Download presentation
Presentation is loading. Please wait.

2
Controversies in managing neonatal infections David Isaacs Children’s Hospital at Westmead Sydney Australia

3
Controversies in managing neonatal infections Should I start antibiotics? Should I do a lumbar puncture first? Which antibiotics? Reluctance to stop antibiotics. How can I prevent fungal infections? How can I prevent coagulase negative staphylococcal infection?

5
Should I start antibiotics? Maternal risk factors in early sepsis Clinical examination Laboratory: blood count, acute phase reactants If in doubt, start them

6
Immediate Biopsy: alters treatment in 25% (Ecoli) 15-40% with meningitis have negative blood cultures Avoids confusion Delayed Respiratory compromise Trauma Cerebral herniation Rare Should I do a lumbar puncture first?
 15-40% with meningitis have negative blood cultures Avoids confusion Delayed Respiratory compromise Trauma Cerebral herniation Rare Should I do a lumbar puncture first")
7
LP and possible early sepsis Baby with RDS: 0.3% have meningitis 1500 LPs to find one meningitis Indications for Selective LP Clinical suspicion Risk factors (greatly prolonged rupture) Wiswell, 1995 169,000 babies: Selective LP would mean delay or missed diagnosis in 16 of 43 babies (37%)
 Wiswell, ,000 babies: Selective LP would mean delay or missed diagnosis in 16 of 43 babies (37%)")
8
LP and late sepsis Traditional data: up to 10% of babies with late sepsis have meningitis Recent data: 50-60% of late sepsis is with coagulase negative staphylococci Inclination: take blood culture, urine but not CSF (unless very sick) start antibiotics LP only if blood growing likely meningitis pathogen
 start antibiotics LP only if blood growing likely meningitis pathogen")
9
Which antibiotics? Narrowest spectrum possible: Penicillin and gentamicin Flucloxacillin and gentamicin Vancomycin and gentamicin Not third generation cephalosporins Not imipenem or carbapenem

12
Antibiotic abuse Paper to review: European country Thanksgiving 30 babies treated for Pseudomonas infection with ciprofloxacin Used ciprofloxacin because had run out of other options Only 4 had sepsis; 26 had endotracheal tube isolates Treated for 8 to 30 days

13
Antibiotics abuse (cont) Treating colonisation not sepsis Treating for long periods of time Using very broad spectrum (and expensive) antibiotics
 Treating colonisation not sepsis Treating for long periods of time Using very broad spectrum (and expensive) antibiotics")
16
Good antibiotic practise Use narrowest spectrum antibiotics possible Treat sepsis, not colonisation Stop antibiotics if cultures negative

17
Reasons given for continuing antibiotics Baby looked sick Acute phase reactants elevated Cultures might be false negatives Cultures unreliable Culture results not back

