Download presentation
Presentation is loading. Please wait.

1
RHP 12 Learning Collaborative Package Two (Topic One)
")
2
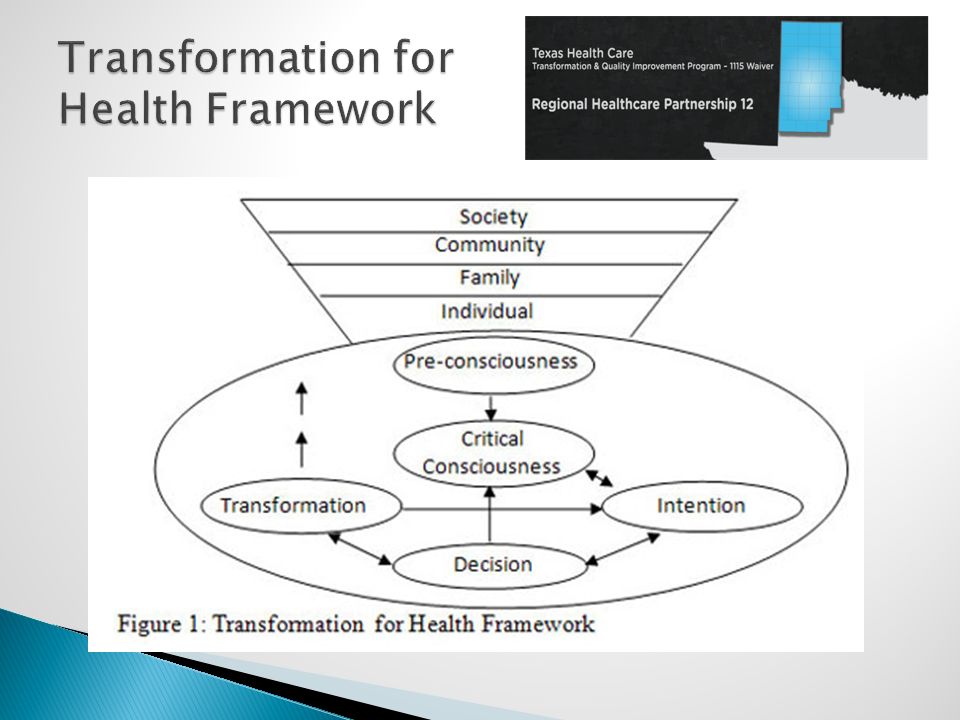
Participants will be able to describe the transformation for health model using the theories of Brazilian Philosopher Paulo Freire Participants will identify the stages and sequences of the transformation for health model Participants will describe the practical implementation of the model in a chronic disease management program. Participants will describe implementation of self efficacious behaviors Participants will demonstrate implementation of survey tools utilized in the transformation for health

3
Determinants of Health Status (from expert consensus; Shi; Blum) Health Status (100%) Genetics (10%) Medical Care (10%) Environment (40%) Behavior (40%) Physical Barriers Financial Education/Literacy Nutrition & Exercise Lifestyle choices Employment
 Health Status (100%) Genetics (10%) Medical Care (10%) Environment (40%) Behavior (40%) Physical Barriers Financial Education/Literacy Nutrition & Exercise Lifestyle choices Employment")
4
“An approach is needed to help patients change or adopt healthy behaviors – by themselves, not for them by others” (Paulo Freire)
")
7
IssueTraditional Patient EducationSelf-Management Education What is taught? Information and technical skills about the disease Skills on how to act on problems How are problems formulated? Problems reflect inadequate control of the disease The patient identifies problems he/she experiences that may or may not be related to the disease Relation of education to the disease Education is disease-specific and teaches information and technical skills related to the disease Education provides problem-solving skills that are relevant to the consequences of chronic conditions in general What is the theory underlying the education? Disease-specific knowledge creates behavior change, which in turn produces better clinical outcomes Greater patient confidence in his/her capacity to make life- improving changes (self-efficacy) yields better clinical outcomes What is the goal? Compliance with the behavior changes taught to the patient to improve clinical outcomes Increased self-efficacy to improve clinical outcomes Who is the educator?A health professionalA health professional, peer leader, or other patients, often in a group setting Constructs Cognition (Critical Consciousness) Intention (Self- Efficacy & Social Support) Decision (Barriers and Facilitators for Goal Setting) Transformation (Self Guided Evaluation & Goal Modification) Implementation
 yields better clinical outcomes What is the goal. Compliance with the behavior changes taught to the patient to improve clinical outcomes Increased self-efficacy to improve clinical outcomes Who is the educator A health professionalA health professional, peer leader, or other patients, often in a group setting Constructs Cognition (Critical Consciousness) Intention (Self- Efficacy & Social Support) Decision (Barriers and Facilitators for Goal Setting) Transformation (Self Guided Evaluation & Goal Modification) Implementation.")
8
“CONSCIENTIZATION” – awakening of critical consciousness, which is… A critical element of “LIBERATORY EDUCATION”, which then leads to… PRAXIS – action needed for transformational behavior

