Download presentation
Presentation is loading. Please wait.

1
PEDIATRIC ENDODONTICS
PULPOTOMY Formocresol Devitalization Preservation Glutaraldehyde Regeneration MTA Presented By: Dr. Rajeev Kumar Singh

2
DEFINITION Finn Pulpotomy can be defined as the complete removal of coronal portion of the dental pulp, followed by placement of suitable dressing or medicament that will promote healing & preserve vitality of the tooth

3
Pulpotomy/Pulpectomy
+ OTOMY to make an incision or cut into PULP + ECTOMY surgical excision of a part

5
Maintain the tooth in the dental arch
Removal of inflamed & infected coronal pulp thus preserving the vitality of the radicular pulp and allowing it to heal Maintain the tooth in the dental arch

7
Cariously exposed primary teeth, when their retention is more advantageous than extraction and replacement with a space maintainer. clinical and radiographic signs of radicular pulp vitality Pain, if present not spontaneous nor persists after removal of the stimulus Tooth which is restorable Tooth with at least 2/3rd root length Haemorrhage from the amputation site is bright red & easy to control

8
root resorption exceeds more than one-third of the root length
the tooth crown is non-restorable highly viscous, sluggish, or absent hemorrhage is observed at the radicular canal orifices marked tenderness to percussion mobility with locally aggravated gingivitis associated with partial or total radicular pulp necrosis exists radiolucency exists in the furcal or periradicular areas Persistent toothaches and coronal pus

9
Indications ?? Contra-indications ??

10
Classification Vital Non-vital Devitalization Regeneration
Preservation One visit Two visits According to removal of coronal tissue Partial Complete

11
Devitalization Pulpotomy
(mummification, cauterization) One visit Two visits Formocresol Gysi Triopaste Electro surgery Easlick’s Formaldehyde Paraform devitalizing paste Laser Destroy or mummify the vital tissues
 One visit. Two visits. Formocresol. Gysi Triopaste. Electro surgery. Easlick’s Formaldehyde. Paraform devitalizing paste. Laser. Destroy or mummify the vital tissues.")
12
Preservation Pulpotomy
(minimal devitalization, non-inductive) Zinc Oxide Eugenol Glutaraldehyde Ferric sulfate Maintain maximum vital tissue without induction of reparative dentin
 Zinc Oxide Eugenol. Glutaraldehyde. Ferric sulfate. Maintain maximum vital tissue without induction of reparative dentin.")
13
Regeneration Pulpotomy
(inductive, reparative) Calcium hydroxide Bone Morphogenic Proteins MTA Enriched collagen Osteogenic protein Freezed dried bone Formation of dentin bridge
 Calcium hydroxide. Bone Morphogenic Proteins. MTA. Enriched collagen. Osteogenic protein. Freezed dried bone. Formation of dentin bridge.")
14
Classification ??

15
Formocresol introduced in 1904 by Buckley
Buckley contended that equal parts of formalin and tricresol would react chemically with the intermediate & end products of pulp inflammation to form a “new, colorless, and non-infective compound of a harmless nature.” Buckley’s Formocresol Formaldehyde 19% Tricresol % Glycerin % Water %

16
Formocresol Mechanism of action
In spite of histologic studies that showed formalin, creosol, and paraformaldehyde to be connective tissue irritants, it was recognized early that formocresol is an efficient bactericide. It was also found to have the ability to prevent tissue autolysis by the complex chemical binding of formaldehyde with peptide groups of side chain amino acids without changing the basic structure of protein molecule.