20
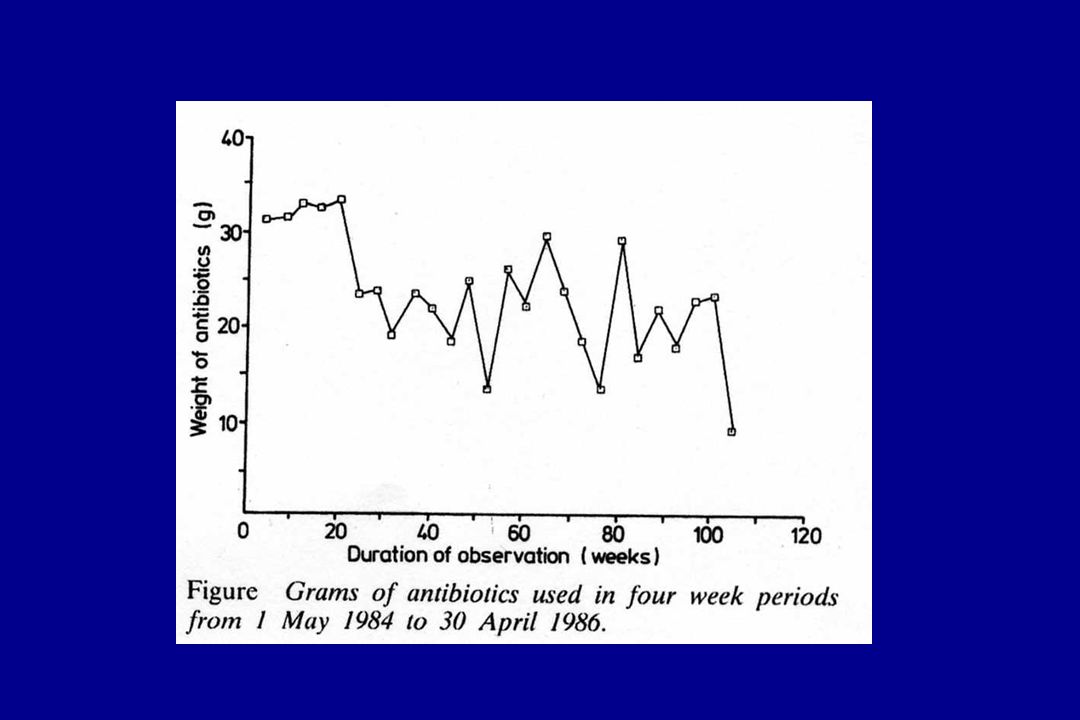
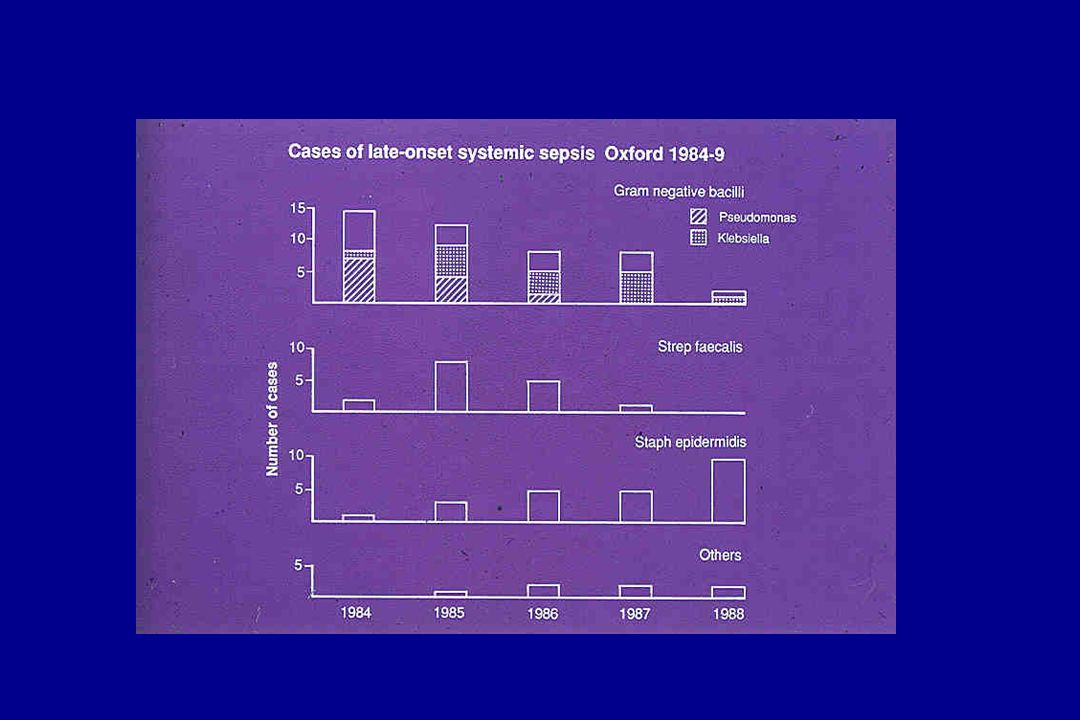
Antibiotic use, Oxford 1984-6 (ADC 1987: 62: 727-8) 19841986 Mean duration of antibiotics5.5 days3.6 days Weight of antibiotics (g)202.7122.1 % treated50%42% Late sepsis1216 No. after stopping antibiotics00

21
Reasons for stopping antibiotics Baby looked sick Courage, other causes Raised CRP Stop measuring it False negative cultures Rare in late sepsis Results not back Go to the lab and ask

23
How do I prevent fungal infections? Reduce duration of antibiotics Reduce duration of parenteral feeding Prophylactic antifungals

24
Fluconazole prophylaxis (Kaufman et al, NESM 2001; 345: 1660-6) 100 babies < 1000g BW over 30 month period 50 IV fluconazole for 6 weeks 50 placebo FluconazolePlacebo Colonisation11 30 Infection (urine, blood, CSF)0 10
 100 babies < 1000g BW over 30 month period 50 IV fluconazole for 6 weeks 50 placebo FluconazolePlacebo Colonisation11 30 Infection (urine, blood, CSF)0 10")
25
Prophylactic oral nystatin Preterm babies, birthweight <1250g Oral nystatin 1mL (100,000U) 8-hourly until one week after extubation. Outcome:colonisation(oropharynx, rectum) sepsis(blood, urine) (Sims M et al. Am J Perinatol 1988; 5:33-6)
 sepsis(blood, urine) (Sims M et al. Am J Perinatol 1988; 5:33-6).")
26
Prophylactic nystatin for low birthweight babies NystatinControl P (n = 33%)(n = 34) Colonised:4 (14%)15 (44%)<0.01 Systemic infection:2 (6%)11 (32%)<0.001 UTI:2 (6%)10 (30%)<0.01 Pneumonia:0 1 (died) Candidaemia:0 2 (Sims ME. 1988)
.")
27
How can we prevent coagulase negative staphylococcal sepsis? Change question: Should we try to prevent CoNS sepsis?

30
Coagulase negative staphylococcal neonatal infection (Australasia 1991 - 2000) 1,281 episodes 57% of late sepsis Meningitis 5 (0.4%) Mortality 4 (0.3%)
 1,281 episodes 57% of late sepsis Meningitis 5 (0.4%) Mortality 4 (0.3%)")
31
Conclusions Antibiotics are an extremely valuable resource Use them wisely Use them sparingly Prevention important Over-vigorous prevention not always wise

Similar presentations