Download presentation
Presentation is loading. Please wait.

1
Using Recent Research to Improve the Cost-Effectiveness of VA Antipsychotic Formulary Policy Robert Rosenheck MD Michael Sernyak MD New England MIRECC Yale Medical School VA Connecticut Health Care System

2
VA Cooperative Study #455 Results(1) Patients assigned to olanzapine had: –less akathisia and –superior cognitive functioning (although not enough to affect quality of life); Olanzapine showed no advantage in: –Symptoms –Quality of life –Parkinsonian (EPS) side effects Olanzapine incurred greater weight gain and greater VA costs ($3,000 - $9,000/pt/year).
 Patients assigned to olanzapine had: –less akathisia and –superior cognitive functioning (although not enough to affect quality of life); Olanzapine showed no advantage in: –Symptoms –Quality of life –Parkinsonian (EPS) side effects Olanzapine incurred greater weight gain and greater VA costs ($3,000 - $9,000/pt/year).")
3
Cost Utility of the Latest Antipsychotic Drugs in Schizophrenia Study (CUtLASS)(S Lewis et al. 2005) RCT conducted in the UK for the NHS Health Tecnhnology Assessment Program Recruited: Aug 1999 – April 2002 Randomly assigned patients to “doctor’s choice” of any SGA other than clozpaine or FGA (n=227) No difference on symptoms, quality of life, side effects, health service use Conventional were more cost-effective
 RCT conducted in the UK for the NHS Health Tecnhnology Assessment Program Recruited: Aug 1999 – April 2002 Randomly assigned patients to doctor’s choice of any SGA other than clozpaine or FGA (n=227) No difference on symptoms, quality of life, side effects, health service use Conventional were more cost-effective.")
4
CATIE Cost Effectiveness Analysis (CEA) Study Design Comparison of Initiation Strategies Longer duration of treatment on olanzapine than risperidone or quetiapine: no difference from the FGA perphenazine Atypicals vs perphenazine: – Cost $3,600 – $6,000 more, –are no more effective on symptoms, quality of life, violence, employment, neurocognition, EPS, TD, akathesia –several incur greater weight gain
 Study Design Comparison of Initiation Strategies Longer duration of treatment on olanzapine than risperidone or quetiapine: no difference from the FGA perphenazine Atypicals vs perphenazine: – Cost $3,600 – $6,000 more, –are no more effective on symptoms, quality of life, violence, employment, neurocognition, EPS, TD, akathesia –several incur greater weight gain")
5
Antipsychotic Formulary Policy Revisited Virtual current policy: only use SGAs –10x greater cost ($230 million for VA/year) 400 MHICM teams or PCTs 3800 Employment specialists –No greater effectiveness –Greater risk of weight gain/metabolic syndrome/ diabetes –Less risk of EPS/TD than moderate/high dose haloperidol, but not intermediate or high potency FGAs (perphenazine, loxitane, thiothixene) Risperidone, least expensive SGA is off patent and will be less expensive.
 400 MHICM teams or PCTs 3800 Employment specialists –No greater effectiveness –Greater risk of weight gain/metabolic syndrome/ diabetes –Less risk of EPS/TD than moderate/high dose haloperidol, but not intermediate or high potency FGAs (perphenazine, loxitane, thiothixene) Risperidone, least expensive SGA is off patent and will be less expensive.")
6
Two Aspects of Formulary Policy What is the most cost-effective sequence of treatments? How do we create incentives to follow it? –No marketing for generics even if they are SGAs –Apprehension about restriction of any MH treatment if cost-saving is a potential motivation.

