Download presentation
Presentation is loading. Please wait.

1
Sakineh Hajebrahimi Associate Professor of urology Department Program Director of Female Urology Fellowship Tabriz University of Medical Sciences

2
Objectives the roles of pregnancy and delivery in pelvic-floor dysfunction pelvic-organ prolapse urinary incontinence fecal incontinence Management Conservative Surgical

3
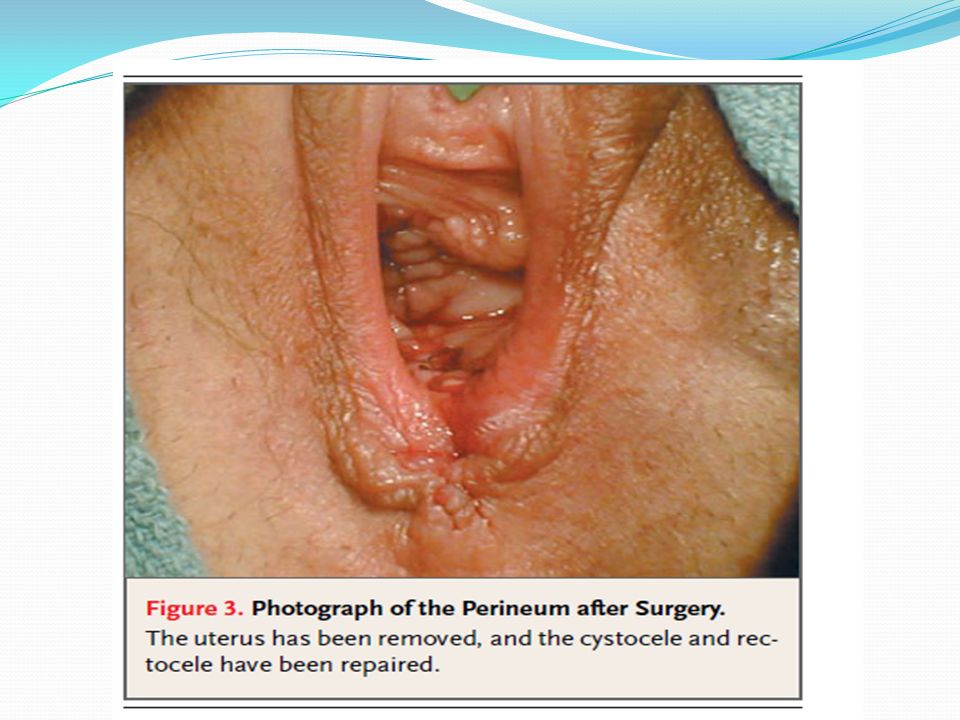
Case 1: A 46-Year-Old Woman with Pelvic-Floor Relaxation after a Second Vaginal Delivery The patient had been well until 10 months earlier, when she had experienced the rapid but otherwise uncomplicated vaginal delivery of her second child. A second degree laceration had occurred and had been repaired. At her six-week, postpartum examination, she had cystocele gIII and rectocele gII with gI-II utrine prolapse

4
Next Four Months During the next four months, the pelvic discomfort worsened, and the patient could see the cervix protruding at the introitus. She reported urinary frequency (12 or more times daily), urgency, leaking, a slow urinary stream, and a sense of incomplete bladder emptying
, urgency, leaking, a slow urinary stream, and a sense of incomplete bladder emptying.")
5
Urodynamics Study

6
Differential Diagnosis Epidemiology: between the ages of 15 and 97 years revealed that 46 %of women and 11 percent of men have pelvic-floor dysfunction A woman has an 11 % lifetime risk of undergoing surgery for incontinence, pelvic-organ prolapse, or both by 80 years of age.

7
Risk factors Vaginal delivery Large baby Prolonged 2nd stage of labor Forceps Multiparous

8
Risk factors Increased abdominal pressure Obesity Chronic constipation Chronic lung disease

9
Risk factors Altered nerve function or tissue strength Diabetes Neurologic diseases Aging Collagen disorders Hypoestrogenism Pelvic surgery

10
Anatomic cosidrations

11
Anatomy Basic Levator ani muscles Pubococcygeuas Puborectalis Iliococcygeus Viscerofascial layer Endopelvic fascia - attaches uterus and vagina to pelvic wall Parametria - cardinal and uterosacral ligaments Fascial defects Neuromuscular pathophysiology

12
The roles of pregnancy and delivery in pelvic-floor dysfunction How did this patient’s pregnancies contribute to her problems? whether elective delivery by cesarean section should be offered to minimize this risk?

