Download presentation
Presentation is loading. Please wait.

4
Projected number of osteoporotic hip fractures worldwide Projected to reach 3.250 million in Asia by 2050 Adapted from Cooper C et al, Osteoporosis Int, 1992;2:285-289 Estimated no of hip fractures: (1000s) 19502050 600 3250 19502050 668 400 19502050 742 378 19502050 100 629 Total number of hip fractures: 1950 = 1.66 million 2050 = 6.26 million
 Total number of hip fractures: 1950 = 1.66 million 2050 = 6.26 million")
7
Health care provider › Health Care System › Private versus public Doctors/Paramedics › Physician/Surgeons/Nurses/Rehabilitation Pharmaceutical companies › Cost › Supportive programs

8
Media Public Patients › Family and carers

9
A Still Neglected Disease › Ischemic heart disease › Diabetes mellitus › Cerebro-vascular disease › AIDS › ?????? OSTEOPOROSIS

10
Public health program does not include osteoporosis Low priority Neglect the concept on skeletal health for all age groups Lack of driving force and support

11
› Raising awareness about osteoporosis as a serious and debilitating disease › Increasing the priority of osteoporosis at national health policy planning › Urgently considering osteoporosis on the list of chronic, disabling diseases › Define essential care levels at a national level › Define future strategies, projects and plan to fight osteoporosis

12
› To reduce the incidence of osteoporosis related fractures by promoting safe home environment for elderly › Creating a national osteoporosis fracture database › Considering subsidy for all proven therapies before fracture for individuals at high risk

13
Programs on › Prevention › Identification of high risk individuals › Early diagnosis › Early and appropriate treatment intervention › Prevention of fall › Rehabilitation program for patients with fracture

14
Disease awareness Priority Pro-active › Physician treating patients for other medical conditions are more proactive in identifying underlying osteoporosis High risk groups › To assess fracture risks

15
Diagnosis › To initiate and suggest diagnostic measurement (DXA) to patients Combined approach (Surgeon & Physician) › Education Pharmacological intervention › to offer appropriate treatment if indicated › to monitor treatment
 to patients Combined approach (Surgeon & Physician) › Education Pharmacological intervention › to offer appropriate treatment if indicated › to monitor treatment")
16
45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90-94 40-44 95-99 45-4950-5455-5960-6465-6970-7475-7980-8485-8990-9440-44 Osteoporosis Self-assessment Tool for Asia (OSTA) Weight (kg) Age (yr) LOW RISK HIGH RISK measure BMD & treat AT RISK measure BMD History of prior non-violent fracture: consider BMD measurement and treatment
 Weight (kg) Age (yr) LOW RISK HIGH RISK measure BMD & treat AT RISK measure BMD History of prior non-violent fracture: consider BMD measurement and treatment")
17
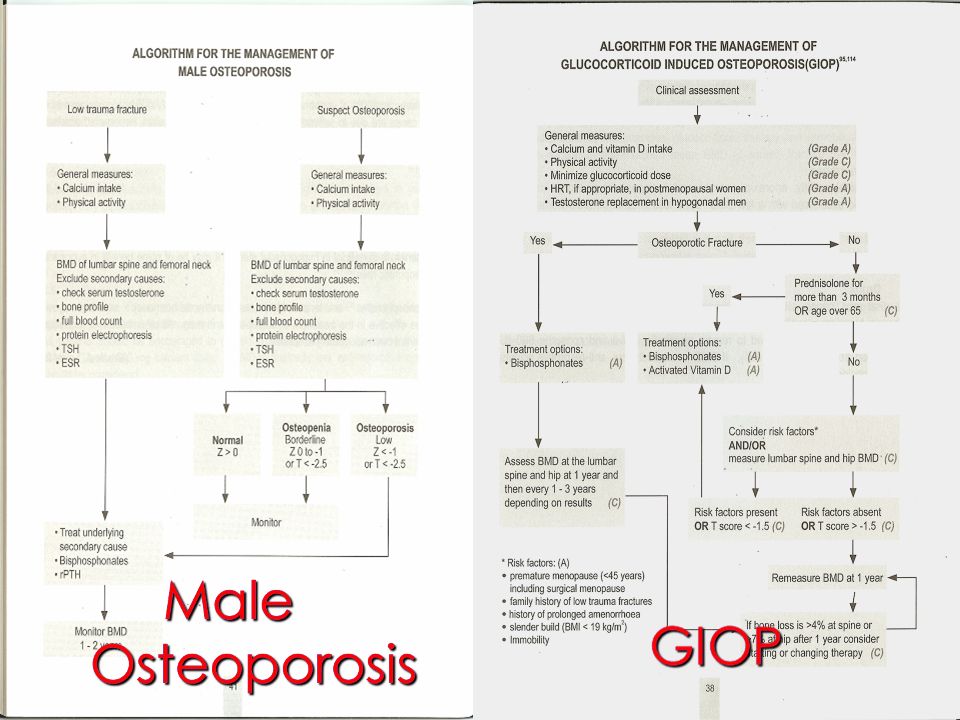
Assist decision making Assist selection of appropriate treatment Algorithm

