Download presentation
Presentation is loading. Please wait.

1
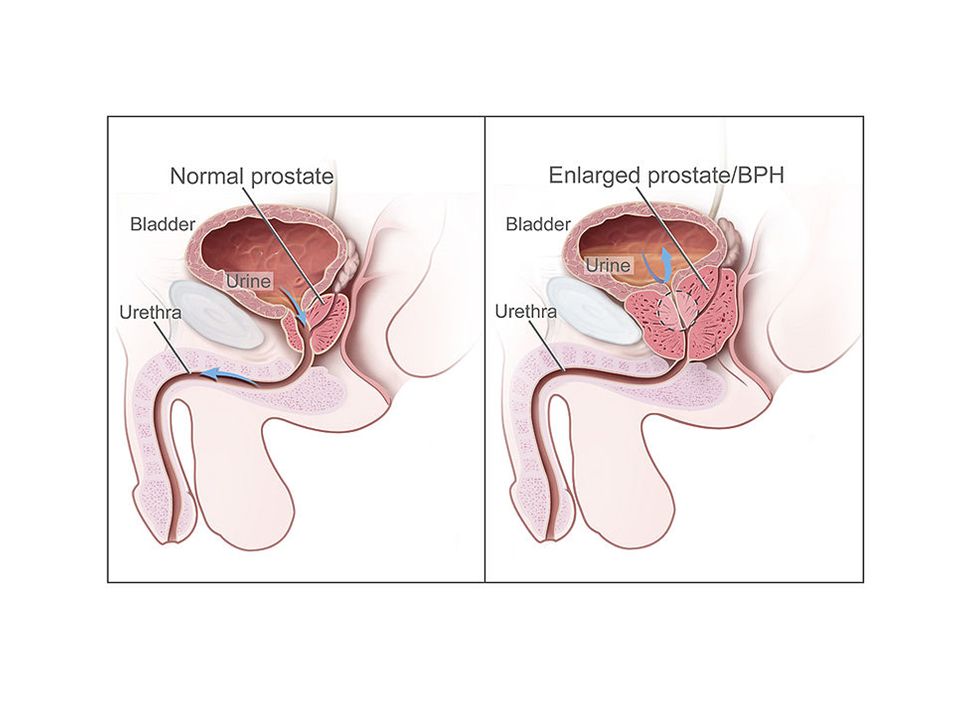
BPH

2
Etiology Most common benign tumor in men (Age related)
Multifactorial and endocrine controlled BPH is under endocrine control (+) correlation between levels of free testosterone and estrogen and the volume of BPH No studies to date has demonstrated eleveated estrogen receptor levels in human BPH
 correlation between levels of free testosterone and estrogen and the volume of BPH. No studies to date has demonstrated eleveated estrogen receptor levels in human BPH.")
4
Pathology BPH develops in transition zone.
Increase in cell number – Microscopic examination reveals a nodular growth pattern that is composed of varying amounts of stroma and epithelium. Stroma is composed of collagen and smooth muscle As BPH nodules in the transition zone enlarge, they compress the outer zones of the prostate, resulting in formation of so called surgical capsule

5
This boundary seperates the transition zone from the peripheral zone and serves as a cleaveage plane for open enucleation of prostate during open simple prostatectomies

6
Pathophysiology As prostatic enlargement occurs, mechanical obstruction may result from intrusion into the lumen. The surrounding capsule prevents it from radially expanding leading into urethral compression. The bladder wall becomes thickened, trabeculated, and irritable when it is forced to hypertrophy and increase its own contractile force

7
This increased sensitivity (detrusor instability), even with small volumes of urine in the bladder, is believed to contribute to urinary frequency and LUTS. The bladder may gradually weaken and lose the ability to empty completely, leading to increased residual urine volume and, possibly, acute or chronic urinary retention.

8
Testosterone (T) diffuses into the prostate epithelial and stromal cell. T can interact directly with the androgen (steroid) receptors bound to the promoter region of androgen-regulated genes. In the stromal cell, a majority of T is converted into dihydrotestosterone (DHT)—a much more potent androgen, which can act in an autocrine manner in the stromal cell or in a paracrine manner by diffusing into epithelial cells in close proximity. DHT produced peripherally, primarily in the skin and liver, can diffuse into the prostate from the circulation and act in a true endocrine manner. In some cases, the basal cell in the prostate may serve as a DHT production site, similar to the stromal cell.1
 receptors bound to the promoter region of androgen-regulated genes. In the stromal cell, a majority of T is converted into dihydrotestosterone (DHT)—a much more potent androgen, which can act in an autocrine manner in the stromal cell or in a paracrine manner by diffusing into epithelial cells in close proximity. DHT produced peripherally, primarily in the skin and liver, can diffuse into the prostate from the circulation and act in a true endocrine manner. In some cases, the basal cell in the prostate may serve as a DHT production site, similar to the stromal cell.1.")
9
Signs and Symptoms Urinary frequency Urinary urgency Hesitancy Incomplete bladder emptying Straining Decreased force of stream Dribbling – loss of small amounts of