9
The first and most important step in the Transformational Process: facilitating the patient’s movement from Pre- consciousness to Critical Consciousness….

10
MAGIC CONSCIOUSNESS A person simply faces facts and attributes to them a superior power by which he is controlled and to which he must submit – characterized by fatalism. Que sera, sera NAÏVE CONSCIOUSNESS The person sees cause and effect as an unchanging established fact which can be deceiving – a person with naïve consciousness considers himself superior to facts, in control of facts, and thus free to understand them as he pleases. CRITICAL CONSCIOUSNESS A person who has reached the critical consciousness thinks of things and facts as they are objectively in reality; it is integrated with reality. Critical understanding leads to critical action.

11
THE NATURE OF HEALTH CARE RECEIVER Limited knowledge – naïve consciousness Different competencies and skills in self-care and care of others Adherence skills to comply with treatment plan varies along a range or continuum Self-defeating and dysfunctional life styles may be present driven by individual and family forces Limited internal and external resources Limited knowledge of internal and external resources

12
THE NATURE OF HEALTH CARE PROVIDER Specialized knowledge – expertise Plenty of experience, frequently of a technical nature Clinical skills vary along a range or extent Level of compassion for others vary along a range or extent Works within a context of limited time and resources to support task achievement Works within a practice setting that frequently may not be particularly supportive or compassionate Applicable community resources are fragmented and/or unknown

13
Creating an environment where patients open up to you as a provider ◦ How do you do this? Find out what patient expects from you as a provider What patients needs? Get on the patient’s level – language barriers Find out what patient is willing to do Starts out with the very first encounter – phone, face-to-face Identify with the patient – start where the patient is, relationship-building

14
How do you do this when you do not speak the same language as the patient? How do you do this when the patient is hostile or uncooperative? How do you do this when the patient is in denial? Creating an environment where patients open up to you as a provider

15
Individual’s motivational system is awakened by critical consciousness Capacity for the transformative process is assessed Development of self- efficacy to begin changing lifestyles and behaviors

16
Actualization of decision to change Acceptance of responsibility Acceptance of consequences and outcomes

17
Direct involvement in the health care process Requires a great deal of critical awareness or awakening Requires relationship building

18
Implementation Motivational Interviewing Self-Efficacy Enhancement Identification of Social Support Promotion of Effective Use of Social Support Avoidance in Goal Setting: Identify Barriers and Facilitators Facilitation of Evaluation of Outcome Guidance in Modification of Goals if Outcomes Not Met

19
SELF-EFFICACY

21
Choice behavior Effort expenditure and persistence Thought patterns and emotional reactions Humans as producers rather than simply foretellers of behavior

