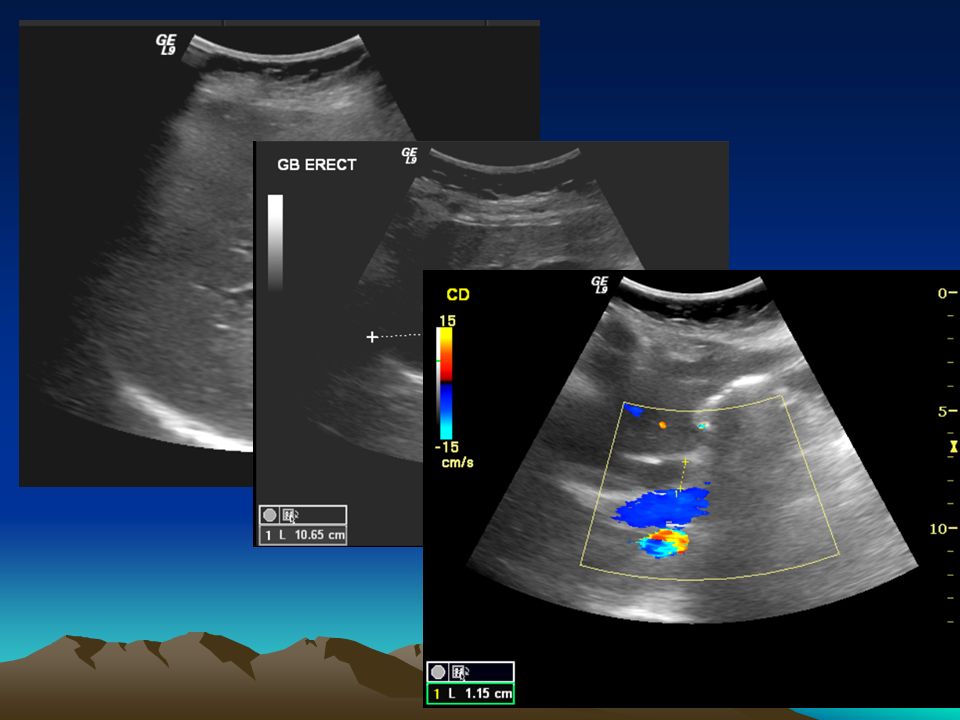
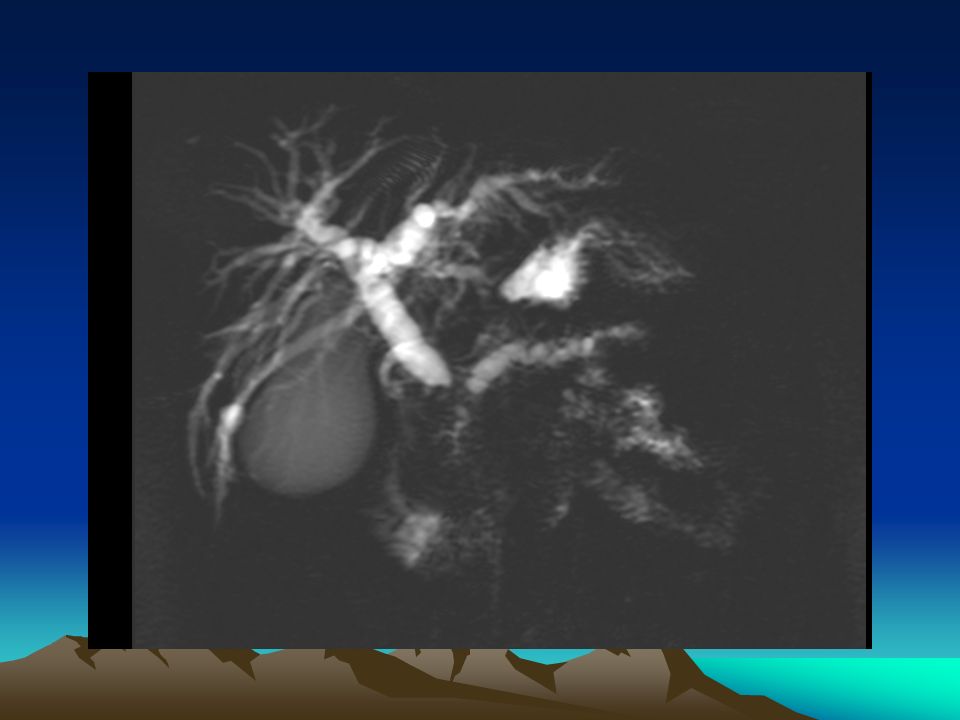
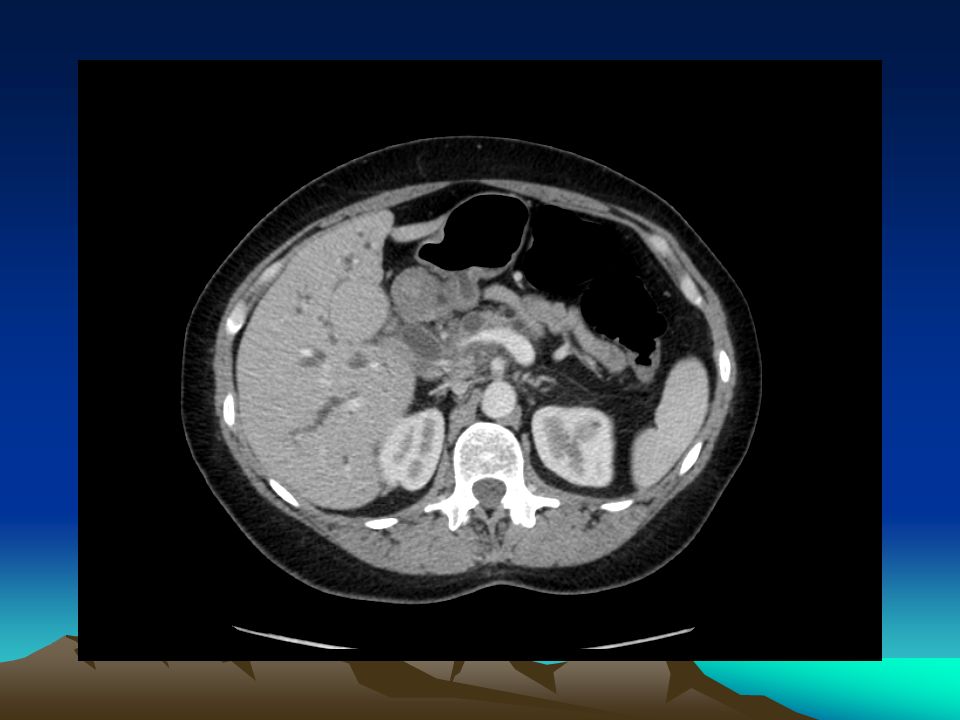
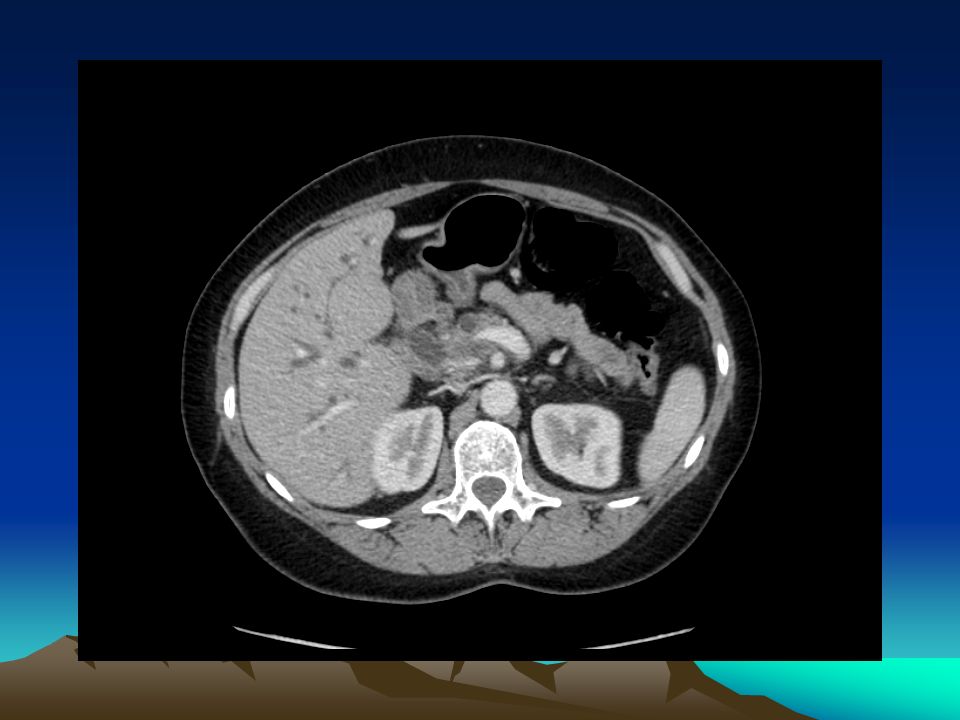
44 year old female with 2 week history of obstructive jaundice OK LFTs but so what USS:

41
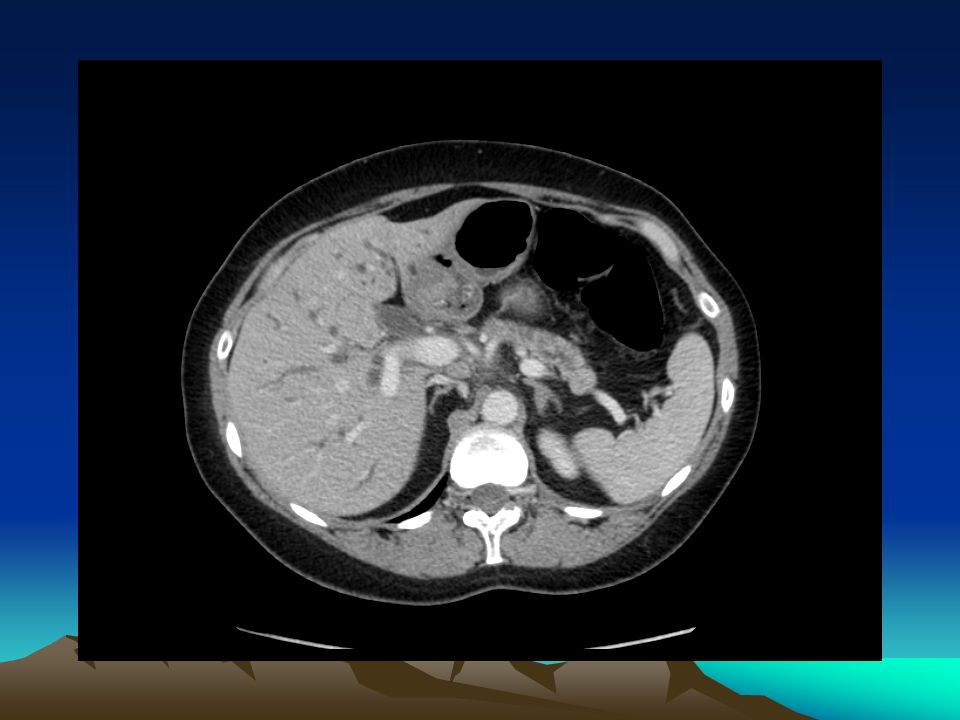
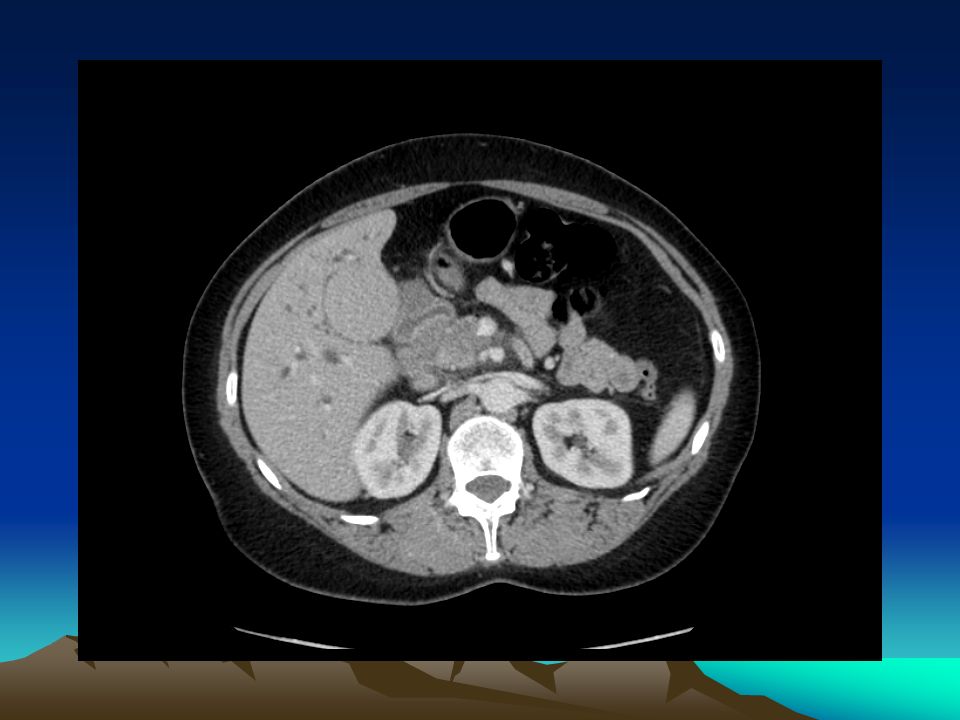
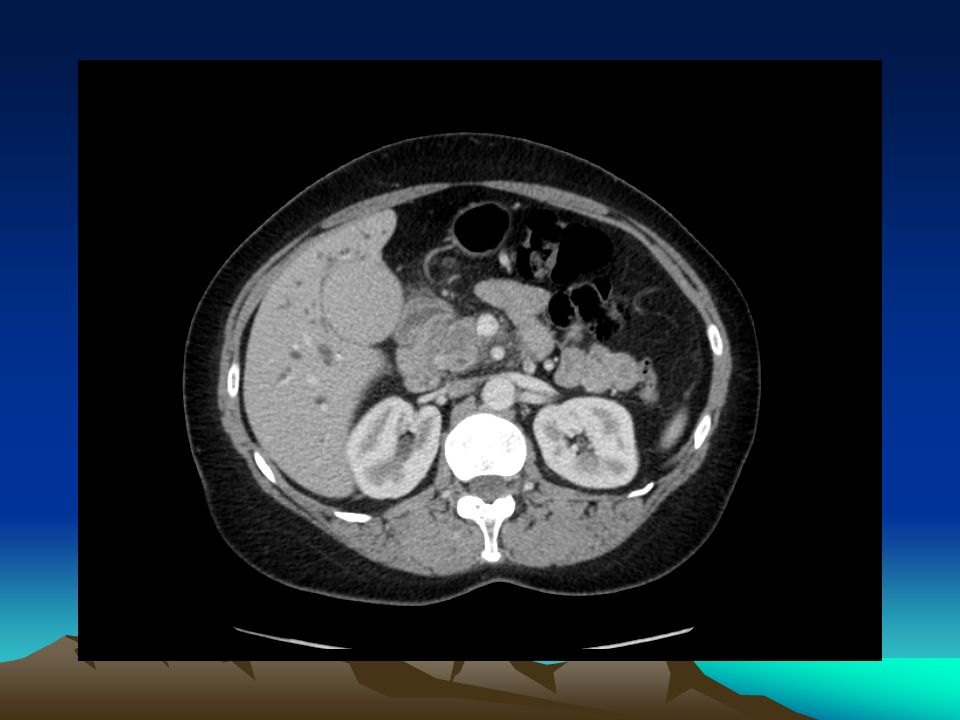
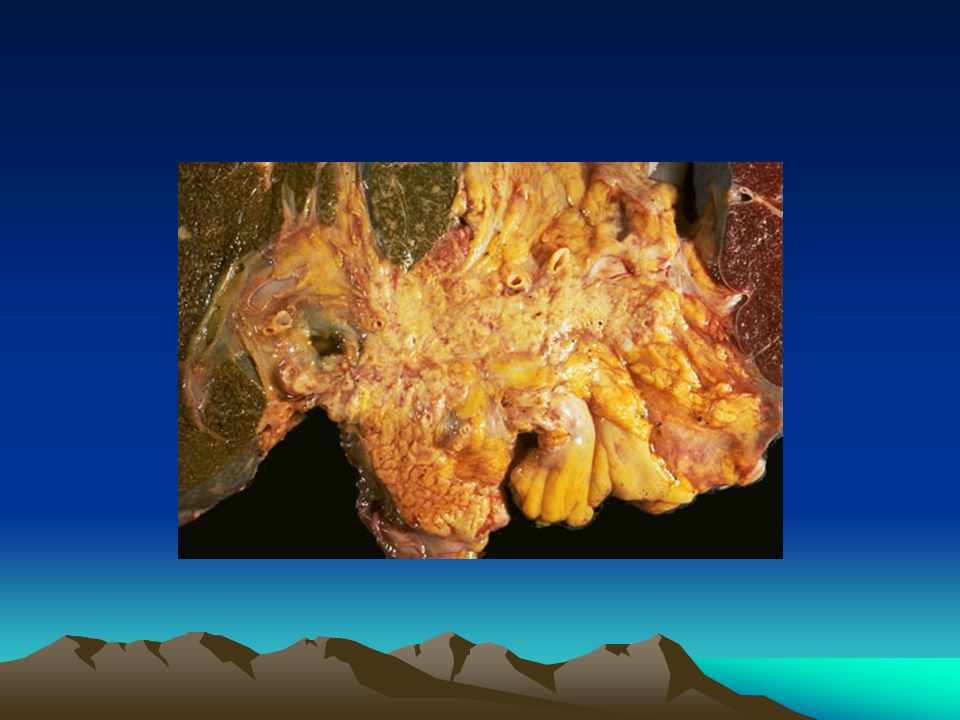
68 year old female with 2 week history of obstructive jaundice USS: CBD 16mm GB distended, no stones CT scan – unresectable ca pancreas Palliative R…. Stent - route

