Download presentation
Presentation is loading. Please wait.

1
Solving TASS: Maximizing Patient Safety in VA Operating Rooms Mary K. Daly, MD Chief of Ophthalmology VA Boston Healthcare System Associate Professor of Ophthalmology Boston University

2
What is TASS? Toxic Anterior Segment Syndrome Acute sterile inflammatory reaction following anterior segment surgery

3
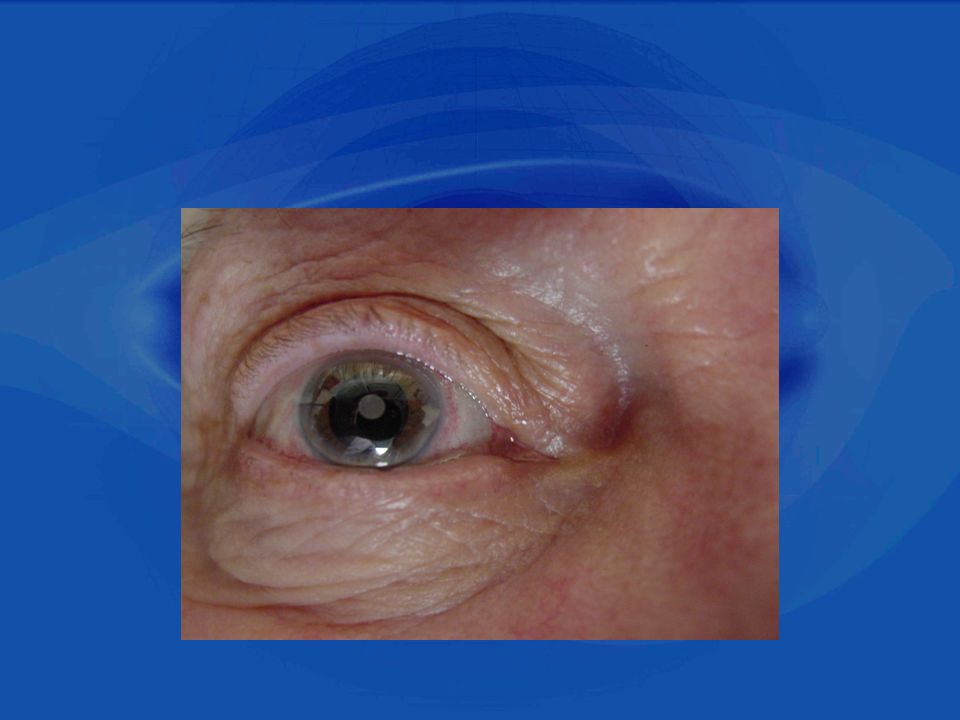
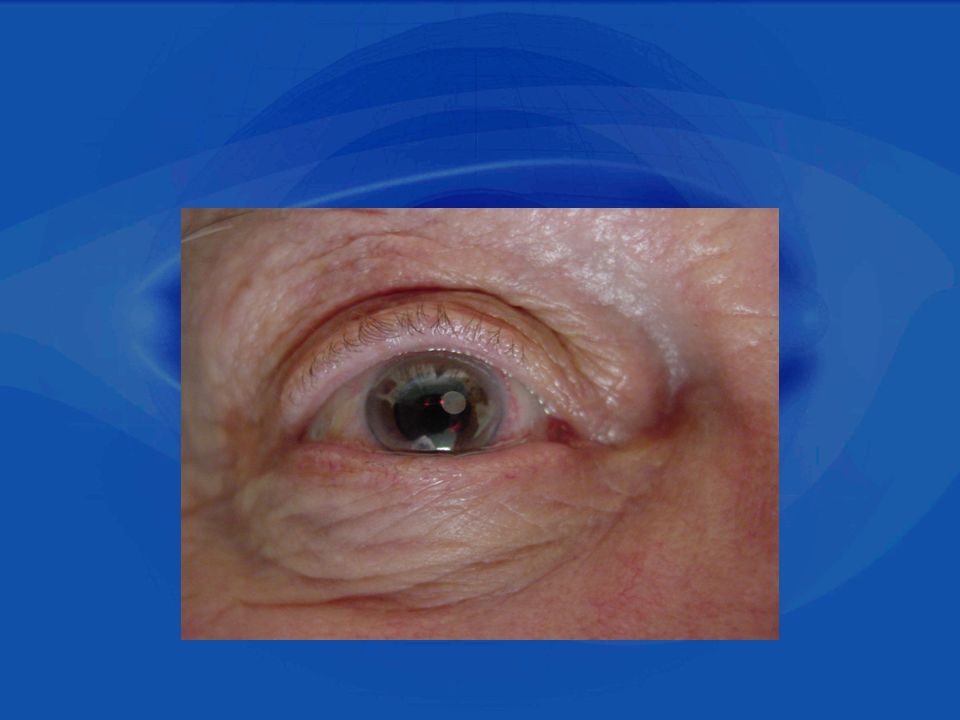
What is TASS? Toxic Anterior Segment Syndrome Clinical Findings: – limbus-to-limbus corneal edema secondary to toxic damage of endothelium –Aggressive AC reaction, fibrin, and hypopyon –Dilated, irregular pupil secondary to toxic damage to iris –Initial hypotony elevated IOP/glaucoma due to TM damage Photos courtesy of: Henry F. Edelhauser, PhD Ferst Professor of Ophthalmology & Director of Ophthalmic Research Emory University Atlanta, GA