17
Fixation of the tissue directly under the medicament was apparent. After a 7- to 14-day application, the pulps developed three distinctive zones: (1) a broad eosinophilic zone of fixation, (2) a broad pale-staining zone with poor cellular definition, and (3) a zone of inflammation diffusing apically into normal pulp tissue. After 60 days, in a limited number of samples, the remaining tissue was believed to be completely fixed, appearing as a strand of eosinophilic fibrous tissue.
 a broad eosinophilic zone of fixation, (2) a broad pale-staining zone with poor cellular. definition, and (3) a zone of inflammation diffusing. apically into normal pulp tissue. After 60 days, in a limited. number of samples, the remaining tissue was. believed to be completely fixed, appearing as a strand of. eosinophilic fibrous tissue.")
18
Formocresol Pulpotomy
One Visit devitalization Formocresol Pulpotomy first approach to pulpotomy treatment of primary teeth introduced by Sweet in 1930 as multiple-visit technique used to mummify the tissue completely Doyle in 1962 used a two visit procedure (Complete devitalization) Spedding in 1965 gave 5 minutes protocol (Partial devitalization) currently 4 minutes application time is used
 Spedding in 1965 gave 5 minutes protocol (Partial devitalization) currently 4 minutes application time is used.")
19
Formocresol Pulpotomy
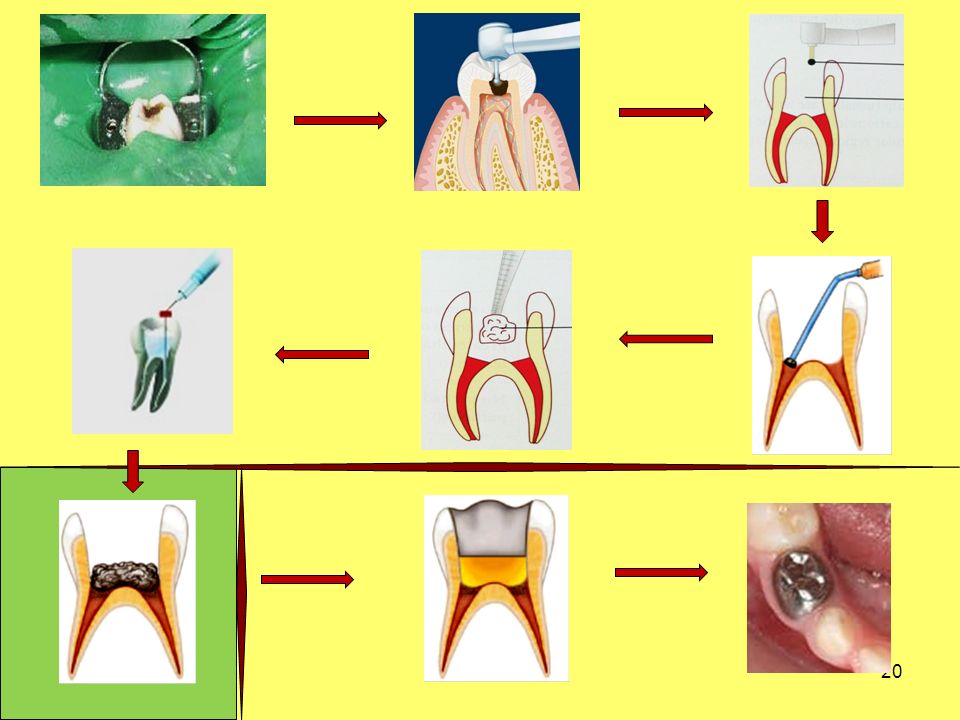
Procedure Anesthetize the tooth & isolation with rubber dam Access cavity preparation done & all caries removed The entire roof of the pulp chamber is removed using a high-speed bur All the coronal pulp is amputated with a slow-speed bur or spoon excavator Pulp chamber is thoroughly washed with saline to remove all debris Hemorrhage is controlled by slightly moistened cotton pellets placed over pulp Apply diluted formocresol to the pulp using a cotton pellet Cavity filled with ZOE paste & permanent restoration Stainless steel crown placed

21
Procedure of formocresol pulpotomy ??
Formaldehyde ?? Toxic effects ?? Procedure of formocresol pulpotomy ??

22
Alternatives to formocresol in primary teeth

23
ZOE Pulpotomy Preservation approach
Zinc oxide-eugenol (ZOE) was the first agent to used for preservation. Studies showed that eugenol possesses destructive properties, and cannot be placed directly on pulp. The success rate of ZOE pulpotomy was much less than formocresol pulpotomy. Resultant inflammation & internal resorption were the causes of failure.
 was the first agent to used for preservation. Studies showed that eugenol possesses destructive properties, and cannot be placed directly on pulp. The success rate of ZOE pulpotomy was much less than formocresol pulpotomy. Resultant inflammation & internal resorption were the causes of failure.")
24
Glutaraldehyde pulpotomy
Preservation approach Glutaraldehyde pulpotomy It was suggested by Gravenmade. Kopel in an initial study used 2% Glutaraldehyde and suggested that it can be used in primary teeth pulpectomies. Mechanism of action The histologic picture of a Glutaraldehyde treated pulp shows a zone of superficial fixation with very little underlying inflammation, so a larger amount of radicular pulp tissue remained vital.

25
Glutaraldehyde pulpotomy As compared to formocresol
Preservation approach Glutaraldehyde pulpotomy Advantages Superior fixation by cross linkage with proteins Excellent antimicrobial Self limiting penetration Less necrosis of pulpal tissues Rapidly metabolized Less toxicity Less systemic distribution Disadvantages Solution is unstable Neither optimum concentration nor application time has been established Lower levels of clinical success with increasing time As compared to formocresol

26
Ferric sulfate Pulpotomy
Preservation approach Ferric sulfate Pulpotomy Ferric sulfate is a non-aldehyde chemical which has been used commonly as an astringent. Mechanism of action It is still unclear. It was proposed that Ferric sulfate might prevent problems encountered with clot formation and thereby minimize the chances for inflammation and internal resorption. Possibly the metal-protein clot at the surface of the pulp stumps acts as a barrier to the irritative components of the subbase.

27
Ferric sulfate Pulpotomy
Preservation approach Ferric sulfate Pulpotomy Application a 15.5% solution of ferric sulfate is applied to the radicular pulp stumps for 10 to15 seconds. It may be applied using a cotton pellet or by allowing small droplets of the solution to drip from a burnisher tip onto the surface of the pulp tissue. Success Both ferric sulfate and formocresol pulpotomies similarly give good clinical and radiographic results, with high tooth survival rate.