42
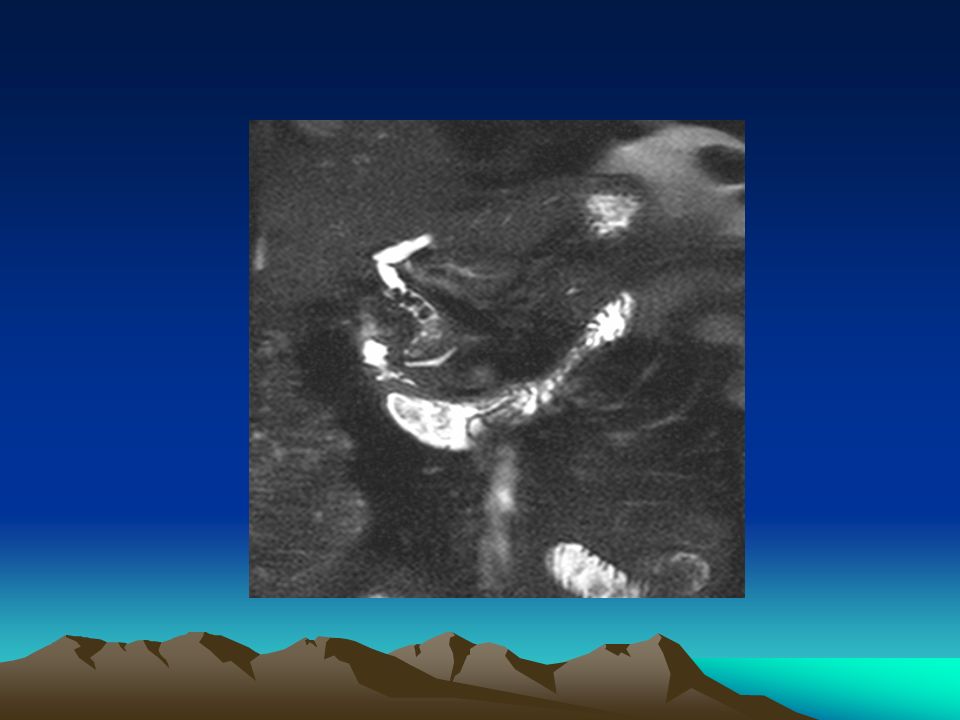
ERCP Stent

44
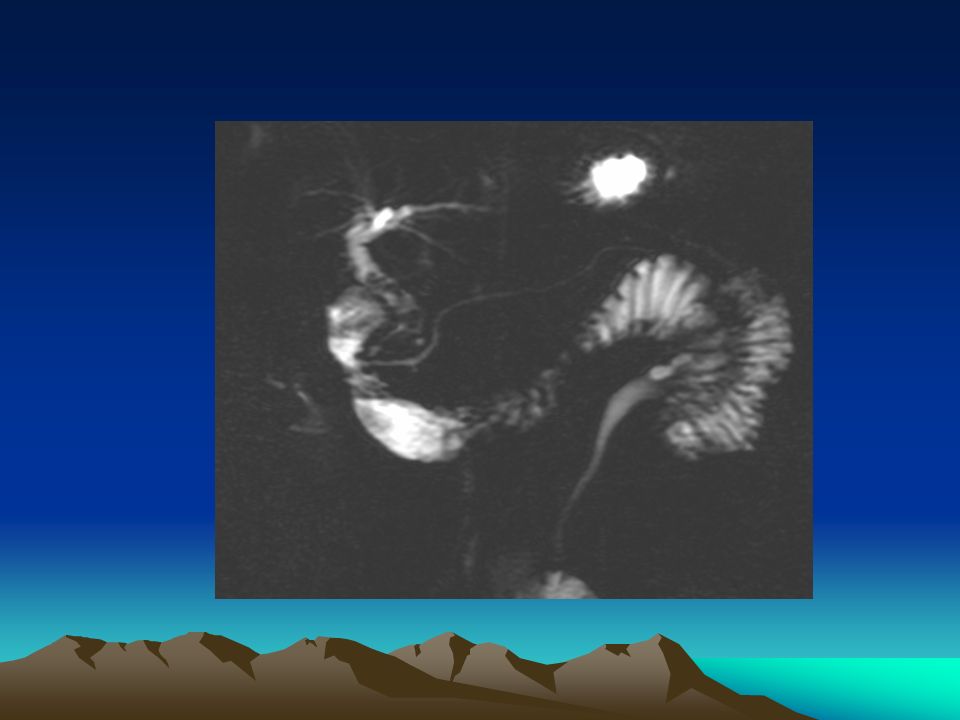
Percutaneous transhepatic cholangiography Indications Determination of obstructive jaundice Level of obstruction Persistent pain after GB removal Contraindications Close to 100% sensitivity and specificity in identifying cause and level of obstruction

45
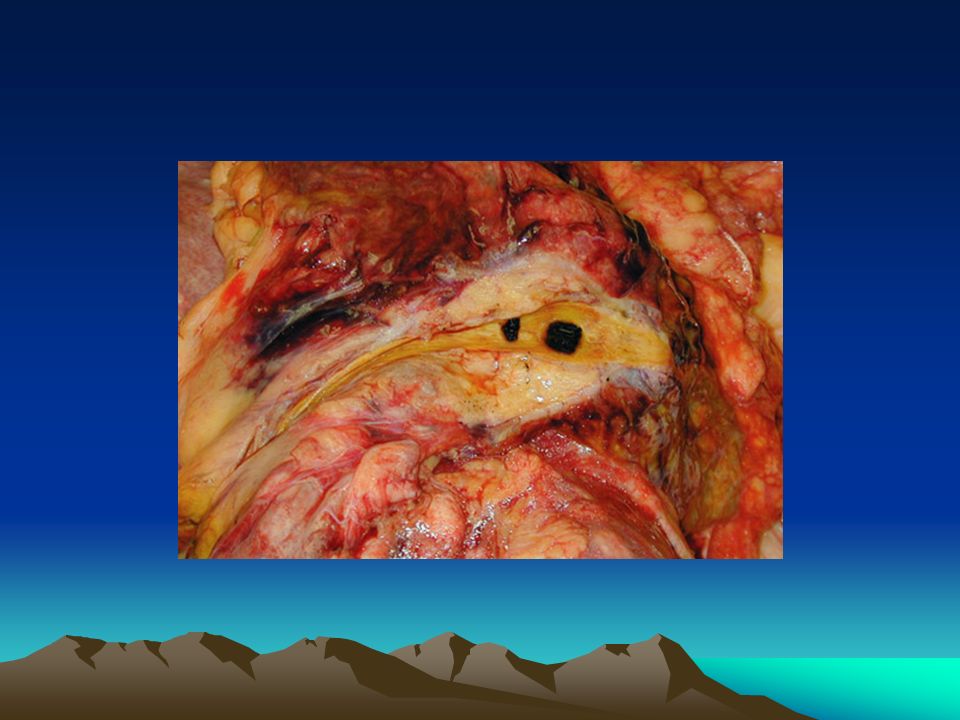
Self-expanding stent placed in the CBD of patient with non-resectable pancreatic tumour