4
Treatment Intense topical steroids Lasting sequelae corneal edema, glaucoma, devastating visual loss

5
How Extensive is the Problem Firm data on the incidence of TASS are lacking Tends to occur in clusters ranging from a few cases to up to 20 cases per cluster

6
How Extensive is the Problem 2006 North American Outbreak 2006 -- Major Outbreak throughout much of North America with >100 surgical centers reporting cases Formation of TASS Task Force chaired by Nick Mamalis and Henry Edelhauser and included representation from the ASCRS, AAO, ASORN, AORN, APIC, CDC, and FDA

7
How Extensive is the Problem 2006 North American Outbreak Extensive Analysis did not find a single factor but rather multiple potential factors, with most common offenders (courtesy of Dr. Henry Edelhauser) : –Inadequate cleaning and flushing of ophthalmic instruments and handpieces –Use of detergents –Shared ultrasonic water baths –Intraocular medications with preservatives Resulted in special report on recommended practices for cleaning and sterilizing intraocular surgical instruments to prevent TASS
 : –Inadequate cleaning and flushing of ophthalmic instruments and handpieces –Use of detergents –Shared ultrasonic water baths –Intraocular medications with preservatives Resulted in special report on recommended practices for cleaning and sterilizing intraocular surgical instruments to prevent TASS.")
8
Case Togus Maine VA –In 1865, as the Civil War was drawing to a close, President Lincoln signed an act establishing the National Asylum (later changed to Home) for Disabled Volunteer Soldiers. The Eastern Branch at Togus, Maine was the first of these homes and admitted the first Veteran in November 1866