10
Prostate Specific Antigen (PSA)
Laboratory Work up Urinalysis Dipstick methods and or centrifuged sediments Check for the presence of blood, WBC, bacteria, CHON and Glucose Urine Culture Useful to exclude infectious causes of irritative voiding Usually performed if the initial urinalysis findings indicate and abnormality Prostate Specific Antigen (PSA) Men at risk for BPH are also at risk for prostate cancer and should be screened accordingly Men with larger prostates may have slightly higher PSA levels
 Men at risk for BPH are also at risk for prostate cancer and should be screened accordingly. Men with larger prostates may have slightly higher PSA levels.")
11
Imaging Studies Ultrasound (Abdominal, renal, transrectal)
Intravenous Urography Determines bladder and prostate size and the degree of hydronephrosis (if any) It is not indicated for initial evaluation of uncomplicated LUTS TRUS In pateients with elevated PSA levels, TRUS guided biopsy may be beneficial Imaging of upper tracts is indicated in patients who present with (+) hematuria, history of urolithiasis, elevated crea, High PVR or history of upper UTI
 It is not indicated for initial evaluation of uncomplicated LUTS. TRUS. In pateients with elevated PSA levels, TRUS guided biopsy may be beneficial. Imaging of upper tracts is indicated in patients who present with (+) hematuria, history of urolithiasis, elevated crea, High PVR or history of upper UTI.")
12
Cystoscopy The procedure involves inserting a tube into the urethra through the opening at the end of the penis. It allows the doctor to visually examine the complete length of the urethra and the bladder for polyps, strictures (narrowing), abnormal growths, and other problems.
, abnormal growths, and other problems.")
13
Post void residual urine
Additional Tests Flow Rate Flow rate is useful in the initial assessment and to help determine response to treatment Post void residual urine Value after the patient voids in order to gauge the severity of bladder decompensation High PVR (350mL) may indicate bladder dysfunction and may predit a negative response to treatment Pressure Flow studies Invasive – findings invaluable for evaluating bladder outlet obstruction Bladder outlet obstruction is characterized by high intravesical voiding pressures (>60 cm water)
 may indicate bladder dysfunction and may predit a negative response to treatment. Pressure Flow studies. Invasive – findings invaluable for evaluating bladder outlet obstruction. Bladder outlet obstruction is characterized by high intravesical voiding pressures (>60 cm water)")
14
Differential Diagnosis
Bladder Cancer Bladder Stones Bladder Trauma Urethral Strictures Chronic Pelvic Pain Urinary Tract Infection,Males Interstitial Cystitis Neurogenic Bladder Prostatitis, Bacteria

15
5 alpha reductase inhibitors like Finasteride and Dutaseride are another treatment option.
They inhibit 5alpha reductase which inhibits production of DHT which is responsible for enlarging the prostate Side effects include decreased libido and ejaculatory or erectile dysfunction

16
Treatment The two main medications for management of BPH are alpha blockers and 5α-reductase inhibitors. Alpha blockers (technically α1-adrenergic receptor antagonists). Alpha blockers used for BPH include doxazosin,terazosin alfuzosin tamsulosin and silodosin. Alpha blockers relax smooth muscle in the prostate and the bladder neck, thus decreasing the blockage of urine flow. Common side effects of alpha blockers include orthostatic hypotension, ejaculation changes, nasal congestion, and asthenia.
. Alpha blockers used for BPH include doxazosin,terazosin alfuzosin tamsulosin and silodosin. Alpha blockers relax smooth muscle in the prostate and the bladder neck, thus decreasing the blockage of urine flow. Common side effects of alpha blockers include orthostatic hypotension, ejaculation changes, nasal congestion, and asthenia.")
17
Antimuscarinics shuch as Tolterodine can also be used especially with combination with alpha blockers. They act by decreasing acetylcholine effects on the smooth muscle wall of the bladder. This results in helping and controlling the symptoms of an overactive bladder

Similar presentations














 in men Kamal Patel GPST2.>")




 Jeannette Y. Lee, Ph.D. University of Alabama at Birmingham.>")