21
Operate and send home!

22
Post-operative care Post-operative care Ambulation and weight bearing

23
1162 women, all greater than 65 year of age and treated for distal radial fractures, coming from 22 states throughout the United States Only 2.8% were sent for bone density testing to evaluate and document the presence of osteoporosis Only 22.9% of the women with fractures received any subsequent anti-osteoporosis medical treatment

24
227 postmenopausal women were admitted with a low-impact fracture (hip, spine, wrist, or humerus) to a hospital in Minnesota, osteoporosis was considered in only 26%. Within 12 months of discharge, only 10% had undergone BMD testing and only 26% were prescribed osteoporosis treatment.

25
Only 5% of 343 postmenopausal women admitted with a minimal trauma forearm fracture underwent bone density measurement in the subsequent 12 months. Only 18% were administered any intervention during the year after fracture.

26
Elderly men with fragility fractures were virtually ignored (1, 2) even though it is known that men have a higher mortality rate than women in acute care after hip fracture. 1. Juby AG, De Geus-Wenceslau CM 2002 Evaluation of osteoporosis treatment in seniors after hip fracture. Osteoporos Int 13:205–210 2. Kiebzak GM, Beinart GA, Perser K, Ambrose CG, Siff SJ, Heggeness MH 2002 Undertreatment of osteoporosis in men with hip fracture. Arch Intern Med 162:2217–2222

27
Osteoporosis was also less likely to be sought in elderly patients*, even though anti-resorptive therapy is known to reduce fracture risk in the very oldest patients** ***. *** Colon-Emeric CS, Sloane R, Hawkes WG, Magaziner J, Zimmerman SI, Pieper CF, Lyles KW 2000 The risk of subsequent fractures in communitydwelling men and male veterans with hip fracture. Am J Med 109:324–326 ** Klotzbuecher CM, Ross PD, Landsman PB, Abbott III TA, Berger M 2000 Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 15:721–739 * Onder G, Pedone C, Gambassi G, Landi F, Cesari M, Bernabei R, Investigators of the GIFA Study 2001 Treatment of osteoporosis among older adults discharged from hospital in Italy. Eur J Clin Pharmacol 57:599–604

28
NO TREATMENT!!!!!! Patient Factors › Osteoporosis? › Default follow up Physician/Surgeon Factors › Attitude – Not interested, Who cares?, So What? › Awareness › Busy practice › Lack of physician-surgeon collaboration

29
Orthopedic surgeons treating low trauma fractures in postmenopausal women and older men need to take the next step to initiate an evaluation for osteoporosis themselves or to refer the patient back to the primary care physician or to a medical specialist with a specific request for evaluation and appropriate treatment.

30
Physiotherapists, nurses etc should identify patients with clinical features of fracture and refer to physicians/surgeon for further evaluation to educate and encourage patients and family to maintain physical activities to minimize fall to tailor rehabilitation program for individual patient to maximize their functional recovery

31
Public health problem Silent disease Early diagnosis for high risk individuals The need for long term therapy Reduction of fracture risk

32
Acceptable › Understand the need for long term treatment Available › Different classes of therapeutic agents Accessible › Both in urban and rural areas Affordable › Cost for long term treatment

33
Stimulators of bone formation Fluoride) (Fluoride) Parathyroid hormone Mixed mechanism of action Vitamin D and metabolites Strontium ranelate For All Patients Calcium and vitamin D Inhibitors of bone resorption Bisphosphonates –Alendronate –Risedronate –Ibandronate –Zoledronate Calcitonin Estrogen ± progestin (SERMs) (SERMs) –Raloxifene
 (Fluoride) Parathyroid hormone Mixed mechanism of action Vitamin D and metabolites Strontium ranelate For All Patients Calcium and vitamin D Inhibitors of bone resorption Bisphosphonates –Alendronate –Risedronate –Ibandronate –Zoledronate Calcitonin Estrogen ± progestin (SERMs) (SERMs) –Raloxifene")
34
Daily › Alendronate 10mg › Strontium ranelate 2gm › Raloxifene 60mg Weekly › Alendronate 70mg, Alendronate Plus 70 mg › Risedronate 35mg Monthly › Ibandronate Yearly › Zoledronate

35
Just like hypertension, diabetes mellitus and other medical conditions Why monitor? Improve adherence and compliance Translate into effective treatment outcome Reduction of fracture risks