47
Palliative Treatment: (Biopsy) – including EUS Gemcitabine
 – including EUS Gemcitabine")
50
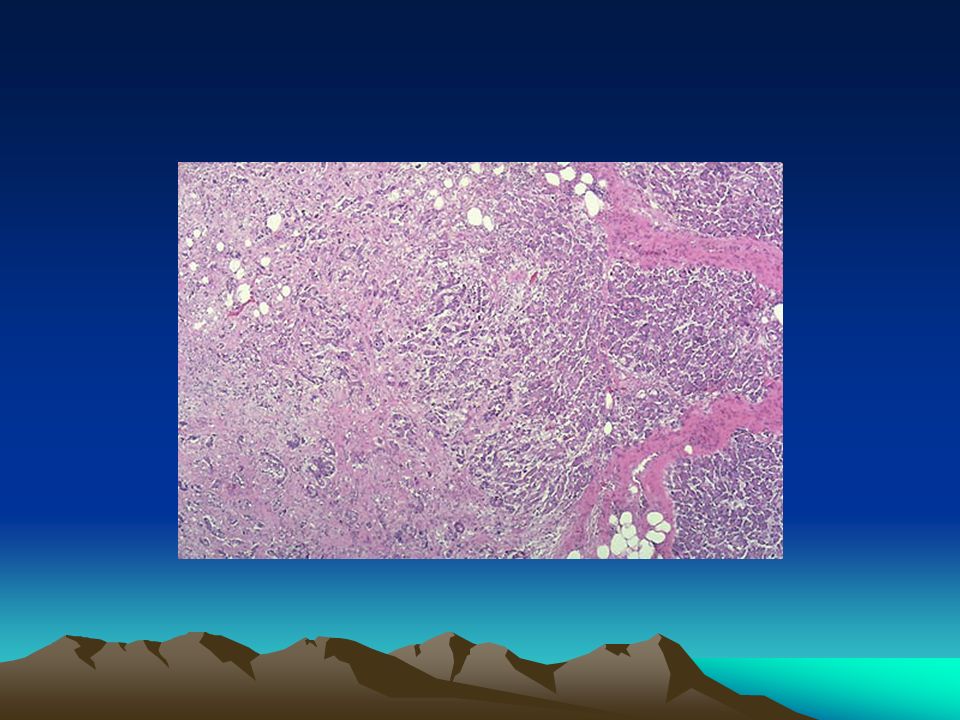
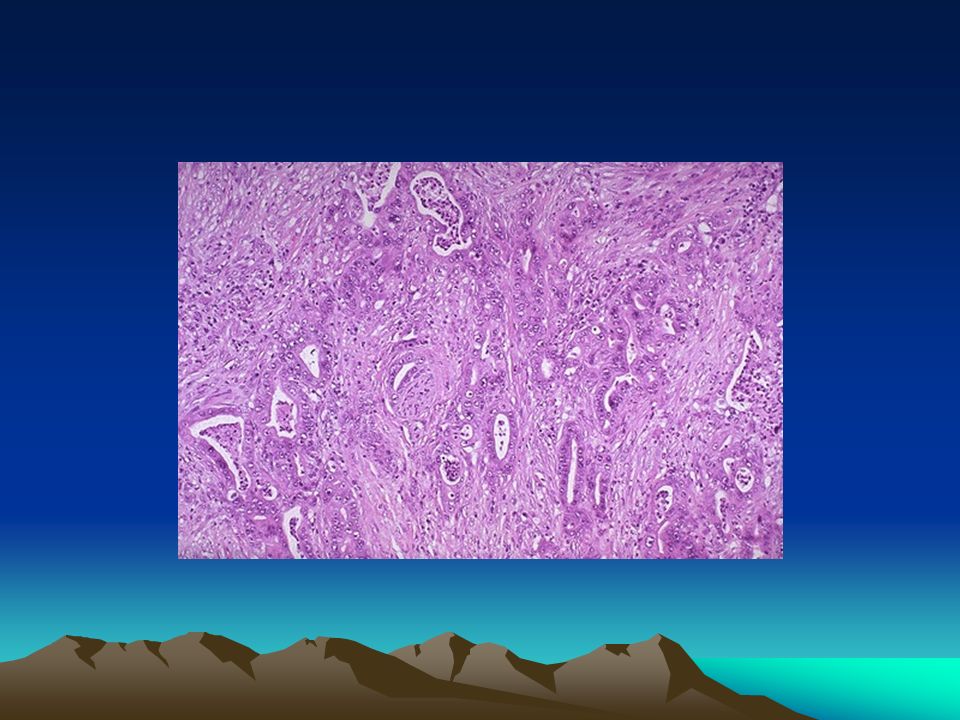
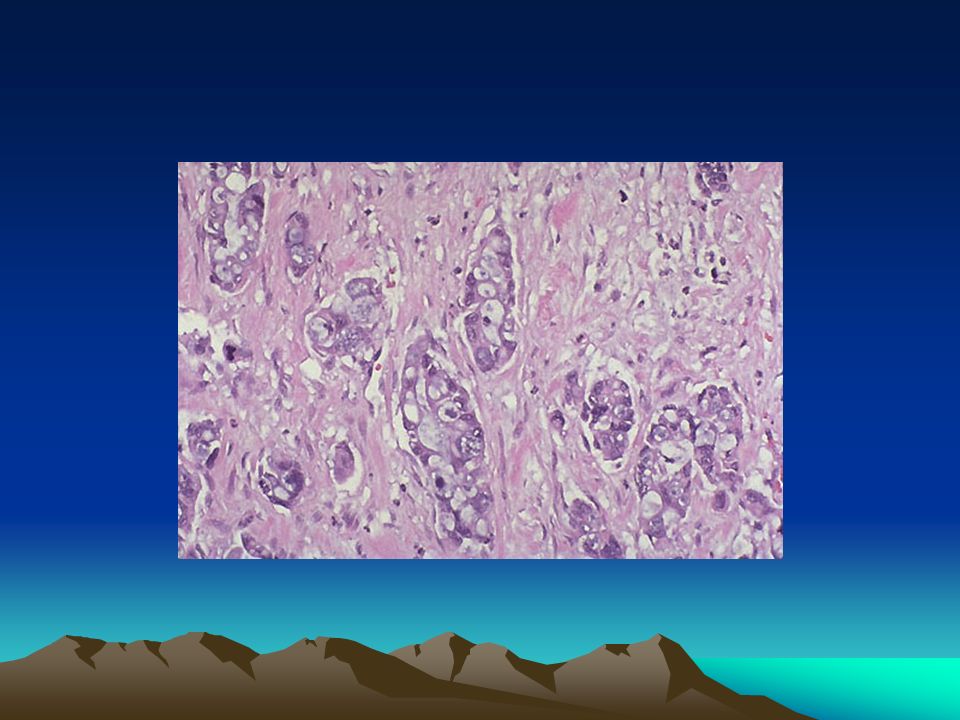
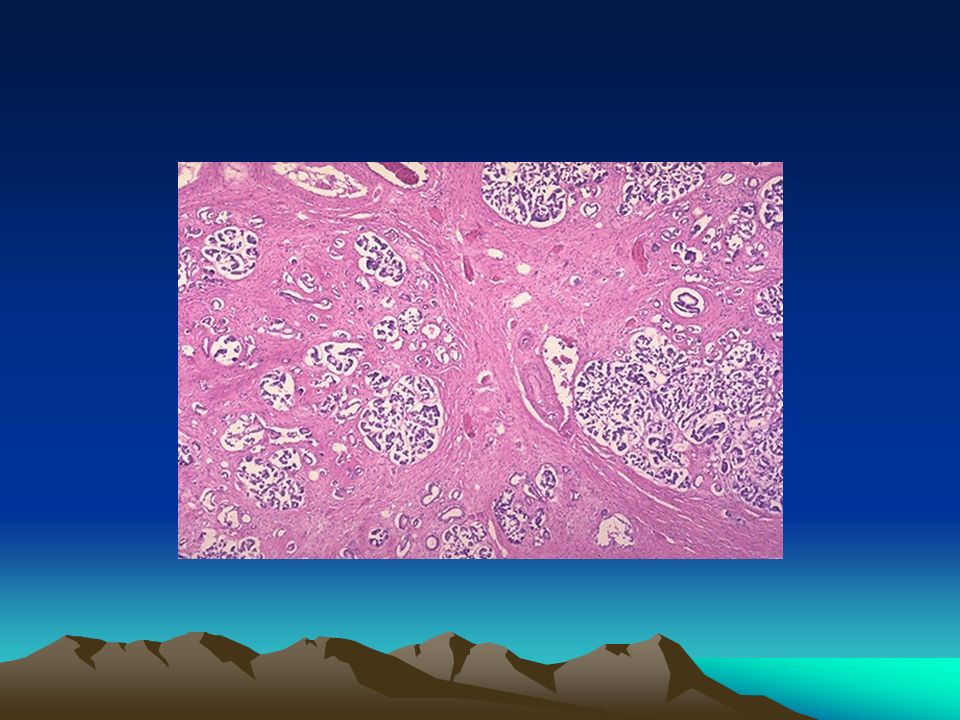
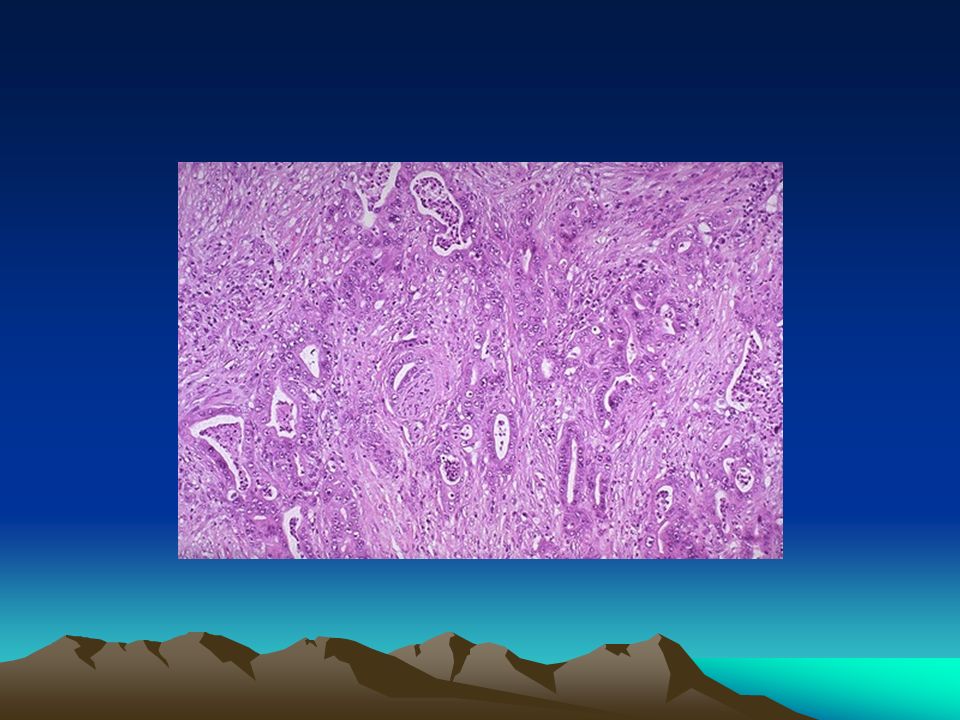
Pancreatic Cancer Adenocarcinoma Exocrine Pancreas Older, males > females, fags, booze, fat, carbs. BRACA-2, PJS 60, 10, 10% (Head, body, tail) 80% outside pancreas at diagnosis CA 19/9.
 80% outside pancreas at diagnosis CA 19/9..")
55
If it had been operable…