9
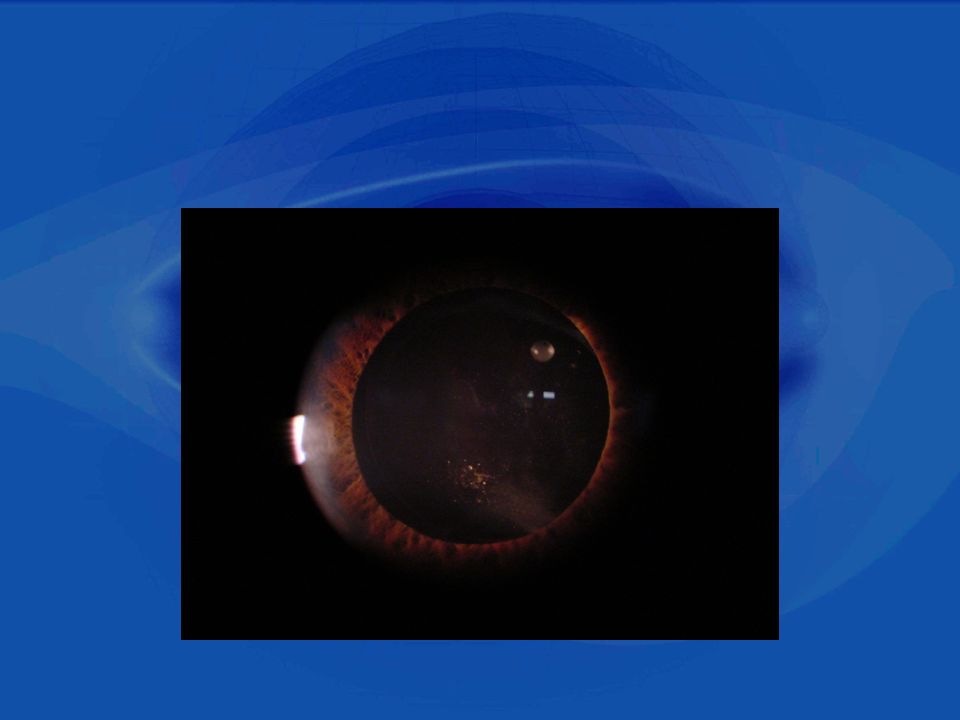
Case 85 year old male referred for: – persistent anterior uveitis –recurrent CME despite chronic topical Pred Forte, Acular, and two subtenons kenalog injections – ‘superior angle cyst’ All following uneventful phacoemulsification surgery more than 2 years prior

14
Continued topical pred forte and acular Took to OR for AC washout and removal of ‘globule’ Irrigated AC well with automated I/A Sent specimen to Prof Jamie McKnight The McKnight Lab, Dept of Physiology and Biophysics at BUSM

15
NMR Antibiotic ointment (ilotycin) dissolved in duturated benzene Benzene – d6 (99.95%) Ilotycin Ointment Unknown Specimen
 dissolved in duturated benzene Benzene – d6 (99.95%) Ilotycin Ointment Unknown Specimen")
16
VA Boston Intraocular ung/inflammation/CME referred to VA Boston One case of fibrin, pupillary membrane post-op day #1 routine PK for KC Several cases of ‘fiber’ noted intraop and/or post-op routine phaco

17
What’s the potential for TASS in VA System as a whole? Approximately 40,000 ophthalmology cases/year in the VA –Boston performs ~ 1000/year TASS Task Force lead by Dr. Edelhauser, Dr. Mamalis, Sue Clouser found 909 cases of TASS out of 50 114 cataract surgeries (reported from 77 questionnaires) Extrapolate to VA ~ potential for 725 cases in VA each year
 Extrapolate to VA ~ potential for 725 cases in VA each year.")
18
Preventative Steps Taken at VA Boston Investigated procedures from the operating room, to SPD, and back Interviewed nursing staff, residents, attendings, SPD and pharmacy staff Observed instrument handling Reviewed topical and intracameral medicines and solutions

19
Steps Taken at VA Boston Initial findings: preserved epinephrine in carts, sterile cloth towels in kits (fibers), reusable cannulas, ointment being used by some at end of cases, variable understanding of SOPs (precleaning and sterilization) amongst staff, unclear how long used trays were sitting around before being sterilized
, reusable cannulas, ointment being used by some at end of cases, variable understanding of SOPs (precleaning and sterilization) amongst staff, unclear how long used trays were sitting around before being sterilized")
20
Next Steps at VA Boston Reviewed all ASCRS/ASORN recommendations and modified policies and procedures accordingly

21
Next Steps Called the TASS Detective –Sue Clouser, RN MSN CRNO –Works with ASCRS –> 100 TASS investigations

22
TASS Detective Report Several different areas needing modification Recommendations specifically targeted: –Cleaning and flushing of ophthalmic instruments and handpieces –Use of detergents –Ultrasonic water baths