28
Ferric sulfate Pulpotomy
Preservation approach

29
MTA Pulpotomy

30
Surely we agree that the ideal pulpotomy treatment
should leave the radicular pulp vital and healthy and completely enclosed within an odontoblast-lined dentin chamber. In this situation, the tissue would be isolated from noxious restorative materials in the chamber, thereby diminishing the chances of internal resorption. Additionally, the odontoclasts of an uninflamed pulp could enter into the exfoliative process at the appropriate time and sustain it in a physiologic manner. Implied in this scenario is the induction of reparative dentin formation by the pulpotomy agent. Unlike the other two categories for pulp treatment, the rationale for the developing field of regeneration is actually based on sound, biologic principles.

31
Formulation of a One-Fifth Dilution of Formocresol Solution
1 part Buckley’s formocresol solution is mixed with: • 1 part distilled water and 3 parts glycerin.

32
A 5-minute application resulted in surface fixation of
normal tissue, whereas an application sealed in for 3 days produced calcific degeneration. They concluded that formocresol pulpotomy in primary pulp therapy may be classified as either vital or nonvital, depending on the duration of the formocresol application.

33
a wide range of pulpal reactions occurred, from normal pulps to total
chronic inflammation. In most instances, however, the pulp tissue in the apical region was vital with minimal inflammation, which was in agreement with many other studies. It was concluded from both studies that the formocresol method should be regarded as only a means to keep primary teeth with pulp exposures functioning for a relatively short period of time.

34
Correct diagnosis is essential to ensure the clinician
that inflammation is limited to the coronal pulp.208 Biopsy studies of pulp tissue removed from the opening of root canals under pulpotomies have demonstrated the unreliability of clinical assessments in primary teeth.192 Radiographic examinations are therefore necessary to confirm the need for pulpotomy therapy in primary teeth. It is judicious to take bitewing and periradicular radiographs so that the depth of caries may be observed and the condition of the periradicular tissues determined.

35
One-Appointment Pulpotomy. Indications. This
method of treatment should be carried out only on those restorable teeth in which it has been determined that inflammation is confined to the coronal portion of the pulp. When the coronal pulp is amputated, only vital, healthy pulp tissue should remain in the root canals (Figure 17-10). Contraindications. Teeth with a history of spontaneous pain should not be considered. If profuse hemorrhage occurs on entering the pulp chamber, the one-step pulpotomy is also contraindicated. Other contraindications are pathologic root resorption, roots that are two-thirds resorbed or internal root resorption, interradicular bone loss, presence of a fistula, or presence of pus in the chamber
. Contraindications. Teeth with a history of spontaneous. pain should not be considered. If profuse. hemorrhage occurs on entering the pulp chamber, the. one-step pulpotomy is also contraindicated. Other. contraindications are pathologic root resorption, roots. that are two-thirds resorbed or internal root resorption, interradicular bone loss, presence of a fistula, or. presence of pus in the chamber.")
36
Two-Appointment Pulpotomy. Indications. The
two-appointment technique is indicated if there is (1) evidence of sluggish or profuse bleeding at the amputation site, (2) difficult-to-control bleeding, (3) slight purulence in the chamber but none at the amputation site, (4) thickening of the periodontal ligament, or (5) a history of spontaneous pain without other contraindications. The two-step pulpotomy can also be used when shorter appointments are necessary to facilitate patient management problems. Miyamoto suggested the two-appointment technique for uncooperative children to minimize chair time, especially for the initial operative visit
 evidence of sluggish or profuse bleeding at the amputation. site, (2) difficult-to-control bleeding, (3) slight. purulence in the chamber but none at the amputation. site, (4) thickening of the periodontal ligament, or (5) a history of spontaneous pain without other contraindications. The two-step pulpotomy can also be. used when shorter appointments are necessary to facilitate. patient management problems. Miyamoto suggested. the two-appointment technique for uncooperative children to minimize chair time, especially for the. initial operative visit.")
37
Calcium hydroxide was the first agent used in
pulpotomies that demonstrated any capacity to induce regeneration of dentin. 49 Even from the first, however, it was observed that the procedure was not always successful. It is considered a safe drug relative to formocresol, but, other than that, there are no strong arguments for its use.

38
Contraindications. This technique should not be
done for teeth that are (1) nonrestorable, (2) soon to be exfoliated, or (3) necrotic.
 nonrestorable, (2) soon to be. exfoliated, or (3) necrotic.")
39
The success rate of pulpotomy treatment depends to a great extent on the operator’s ability to determine whether the pulpal inflammation is confined to the coronal pulp or has possibly progressed into the root pulp as well. Numerous studies have shown that this is not possible by clinical means, and that the diagnosis will be

40
Thank You

Similar presentations












. All rights reserved. Endodontics Chapter 54 Copyright 2003, Elsevier Science (USA). All rights reserved. No part.>")