59
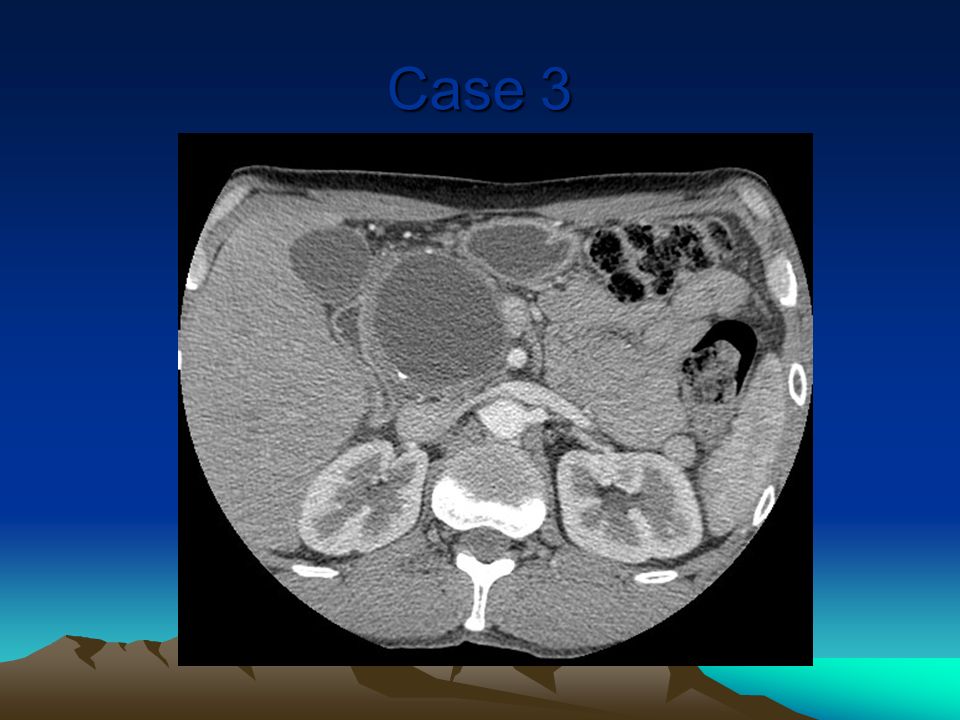
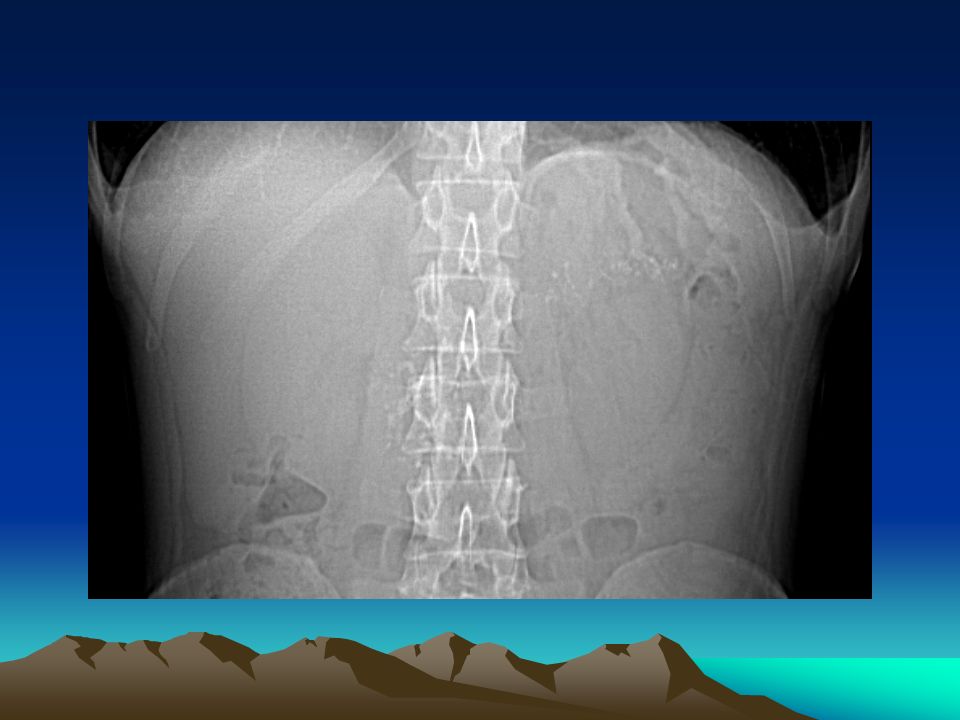
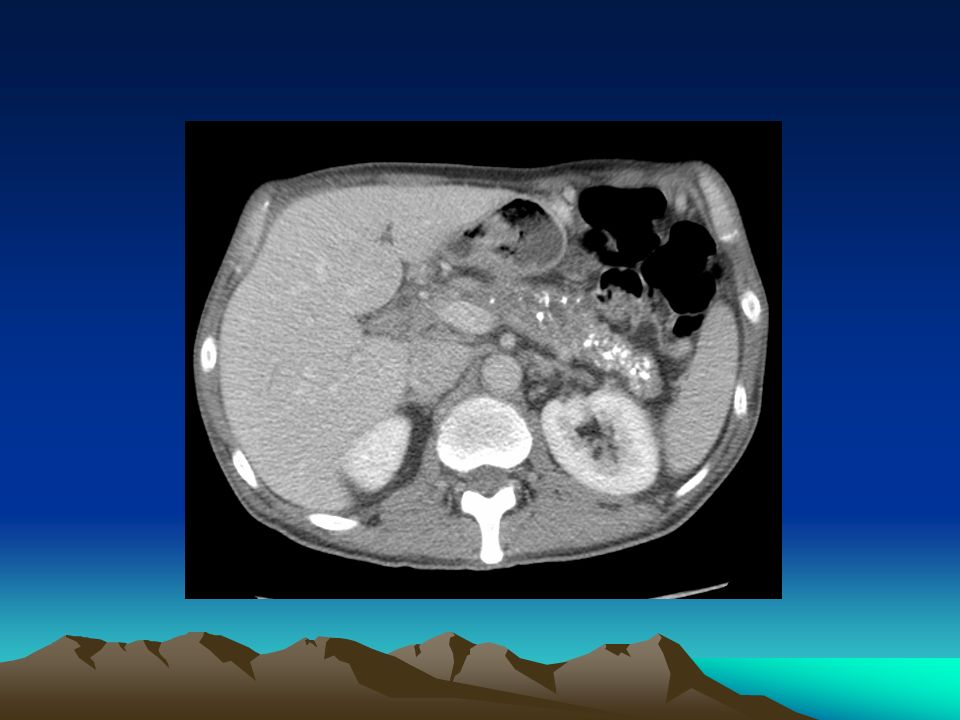
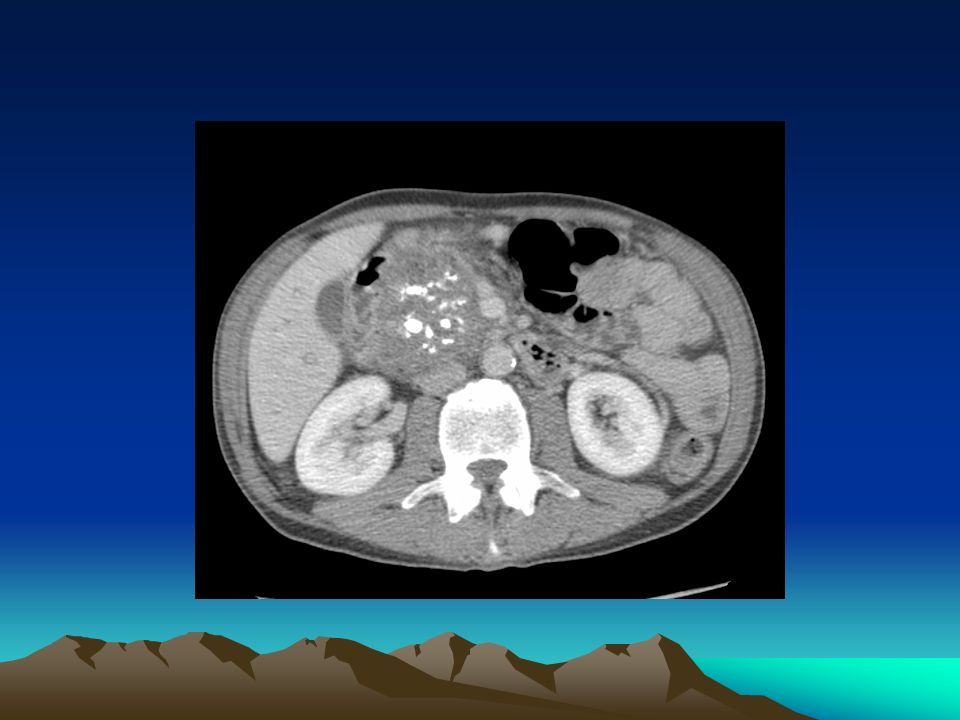
47 year old male. 3 year history of epigastric pain -> back. Rather constant. Worsening over 6 months. Stools recently rather loose. Thoughts…. USS ….