7
Preferred Sequence: Four groups of APS drugs Risperidone or intermediate potency FGA Clozapine (after 2 or 3 drug failures) Aripiprazole, ziprasidone or quetiapine Olanzapine: greatest weight gain Rosenheck et al., Schizophr Bull, 2008,34(2):375-380
 Aripiprazole, ziprasidone or quetiapine Olanzapine: greatest weight gain Rosenheck et al., Schizophr Bull, 2008,34(2):")
8
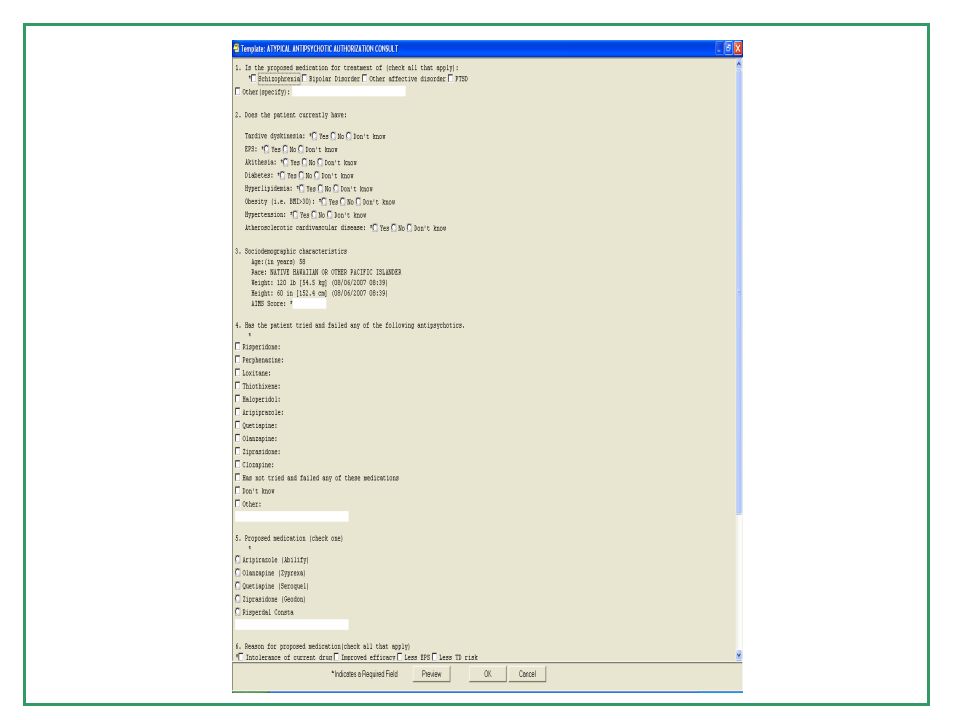
Incentives to Change Academic Detailing; Education/Information Monitor prescribing decision making with a structured form when NEW SGAs are prescribed –Very weak disincentive (time burden for the form) Feedback information in further academic detailing Caveat: Astra-Zeneca complained that we were not treating all SGAs equally as per VA agreement so we had to add risperidone to level 2
 Feedback information in further academic detailing Caveat: Astra-Zeneca complained that we were not treating all SGAs equally as per VA agreement so we had to add risperidone to level 2")
11
Monitoring Form Data (N=1,721): Diagnosis Schizophrenia or BP 44% –Schizophrenia18.1% –Bipolar disorder26.6% Sleep 18% Other Diagnoses 38% –Other affective24.0% –PTSD 23.4%
: Diagnosis Schizophrenia or BP 44% –Schizophrenia18.1% –Bipolar disorder26.6% Sleep 18% Other Diagnoses 38% –Other affective24.0% –PTSD 23.4%")
12
Monitoring Form Data (N=1,721): Reason for new medication Efficacy39.3% Sleep30.0% Patient preference27.0% Less EPS 12.5% Less TD risk 8.9% Less akathisia 4.7% Less sedation 5.8% Treatment of TD 0.8% Other20.7%
: Reason for new medication Efficacy39.3% Sleep30.0% Patient preference27.0% Less EPS 12.5% Less TD risk 8.9% Less akathisia 4.7% Less sedation 5.8% Treatment of TD 0.8% Other20.7%")
13
Monitoring Form Data (N=1,721): Health Status Age= 54.5 (±14) Weight=195 (±47) lbs. Ht = 5’9” BMI=28.8 (30=obese)
.")
14
Monitoring Form Data (N=1,721): Co-Morbidity –TD 4.3% –EPS 3.7% –Akathisia3.0% –Diabetes14.9% –Hyperlipidemia29.0% (DK-17.0%) –Obesity20.5% (DK-11.3%) –Hypertension34.0% (DK-10.2%) - ASCVD10.6% (DK-24.5%)
: Co-Morbidity –TD 4.3% –EPS 3.7% –Akathisia3.0% –Diabetes14.9% –Hyperlipidemia29.0% (DK-17.0%) –Obesity20.5% (DK-11.3%) –Hypertension34.0% (DK-10.2%) - ASCVD10.6% (DK-24.5%)")
15
Antipsychotics for Sleep (n=318 [18%]) Medication –Quetiapine 78.0% –Olanzapine 9.7% –Risperidone 8.8% Co-morbidities –HTN-38.4% –Hyperlipidemia-28.6% –Diabetes 13.5% –Obesity-16.7%