23
VA Boston Conclusions and Solutions to Prevent TASS Distributed ASCRS/ASORN Recommendations on the prevention of TASS Reviewed with staff and implemented the recommedations of TASS Detective, Sue Clouser Established continuing education program for OR, Clinic, Pharmacy, SPD staff –Joint educational lectures q6 months on policies, procedures, recognition of TASS Promoted open discussion, awareness, team effort

24
VA Boston Solutions to Prevent TASS Empowered every staff member to familiarize themselves with the OR processes and procedures including SPD Reiterated to everyone importance of double checking all solutions/meds for themselves to ensure correct concentrations and preservative-free

25
VA Boston Solutions to Prevent TASS Weekly Surgical Complications Conferences – with non-punitive reporting mechanisms and open, collegiate discussions and case-presentations –Formal written peer review done on every complication –Clearly define reportable findings Fibrin Hypopyon Severe corneal edema/edema inconsistent with case Pain, reduced vision, red eye inconsistent with case

26
Ophthalmic Surgical Outcomes Committee VA Boston is one of the five pilot sites in the OSOD Committee under direction of Mary Lawrence (Deputy Director of the Vision Center of Excellence) Tracking ophthalmic surgery data in order to establish a prospective outcome-based program to enhance the quality of cataract surgery across the VA and the country Instrumental in monitoring data and identifying and preventing potential outbreaks
 Tracking ophthalmic surgery data in order to establish a prospective outcome-based program to enhance the quality of cataract surgery across the VA and the country Instrumental in monitoring data and identifying and preventing potential outbreaks")
27
Important References *Focal Points, N. Mamalis, Module 10, 2009 (AAO) *Instrument Re-processing Product Questionnaire Survey (ASCRS) *Mammalis N, Edelhauser HF, Dawson DG, Chew J, LeBoyer RM, Werner L. Toxic anterior segment syndrome. J Cataract Refract Surg 2006;32:324.Mammalis N, Edelhauser HF, Dawson DG, Chew J, LeBoyer RM, Werner L. Toxic anterior segment syndrome. J Cataract Refract Surg 2006;32:324. *On-line www.tassforce.comwww.tassforce.com *ASCRS and ASORN Toxic anterior segment syndrome task force guidelines. Recommended practices for cleaning and sterilizing intraocular surgical instruments, June 15 2009, http://www.ascrs.org/TASS/upload/TASS_guidelines-CBC.pdfhttp://www.ascrs.org/TASS/upload/TASS_guidelines-CBC.pdf *Cohen AW, Oetting TA. Toxic Anterior Segment Syndrome (TASS): A System's Based View of a Day in the Life of a Canula. EyeRounds.org. May 7, 2008 [cited --insert today's date here -- ]; Available from: http://www.EyeRounds.org/cases/85-Toxic- Anterior-Segment-Syndrome-TASS-Systems-Based.htm.
 *Instrument Re-processing Product Questionnaire Survey (ASCRS) *Mammalis N, Edelhauser HF, Dawson DG, Chew J, LeBoyer RM, Werner L. Toxic anterior segment syndrome. J Cataract Refract Surg 2006;32:324.Mammalis N, Edelhauser HF, Dawson DG, Chew J, LeBoyer RM, Werner L. Toxic anterior segment syndrome. J Cataract Refract Surg 2006;32:324. *On-line *ASCRS and ASORN Toxic anterior segment syndrome task force guidelines. Recommended practices for cleaning and sterilizing intraocular surgical instruments, June , *Cohen AW, Oetting TA. Toxic Anterior Segment Syndrome (TASS): A System s Based View of a Day in the Life of a Canula. EyeRounds.org. May 7, 2008 [cited --insert today s date here -- ]; Available from: Anterior-Segment-Syndrome-TASS-Systems-Based.htm..")
28
The End

Similar presentations



 Visual loss 2)Surveillance of retinopathy 3)Laser therapy.>")

>")


 Dislocation M.R. Akhlaghi MD.>")







 I am encouraged by my colleagues to report any patient safety concerns.>")



