Download presentation
Presentation is loading. Please wait.

1
Introduction to the Indian Health Service Thomas Sequist, MD MPH

2
Varying Population Estimates 2010 US Census/ IHS Enrollment Files

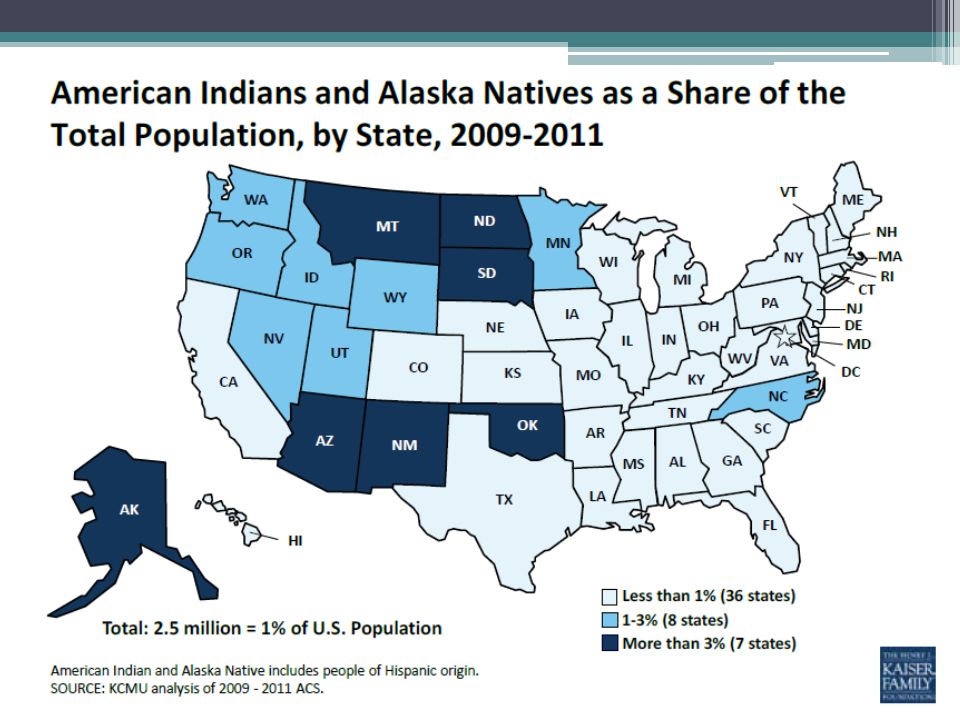
3
Population Distribution Office of Minority Health, 2010

5
Health Status of AI/AN Population

6
4 year shorter life expectancy IHS, Indian Health Disparities, www.ihs.gov Life Expectancy at Birth

7
Sequist et al, Health Affairs 2011 Major Contributors to Premature Death

8
US Census Bureau 2010 Health Insurance Coverage

9
The Indian Health Service

10
1.9 million people served 850 federally employed physicians 500 health centers 45 hospitals Indian Health Service

11
IHS Clinical Locations

12
Roubideaux, Y. N Engl J Med 2005 Kaiser Family Foundation, 2013

13
IHS Budget Process ▫Annual appropriation through House and Senate ▫Extensive tribal consultation ▫Budget justification ▫House and Senate approval

14
Contract Health Services ▫Many services not available within IHS or tribal facilities ▫Hospital services, specialty services, pharmacy, imaging ▫Rationing of health services Prioritize funding of medical cases that “threaten life or limb” Lack of priority on preventive services

15
Tribal Management of Funds ▫>50% of funds currently ▫Tribal sovereignty and local control ▫Ability to seek external grant funding ▫Ability to lobby on behalf of community There are limited rigorous data evaluating the impact on health care and outcomes

16
Quality of Care

17
Challenges to Quality Improvement Preventive services Chronic disease

18
The Burden of Diabetes CDC 2010

19
The Epidemic of Heart Disease CDC 2010

20
Preventive services Chronic disease Specialty services Challenges to Quality Improvement

21
Ability to Access Needed Services Were you able to obtain access to these services for your patients when necessary? Sequist, et al. JGIM 2010,, Bach et al. NEJM 2004

22
Access to Subspecialty Care Would you say that the complexity of patient conditions you are currently expected to provide care for is… Sequist, et al. JGIM 2010