60
Case 3

62
Some other images

66
How to treat pseudocysts??

67
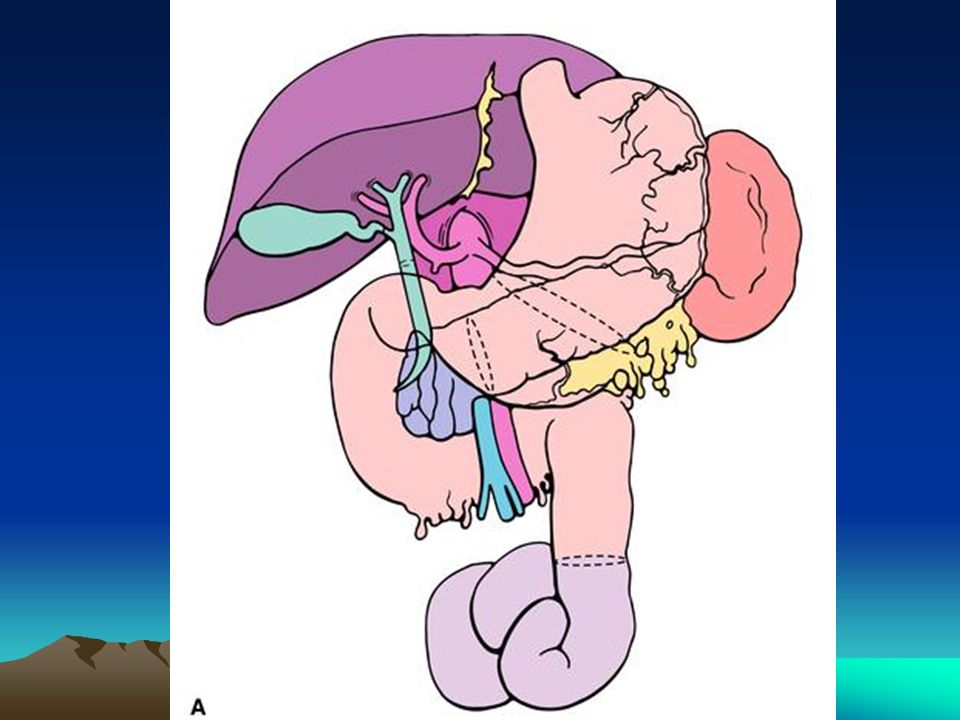
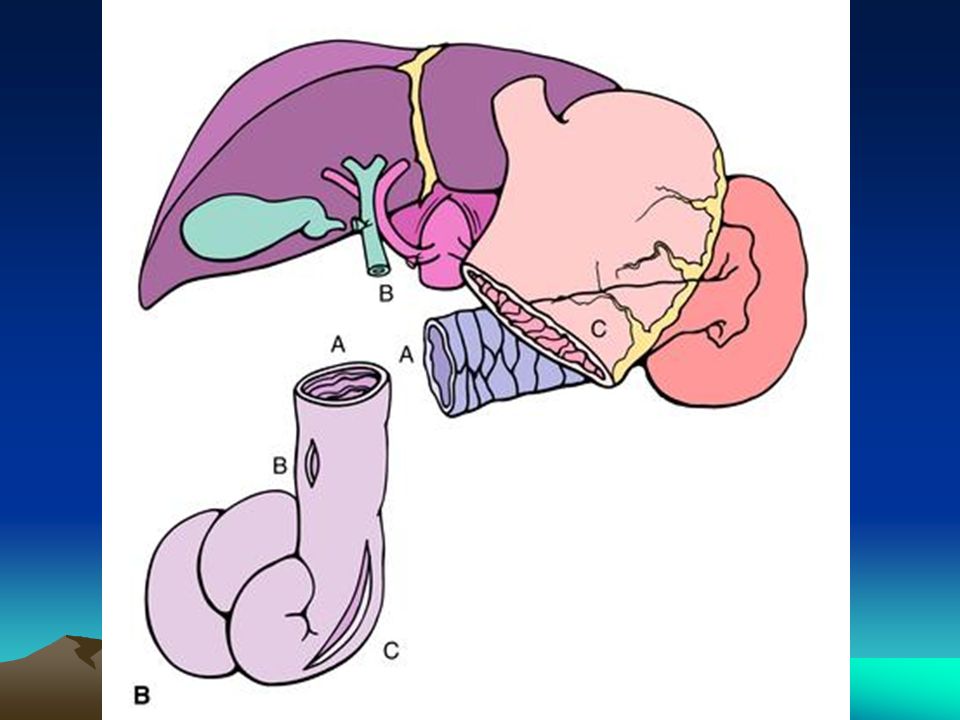
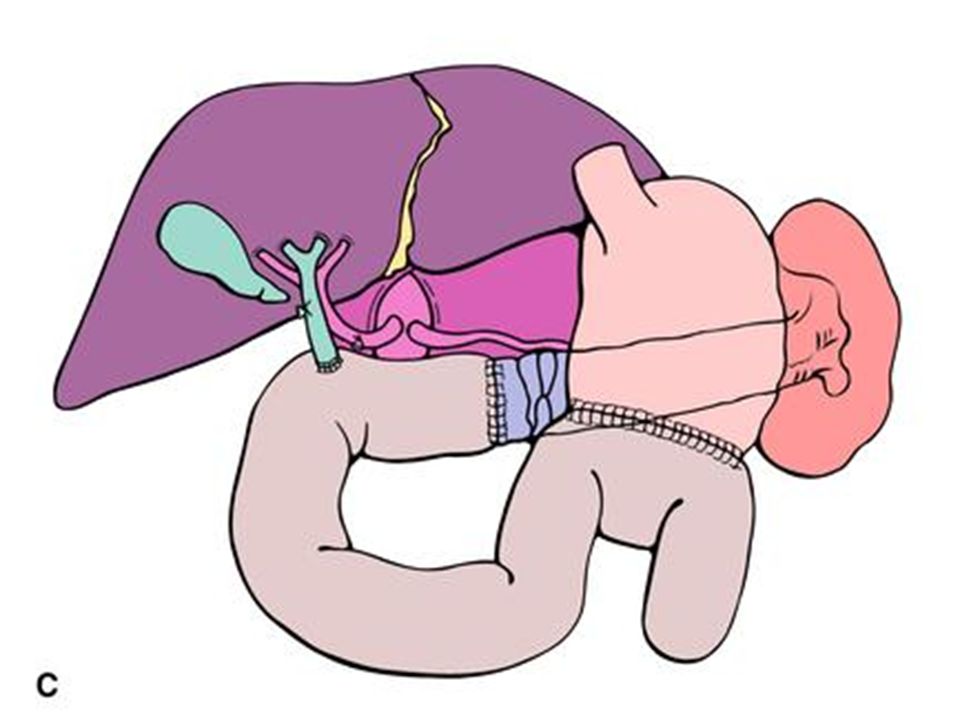
Pancreatic Anatomy Consists of head, ucinate process, meck, body and tail Head lies within C shaped concavity of the duodenum Ucinate process passes posterior to the superior mesenteric vessels Neck is anterior to superior mesenteric vessels Tail ends as it passes between the layers of the splenorenal ligament Pancreatic duct- begins at tail and passes right through the body to the head where joins CBD at A of V. Also accessory pancreatic duct reflects the embryological origin of the pancreas from dorsal and ventral processes.

68
Pseudocyst drainage

73
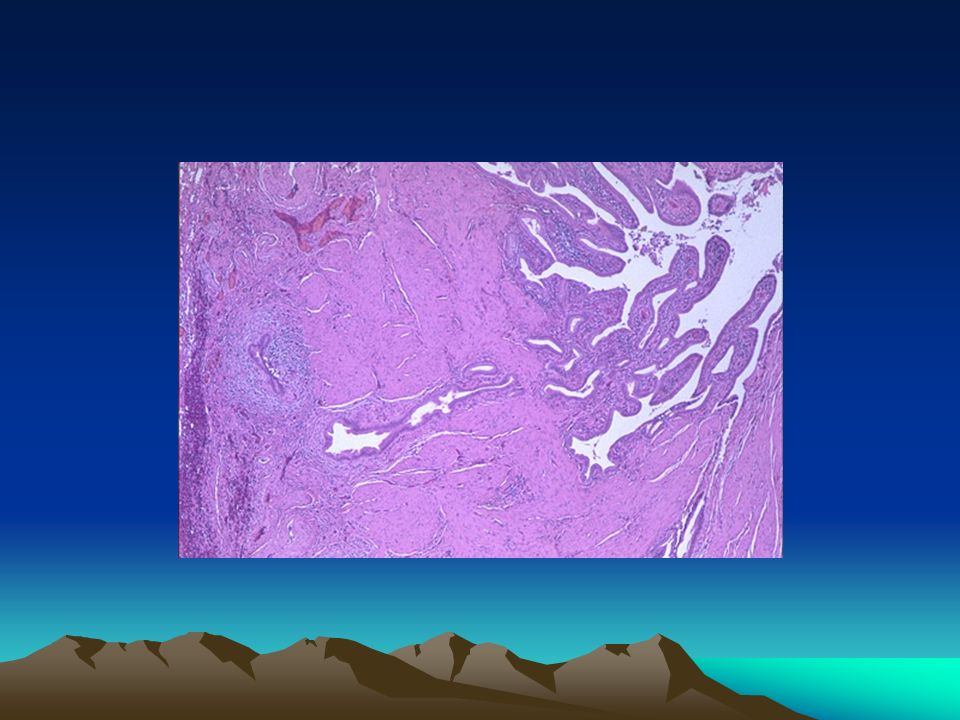
Pancreatic Cysts Non-neoplastic –Pseudocysts –others Neoplastic –Mucinous (cystadenoma) –Papillary/cystic tumours –Cystadenocarcinoma –Degeneration in any cancer FNAC –Steep learning curve
 –Papillary/cystic tumours –Cystadenocarcinoma –Degeneration in any cancer FNAC –Steep learning curve")
74
PANCREATITIS, attempts to clarify MARSEILLES Chronic Pancreatitis Acute Pancreatitis

75
Mild - 80% ?management Severe – 20% total – manage carefully 6% mortality – what of, operations? How to identify the severes