13
Vaginal Delivery or C/S??? Pelvic-organ prolapse Several observational study No differents for new prolaps and modle of delivery (Level of Evidence C)
.")
14
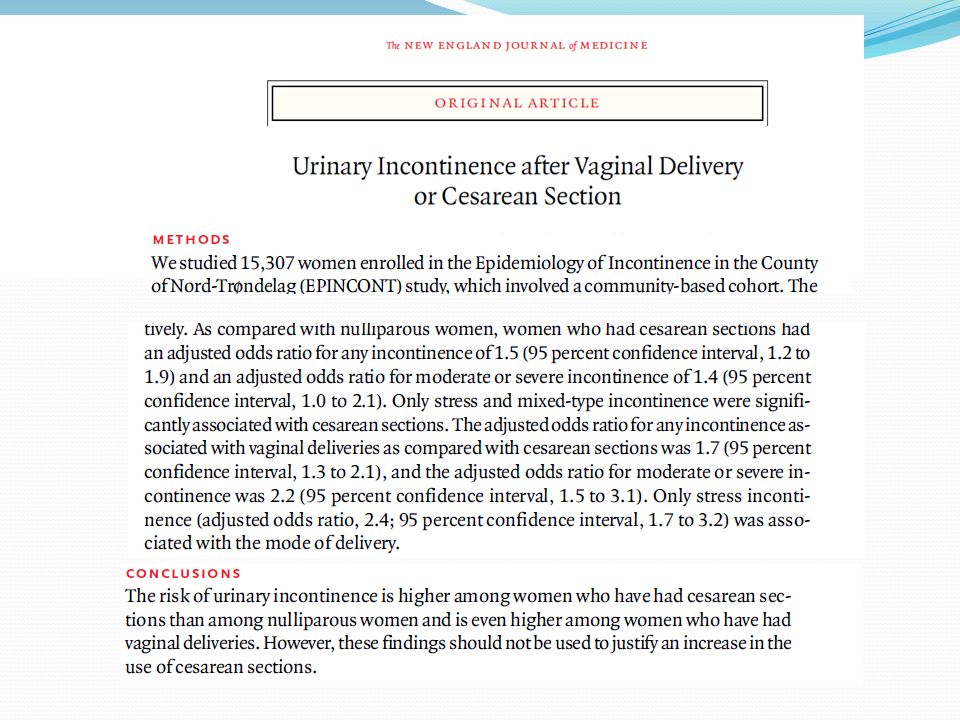
Vaginal Delivery or C/S??? Urinary Incontinence According to two studies,an urgent need to urinate occurred in 22 % and 62 % of pregnant women; 8 percent and 18 percent of pregnant women, respectively, had urge incontinence or urodynamic evidence of detrusor instability

15
Vaginal Delivery or C/S??? In a study of 305 primiparous patients, urinary incontinence appeared before, during, or after pregnancy in 4 %, 32 %, and 7 %, respectively. In a survey of 1505 women at three months post partum,the prevalence of incontinence was higher in those who had given birth vaginally rather than by cesarean section (24 percent vs. 5.2 percent

17
This highly controversial proposal is supported by a single trial of planned cesarean delivery versus planned vaginal delivery in cases of breech presentation, which showed a decrease in the rate of stress incontinence in the cesarean delivery group at 3 months post partum (relative risk, 0.62; 95% confidence interval, 0.41 to 0.93) but no significant difference between the two groups at 2 years post partum.
 but no significant difference between the two groups at 2 years post partum.")
18
Vaginal Delivery or C/S??? Insufficient Evidences in Favored of any delivery model!!

19
Vaginal Delivery or C/S??? Fecal incontinence Vaginal delivery appears to be responsible for fecal incontinence, through a combination of compression and stretch injury to the pudendal nerve and disruption of the anal sphincter.

20
Management OUTCOME

21
Note: A clinician might well be prepared to try a Antibiotics in a woman in whom there was an 80% chance her symptoms were due to cystitis, but the urologist would want to be close of 100% Adenocacinoma before starting Radical prostatectomy.

22
What are “tests” used for? Log of reasons by several docs: Diagnosis – most common but also Monitoring – has it changed? Prognosis – risk/stage within Dx Treatment planning, e.g., location Stalling for time!