23
Preventive services Chronic disease Cross Cultural Specialty services Challenges to Quality Improvement

24
Some Particular Challenges ▫> 500 tribes and Nations ▫28% of AI/AN speak a language other than English at home ▫IHS Physicians…. 10% report that cross-cultural barriers are common during encounters As many as 10% of patients challenging to communicate with due to language 12% report that professional translator available

25
Preventive services Chronic disease Cross Cultural Specialty services Social inequities Challenges to Quality Improvement

26
Socioeconomic Challenges BLS 2011; OMH 2010

27
Preventive services Chronic disease Cross Cultural Specialty services Social inequities Limited finances Challenges to Quality Improvement

28
Roubideaux, Y. N Engl J Med 2005 IHS is Generally Underfunded $4.3 billion (52% of need)
")
29
IHS Clinician Shortage IHS Workforce 2009

30
Preventive services Chronic disease Cross Cultural Specialty services Social inequities Geographic isolation Limited finances Challenges to Quality Improvement

31
Distribution of AI/AN Population 2010 US Census Bureau

32
New Mexico AI/AN Population Sequist et al, HSR 2006

33
The Importance of Geography

34
Geographic Isolation

35
Appropriate Care for Acute MI? AI/AN with acute myocardial infarction have… ▫Longest duration from symptom onset to arrival at the hospital ▫Increased risk of arriving to hospital without ambulance ▫Lower rates of cardiac catheterization, angioplasty, and coronary bypass surgery

36
Access To Renal Transplantation Sequist, et al Am J Kid Dis 2004

37
Snapshot of IHS Quality Sequist, et al. AJPH 2005

38
Diabetic Retinopathy Screening

39
Tele-Ophthalmology AI/AN have low rates of dilated eye exams Lack of access to providers Tele-ophthalmology program allows remote provision of care

40
Phoenix Indian Medical Center Wilson, Diabetes Care 2005

41
How Can Academic Centers Contribute? Development of physician leaders Provision of clinical expertise

42
Four Directions Summer Research Program Increase representation of Native Americans among physicians, scientists, and public health officials. www.fdsrp.org 1) Increase student motivation and confidence 2) Individualized mentoring 3) Social and professional networking 4) Continuous program evaluation
 Increase student motivation and confidence 2) Individualized mentoring 3) Social and professional networking 4) Continuous program evaluation.")
43
Barriers to Career Advancement Intrapersonal Perceived abilities Motivation Fear of isolation Structural Financial Mentoring Enrichment programs

44
Program Results Nearly 200 students over 21 years “How much did the program increase your motivation to pursue a career in medicine?” ▫82% report ‘extreme’ “Do you feel better prepared to apply to medical or graduate school after participating in the program?” ▫65% report ‘extreme’, 30% ‘significant’

45
Long Term Outcomes 100% of alumni would recommend program to a colleague 70% report an ‘extreme’ impact achieving their goals 63% enrolled in medical or graduate school

46
BWH Physician Volunteer Program Work with IHS clinical staff to expand ability to meet patients’ clinical needs To improve the health status of Native American communities www.brighamandwomens.org/ihs

47
Navajo Reservation 3x the size of Massachusetts with 300,000 members 25% unemployment 43% below federal poverty level 60% without regular telephone access 32% lack access to plumbing Shiprock Gallup CO UT NM AZ

48
Gallup and Shiprock Gallup: 99 bed facility, 120 physicians Shiprock: 60 bed facility, 75 physicians

49
Large Service Areas SHIPROCK GALLUP

50
Large Service Areas ALBUQUERQUE SHIPROCK GALLUP 230 miles

51
Large Service Areas ALBUQUERQUE SHIPROCK GALLUP 230 miles 140 miles

52
Challenges to Accessing Care Concept of “contract care” ▫Outside referrals ▫Fixed budget ▫Rationed according to emergent need Lack of specialty services ▫Intermittent (or no) availability Many conditions go untreated
 availability Many conditions go untreated")
53
Solutions to Accessing Care “Clearing” clinical consult backlog Increasing capacity of IHS physicians ▫Up to date practices ▫Expanding ability to provide specialty care Low volume, complex care ▫Stabilizing patients ▫BWH based experiences

54
Model of Volunteering Site Visit Teaching/ training Patient care Distance teaching Video conferencing Distance consulting Email Telephone BWH Shadowing IHS clinicians travel Site-specific needs assessment

55
Thank You!

Similar presentations


















 1.5d: Controlling Medical Expenses.>")