76
Acute Pancreatitis Requires: Small stones Wide cystic duct Decent common channel 1 2

77
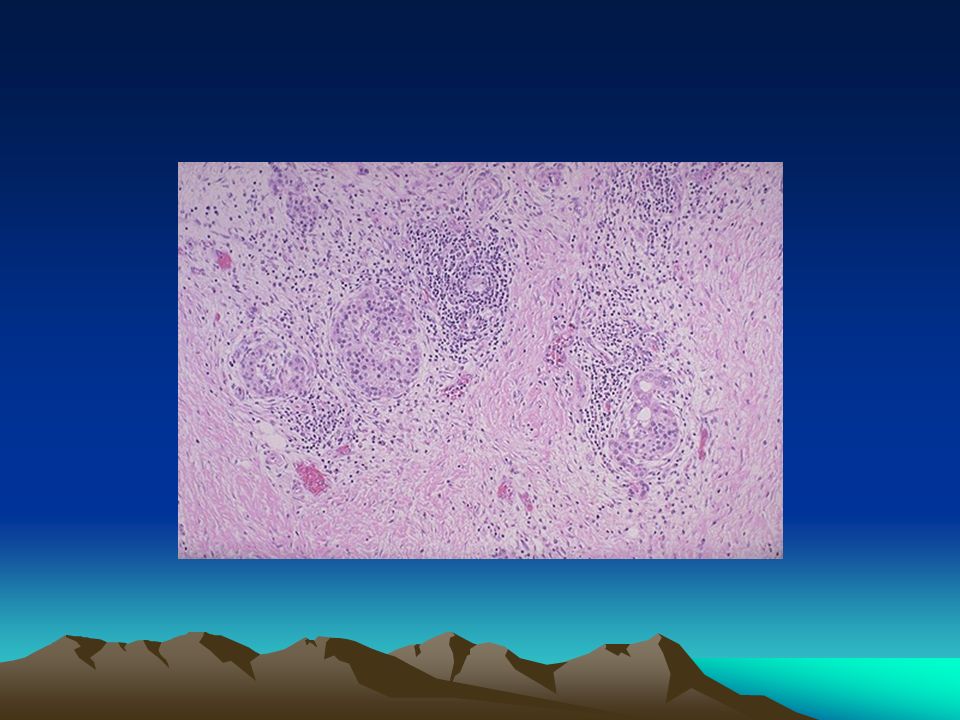
Chronic Pancreatitis Usually alcoholic aetiology Slowly progressive (1/4 if abstain) Will not recover Fibrosis, stone protein, calcification Some have pain Some have episodes of pancreatitis
 Will not recover Fibrosis, stone protein, calcification Some have pain Some have episodes of pancreatitis")
78
Ok its chronic pancreatitis Alcohol … Pain … Diabetes … Steatorrhoea …

79
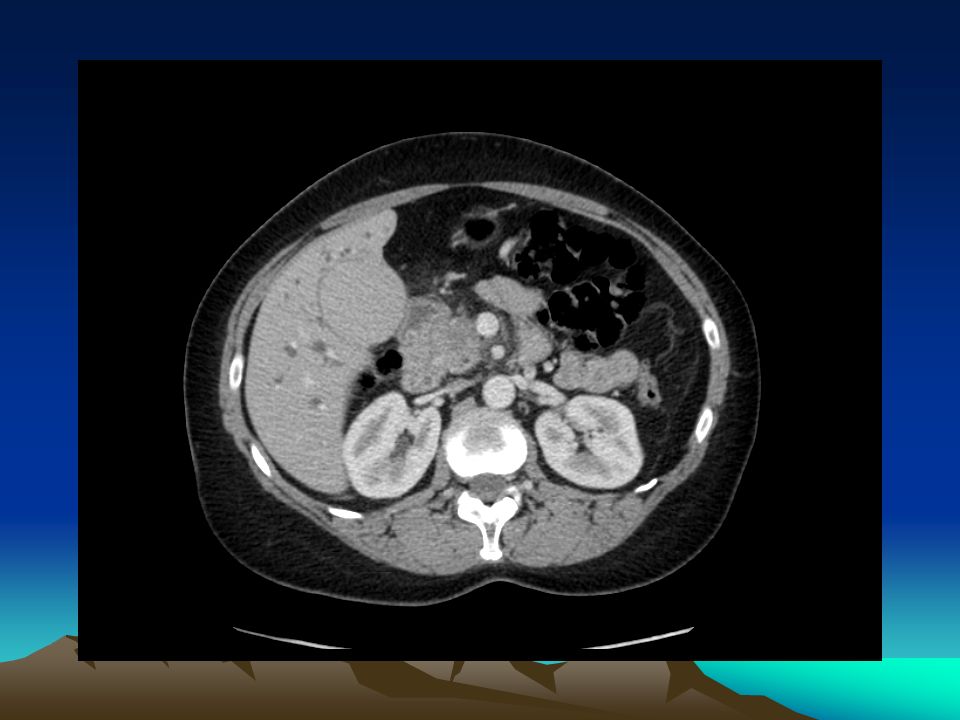
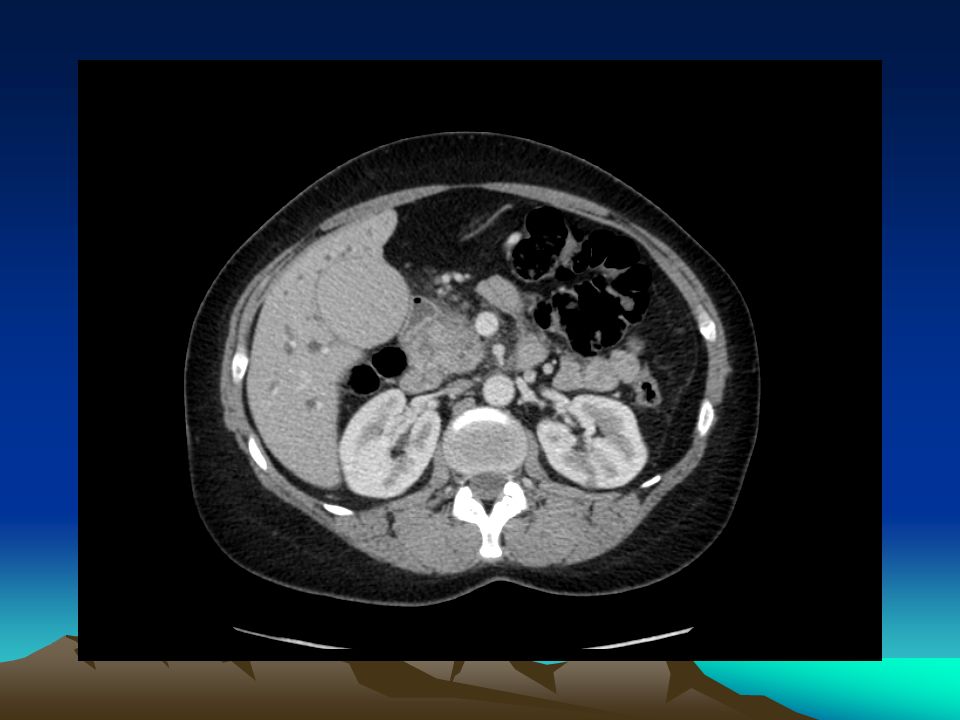
69 year old male referred with an inguinal hernia. Looks terrible. Admits to 3 months of anorexia, lethargy and weight loss. Investigation …

80
Case 4

81
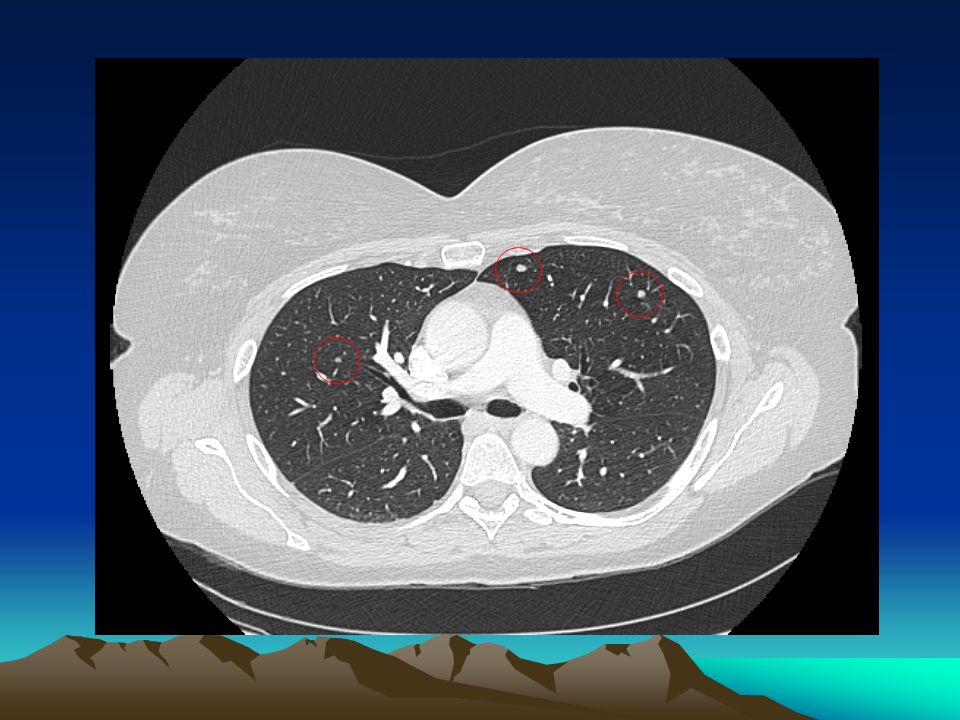
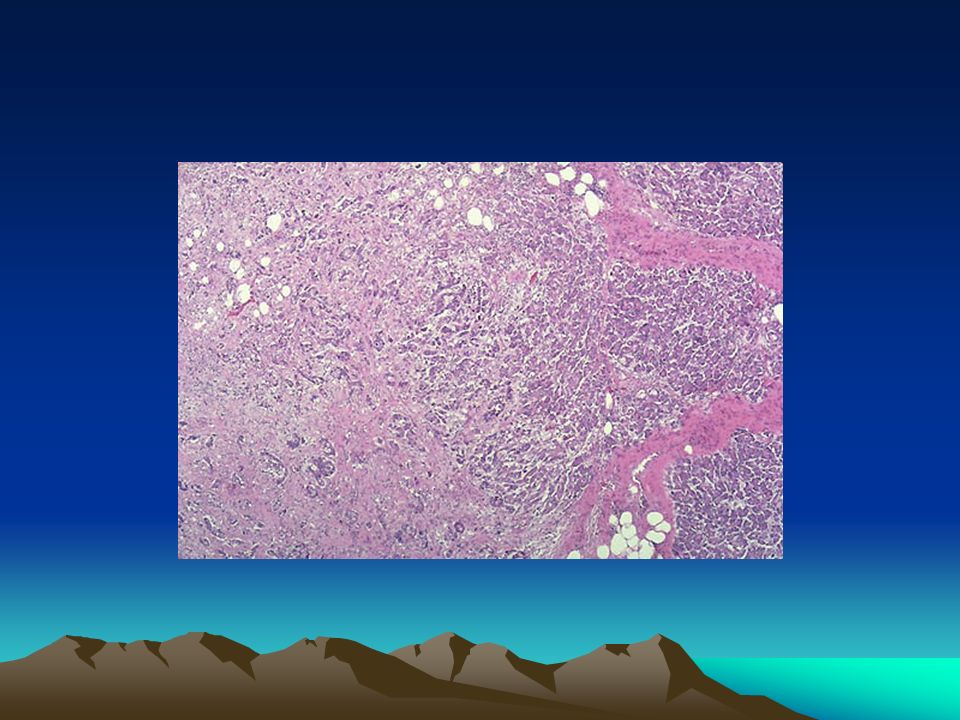
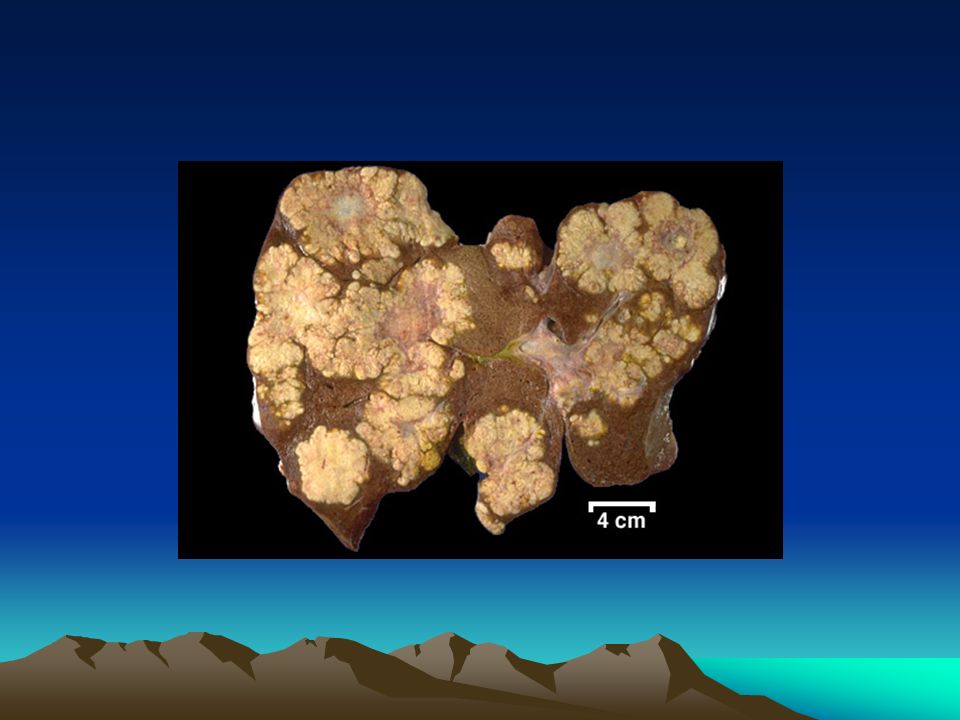
Multiple Liver Mets Hunt the primary?? Why?? Most colorectal, upper GI, pancreas, lung