23
Evaluation

24
Simple Complex (Office tests)(Urodynamics) Urinalysis Uroflowmetry Urine cultureCystometry Urinary diary Urethral function tests Pad test Ultrasound Videocystometry Ambulatory urodynamics Urinary Incontinence Investigation
(Urodynamics) Urinalysis Uroflowmetry Urine cultureCystometry Urinary diary Urethral function tests Pad test Ultrasound Videocystometry Ambulatory urodynamics Urinary Incontinence Investigation")
25
Normal flow trace Flowmeter Stress Urinary Incontinence Investigations - Uroflowmetry

26
UDS

27
Lifestyle interventions Weight loss Cessation of smoking Avoidance of heavy exercise / straining Effective management of constipation Pregnancy and childbirth Antenatal pelvic floor exercises Active management of labour Role of elective caesarean section? Urinary Incontinence Treatment: Primary Prevention

28
Urinary Incontinence - Management Incontinence on physical activity General assessment Physical examination: abdominal, pelvic, neurological ? Oestrogen status - if atrophic, treat as necessary Assess quality of life and desire for treatment Frequency volume chart Urinalysis ± urine culture – if infected, treat and reassess Assess post-void residual volume (by catheter or ultrasound) Assess for pelvic organ mobility / prolapse Consider imaging of the UT Urodynamics Lifestyle interventions ± Pelvic floor muscle training If initial therapy fails, consider Stress incontinence surgery / correct prolapse surgically HISTORY CLINICAL ASSESSMENT TREATMENT
 Assess for pelvic organ mobility / prolapse Consider imaging of the UT Urodynamics Lifestyle interventions ± Pelvic floor muscle training If initial therapy fails, consider Stress incontinence surgery / correct prolapse surgically HISTORY CLINICAL ASSESSMENT TREATMENT.")
29
Medications Duloxetine hydrochloride, a serotonin-reuptake Inhibitor A recent meta-analysis of randomized trials concluded that duloxetine significantly decreased the frequency of episodes of stress incontinence and improved the quality of life; adverse events, primarily nausea, were common but generally minor. Anti muscarinics for urge

30
Alpha agonists, such as clonidine, have been used empirically for the treatment of stress incontinence, but this use is not supported by rigorous studies, and efficacy in clinical practice is limited.

31
Postmenopausal estrogen treatment was previously believed to decrease the symptoms of stress incontinence. However, data from the Heart and Estrogen/Progestin Replacement Study showed a significantly higher risk of stress and urge incontinence among women randomly assigned to receive estrogen alone or estrogen and progesterone than among those assigned to receive placebo. Given these results, the initiation of hormone therapy for treatment of stress incontinence is not indicated.

32
Devices

33
A randomized, controlled trial comparing the use of super tampons and the use of pessaries to the use of no device in women who were incontinent while exercising found that the tampons and pessaries were similarly effective in reducing the frequency of stress Incontinence.

34
Surgery A Burch Colposuspension C Tension-free Vaginal Tape B Fascial Sling

36
Suprapubic Approach

37
“Mini – Sling” TVT SECUR System

38
Obturator Approach Transobturator tape (TOT)
")
39
Pelvic organ prolapse

40
Prolapse Surgery Never remove the vaginal mucosa Ethics and patient safety

42
Areas of Uncertainty Definition of Cure Reported cure rates associated with surgical treatment of stress incontinence by means of Burch colposuspension, suburethral sling, tension-free vaginal tape, or transobturator tape range widely, from 30% to 100%. This wide variation relates in part to the use of varying definitions of cure

43
Prevention Given the observational data indicating increased rates of stress incontinence among women who have undergone vaginal delivery as compared with cesarean delivery, cesarean delivery has been proposed as a strategy to prevent stress incontinence!!!!!!

44
New Surgical Procedures Many midurethral slings and related devices have been approved for use by the Food and Drug Administration (FDA). However, these approvals have involved the FDA’s 510(k), or premarket-notification,process that does not require proof of safety and efficacy of the new device but simply requires evidence that it is similar to one that has already been approved
, or premarket-notification,process that does not require proof of safety and efficacy of the new device but simply requires evidence that it is similar to one that has already been approved.")
45
The potential risks associated with this process are evidenced by the experience with the ProteGen sling, which was widely implanted in women before clinical trials were conducted Until peer-reviewed comparative data are available, caution is warranted in the adoption of new devices, and patients should be informed that the data available to guide the use of many new techniques are limited

46
Conlusion I would with my patient discuss surgical treatment as an alternative to behavioral or device therapies. I would explain that surgical treatment would probably result in improved quality of life and sexual function and would be expected to decrease considerably, but not completely eliminate, all symptoms of incontinence. No preventive prolapse surgery

47
Thank you

Similar presentations













 is a condition in which a woman's uterus (womb) sags or slips out of its normal position. The uterus.>")






