Download presentation
Presentation is loading. Please wait.

1
Failed Tracheotomy Management Timothy M. McCulloch, MD University of Washington Harborview Hospital Otolaryngology

2
Case Report 35 year old male arrives in ER complaining of Sore throat and swallowing trouble ER Doctor finds no Neck mass or oral cavity irregularity CXR clear Calls Otolaryngology Doctor (1 hour in response)
")
3
Continued case one Oxygen saturation 99% After 50 minutes the patient complains of Shortness of breath Anesthesiology Called (10 minutes) Retracting, stridor Intubation planned
 Retracting, stridor Intubation planned")
4
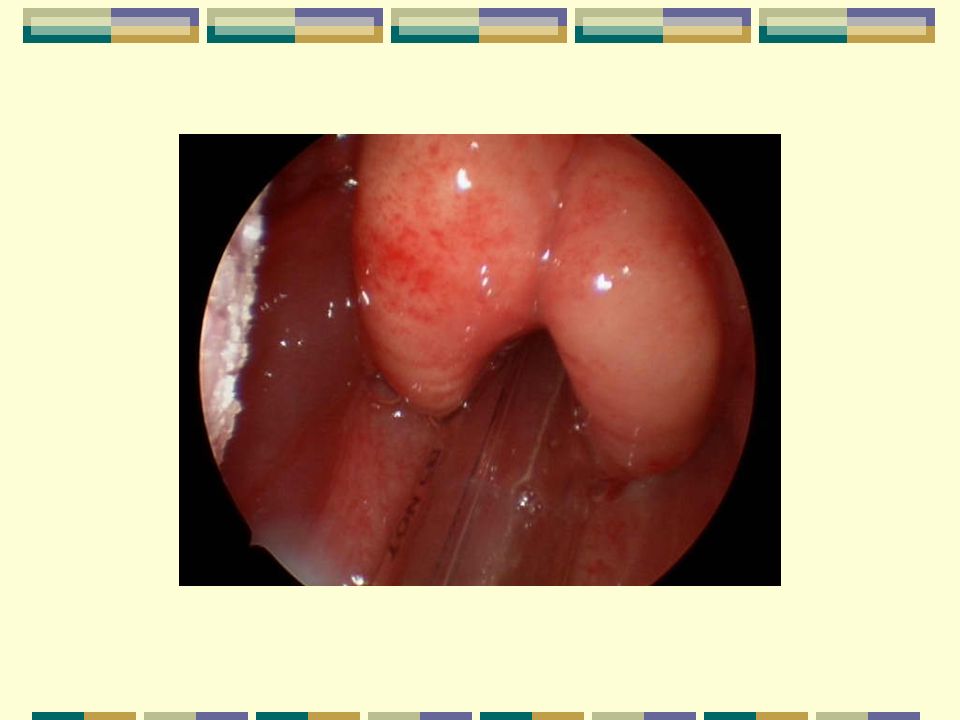
Intubation attempt Patient paralyzed Airway visualized Very swollen epiglottis and arytenoids Very erythematous bleeding started Oxygen sat drift down Otolaryngologist reaches ER- Crash Tracheotomy begun

5
Tracheotomy Tracheotomy completed 6 cuffed Shiley tracheotomy tube placed Tied with tracheotomy ties no sutures placed Patient now awake / responsive Admitted to ICU

6
ICU Morphine Sedation with Versed Ventilator setting ordered RATE 12 Volume 700 cc

7
6 hours later Midnight Patient awake Voices complaint about pain Feels short of breath Nurse call RT about “leak around tube”

8
RT and Nurse Add air to tracheotomy tube Patient medicated for “anxiety”

9
Shit hits the fan Patient become more agitated Oxygen saturations drop Removed from ventilator bagged by Hand Saturations drop Code called

10
ER doc reaches bedside Patient blue Unresponsive CPR started Sub-cutaneous air in neck and chest Needles placed in chest to treat pneumothorax Tracheotomy tube removed replaced with endotracheal tube - ventilation fails