82
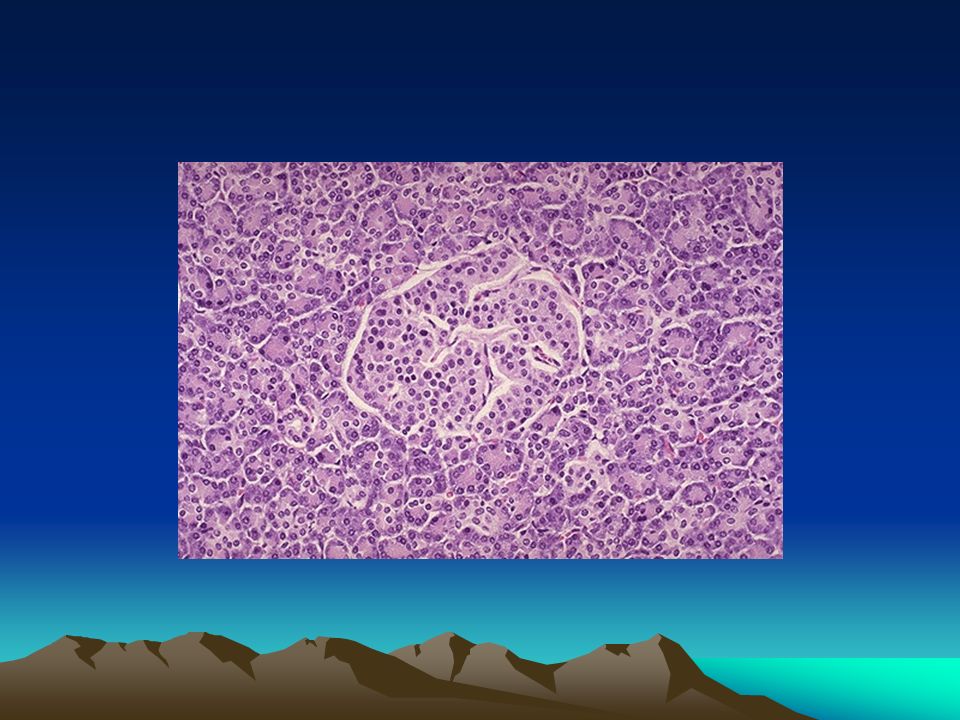
Inoperable liver mets. Hunting? Clinical Imaging +/- biopsy Immunochemistry –Specific (ha ha) markers –Cytokeratin profiles
 markers –Cytokeratin profiles.")
83
Tumours with specific therapies Breast Colorectal Other UGI (Prostate) (Thyroid) Oncology peer pressure
 (Thyroid) Oncology peer pressure")
85
Potential treatments available for some patients Resection Local treatments ….

87
Case 5

88
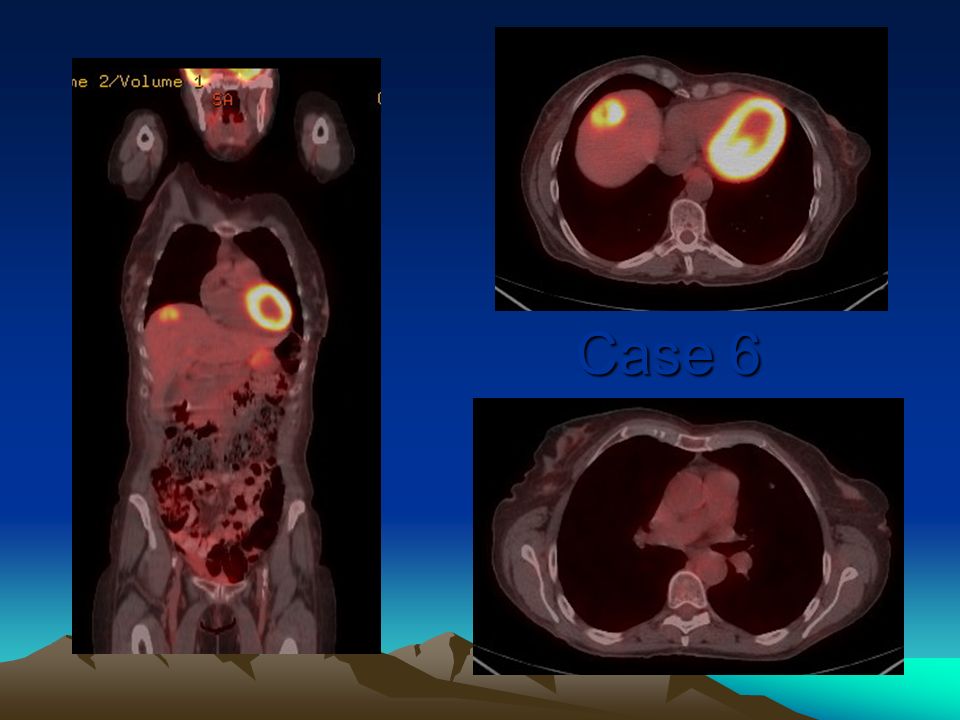
Case 6

90
A few messages to repeat: Don’t forget CBD stones Don’t forget CBD stones ERCP is principally for therapy now ERCP is principally for therapy now Save time, do the right test, ask a radiologist Save time, do the right test, ask a radiologist Tissue diagnosis not always possible in pancreatic cancer Tissue diagnosis not always possible in pancreatic cancer Time is critical in obs jaundice Time is critical in obs jaundice Good palliation from biliary decompression Good palliation from biliary decompression CA 19/9 for pancreatic cancer CA 19/9 for pancreatic cancer GEMCITABINE for pancreatic cancer GEMCITABINE for pancreatic cancer

91
Any questions about anything

Similar presentations











 EXOCRINE PANCREASE Lecture Dr. Gamal Hamra Wednesday 01/12/1430 (18/11/2009)>")













![GI Endoscopy ~ BASIC ~ ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS EOSINOPHILIC ESOPHAGITIS IN CHILDREN [LECTURE] EOSINOPHILIC.](/20/5943603/big_thumb.jpg "GI Endoscopy ~ BASIC ~ ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS ESOPHAGUS - EOSINOPHILIC ESOPHAGITIS EOSINOPHILIC ESOPHAGITIS IN CHILDREN [LECTURE] EOSINOPHILIC.>")