![Antipsychotics for Sleep (n=318 [18%]) Medication –Quetiapine 78.0% –Olanzapine 9.7% –Risperidone 8.8% Co-morbidities –HTN-38.4% –Hyperlipidemia-28.6% –Diabetes 13.5% –Obesity-16.7%](http://images.slideplayer.com/25/7923157/slides/slide_15.jpg "Antipsychotics for Sleep (n=318 [18%]) Medication –Quetiapine 78.0% –Olanzapine 9.7% –Risperidone 8.8% Co-morbidities –HTN-38.4% –Hyperlipidemia-28.6% –Diabetes 13.5% –Obesity-16.7%")
16
Previous drug trials Failed previous trial (efficacy) –Risperidone (5.0%) –Perphenazine (0.5%) –Haloperidol (2.4%) –Aripiprazole (1.4%) –Quetiapine (1.9%) –Ziprasidone(1.5%) –Clozapine (0.3%) –Olanzapine (1.7%) –Don’t know (26.6%) Failed previous trial (intolerability) –Risperidone (7.0%) –Perphenazine (1.8%) –Haloperidol (2.7%) –Aripiprazole (1.2%) –Quetiapine (3.3%) –Ziprasidone (1.6%) –Clozapine (0.5%) –Olanzapine (3.3%)
 –Risperidone (5.0%) –Perphenazine (0.5%) –Haloperidol (2.4%) –Aripiprazole (1.4%) –Quetiapine (1.9%) –Ziprasidone(1.5%) –Clozapine (0.3%) –Olanzapine (1.7%) –Don’t know (26.6%) Failed previous trial (intolerability) –Risperidone (7.0%) –Perphenazine (1.8%) –Haloperidol (2.7%) –Aripiprazole (1.2%) –Quetiapine (3.3%) –Ziprasidone (1.6%) –Clozapine (0.5%) –Olanzapine (3.3%)")
17
Additional Interventions Reviewed findings with groups –MDs –APRNs –MHSLs No detail work force

20
Conclusions SGAs are largely used for reasons without supporting evidence SGAs are largely used in patients who have medical conditions that these drug may worsen. MHSL managers have few tools to impact prescribing (?) Visit: http://vaww.nepec.mentalhealth.va.gov/AFP.htm
 Visit:")
21
Favors FGA Favors SGA Hypothesis of 5 point advantage for SGA excluded Difference in QLS scores Data from Table 3b Equivalence Estimate of difference in QLS after imputation of missing data, with 95% c.i. of difference ExpectedObserved 0 12 345 -2-3-4 -5 -66

22
Treatment (N=1,721) Treatment proposed: –Quetiapine49.4% –Olanzapine17.7% –Aripirazole13.2% –Risperidone*12.4% –Ziprasidone 5.2% –CONSTA 1.4% *Added in Summerof 2008
 Treatment proposed: –Quetiapine49.4% –Olanzapine17.7% –Aripirazole13.2% –Risperidone*12.4% –Ziprasidone 5.2% –CONSTA 1.4% *Added in Summerof 2008")
Similar presentations






; S Murphy; S McPherson & M Layton (co-Is) Start date: 9/13End date: 8/15 This research project.>")
 Anticholinergic.>")