22
Mastery experience Vicarious experience Social persuasion (including verbal persuasions) Physiological states
 Physiological states")
23
Self-Efficacy for Managing Chronic Disease 6-Item Scale Self-Efficacy for Diabetes Measure of Patient Adherence (MOS)
")
24
Behavoiral Outcomes Apprehension of realities and readiness to change Enhanced Self- efficacy for health behavior change Intention to Adapt Positive Changes Effective use of social support in behavior change Realistic goal setting for behavior change Maintenance of Goals Continued Positive Behaviors

25
PROCHESKA & DICLEMENTE

26
permanent exit maintenance resumed use pre-contemplation contemplation preparation action preparation

27
Not thinking about change Thinking about change Preparing for change Taking action Maintaining change Return to old habits Change become permanent

28
How important is it to you to change this? 0…..1…..2…..3…..4…..5…..6…..7…..8…..9…..10 Not at all Extremely How confident are you that you can change this? 0…..1…..2…..3…..4…..5…..6…..7…..8…..9…..10 Not at all Extremely

30
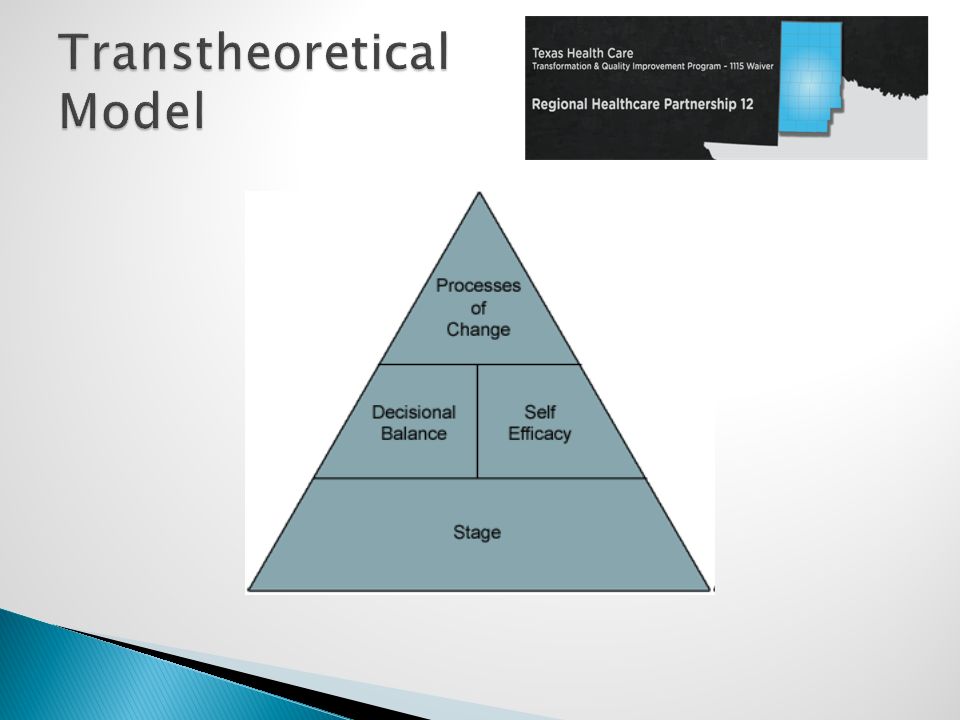
For individuals to progress, they need: A growing awareness that the advantages (the “Pros”) of changing outweigh the disadvantages (the “Cons”)—the TTM calls this decisional balance Confidence that they can make and maintain changes in situations that tempt them to return to their old, unhealthy behavior—the TTM calls this self-efficacy Strategies that can help them make and maintain change—the TTM calls these processes of change. The ten processes include

31
Consciousness-Raising Dramatic Relief Self-Reevaluation Environmental Reevaluation Social Liberation Self-Liberation Helping Relationships Counter-Conditioning Reinforcement Management Stimulus Control

32
ConstructsImplementation Behavioral Outcomes Targeted Goals Met

Similar presentations




,>")
