36
Patients Show Poor Persistence Why Monitoring? NDC Health Study: Poor Persistence even with Weekly Prescriptions Ettinger M, et al. Arthritis Rheum. 2004;50(suppl):S513-S514. Abstract 1325. Data on file (Reference # 161-040), Hoffmann-La Roche Inc., Nutley, NJ 07110. A HIPAA-compliant, longitudinal patient database of prescriptions dispensed from ~25% of US retail pharmacies was used to assess discontinuation of bisphosphonates over a 12-month period in women aged ≥50 years.* * Primary usage in osteoporosis; however, data may include use in other indications.
:S513-S514. Abstract Data on file (Reference # ), Hoffmann-La Roche Inc., Nutley, NJ A HIPAA-compliant, longitudinal patient database of prescriptions dispensed from ~25% of US retail pharmacies was used to assess discontinuation of bisphosphonates over a 12-month period in women aged ≥50 years.* * Primary usage in osteoporosis; however, data may include use in other indications..")
37
Monitoring Improves Compliance The Impact of Monitoring on Adherence and Persistence Source: Clowes et al (2004) The Journal of Clinical Endocrinology & Metabolism 89(3):1117-1123 The Kaplan-Meier survival curves for cumulative adherence to therapy (75%) are shown for the monitored group (nurse-monitoring and marker- monitoring) compared to the no monitoring group. Monitoring increased cumulative adherence to therapy (75%) by 57% compared with no monitoring ( P 0.04). There was a trend for greater cumulative adherence to therapy in the nurse-monitoring and marker- monitoring groups ( P 0.05 and P 0.15) compared to usual cure.
 by 57% compared with no monitoring ( P 0.04). There was a trend for greater cumulative adherence to therapy in the nurse-monitoring and marker- monitoring groups ( P 0.05 and P 0.15) compared to usual cure..")
38
Monitoring Techniques › Acceptable › Available › Accessible › Affordable Clinical Radiological DXA scan Bone turnover markers

39
DXA › BMD changes with pharmacological agents only explain partially the reduction of fracture risk › Significant changes seen only after 1 ½ to 2 years of treatment

40
Bone turnover markers › As early as three months after treatment with anti-resorptive agents

41
Bone turnover markers › Limitations › Not readily available in Asian countries › More important role in clinical practice › Baseline, three months and nine months after treatment

44
Persatuan Kesedaran Osteoporosis Kuala Lumpur (Osteoporosis Awareness Society of Kuala Lumpur)
")
45
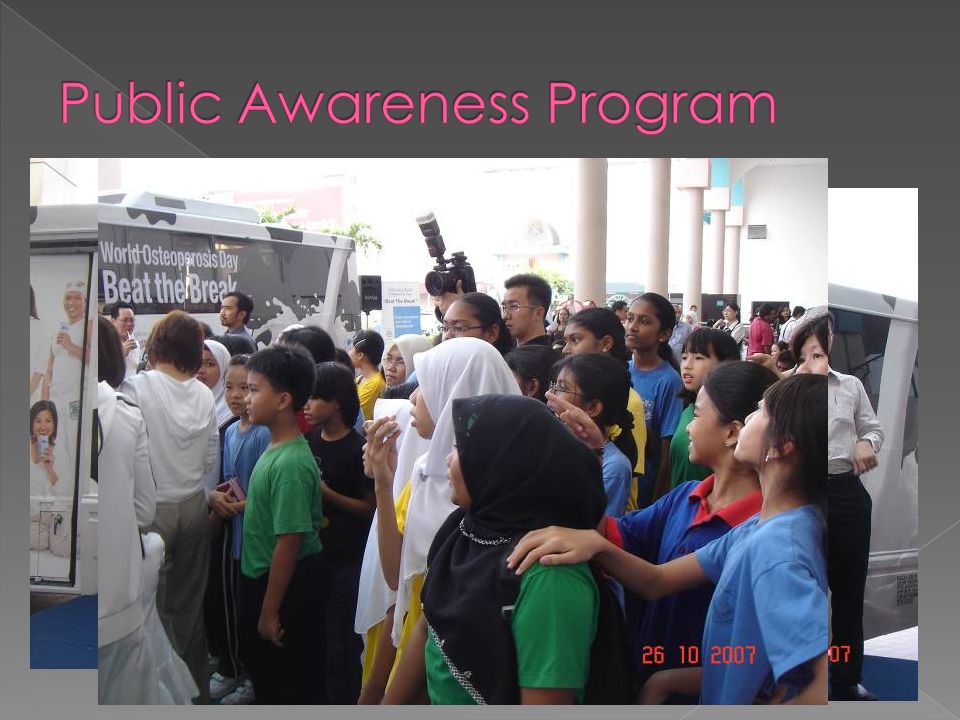
Promoting skeletal health in public throughout all age groups Public awareness on osteoporosis Identification of at risk group › Diagnosis › Treatment Patient support group › Patients with and without fractures › Carers

46
Patient and family should play the primary role in promoting treatment uptake Supervise patients the correct way of taking their medicines Ensure compliance and adherence Safe home environment

48
Health Care Providers Doctors/Paramedics Patients/Public

49
Thank You

Similar presentations




, Fellowship Diabetes/Endocrinology (AKUH), PG Dip Diab (UK) Consultant Endocrinologist.>")



>")