11
PATIENT DIES

12
REVIEW THE ERRORS

13
Case Report 35 year old male arrives in ER complaining of Sore throat and swallowing trouble ER Doctor finds no Neck mass or oral cavity irregularity CXR clear Calls Otolaryngology Doctor (1 hour in response) DID NOT RECOGNIZE SUPRAGLOTTIS SLOW RESPONSE BY SPECIALIST
 DID NOT RECOGNIZE SUPRAGLOTTIS SLOW RESPONSE BY SPECIALIST")
15
Continued case one Oxygen saturation 99% After 50 minutes the patient complains of Shortness of breath Anesthesiology Called (10 minutes) Retracting, stridor Intubation planned DID NOT RECOGNIZE SUPRAGLOTTIS
 Retracting, stridor Intubation planned DID NOT RECOGNIZE SUPRAGLOTTIS")
16
Intubation attempt Patient paralyzed Airway visualized Very swollen epiglottis and arytenoids Very erythematous bleeding started Oxygen sat drift down Otolaryngologist reaches ER- Crash Tracheotomy begun PRIMARY TRACHEOTOMY PLAN WOULD HAVE BEEN BEST

17
Tracheotomy Tracheotomy completed 6 cuffed Shiley tracheotomy tube placed Sutures placed to close wound Tied with tracheotomy ties no sutures placed Patient now awake / responsive Admitted to ICU OR REVISION WOULD HAVE BEEN BEST TUBE MOST LIKELY TOO SMALL NO SUTURES PLACED TO ADD SECURITY SUTURES CLOSING WOUND - BAD IDEA

19
ICU Morphine Sedation with Versed Ventilator setting ordered RATE 12 Volume 700 cc POOR MANAGEMENT OF AWAKE PATIENT OXYGEN Supplementation or Total Airway control

20
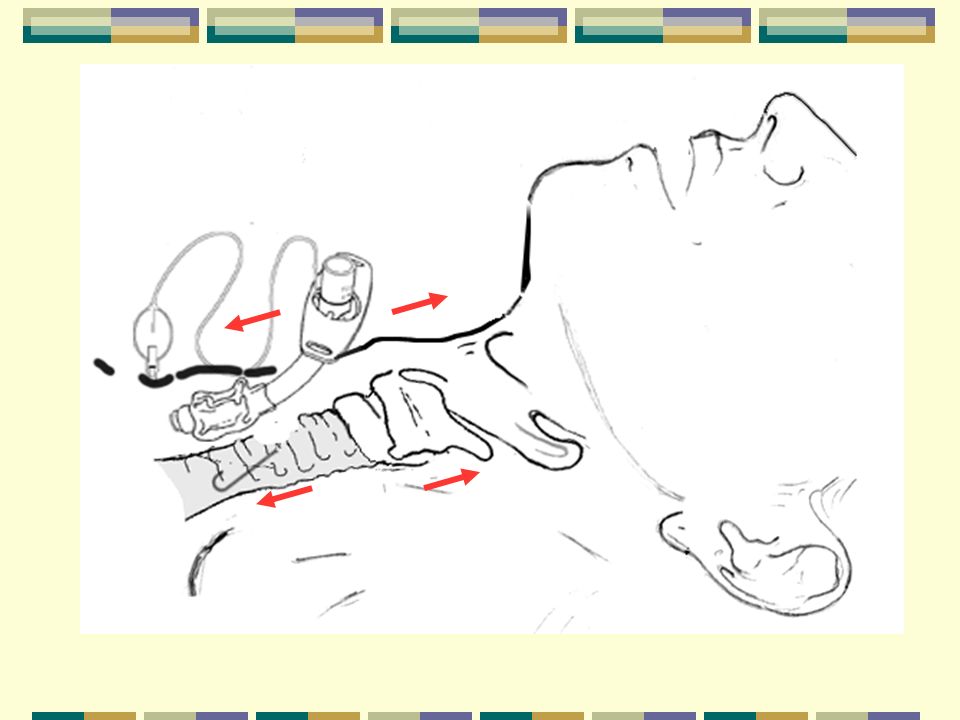
6 hours later Midnight Patient awake Voices complaint about pain Feels short of breath Nurse call RT about “leak around tube” DID NOT RECOGNIZE DISPLACED TUBE

22
Weight of vent tubing

23
RT and Nurse Add air to tracheotomy tube cuff Patient medicated for “anxiety” DID NOT RECOGNIZE DISPLACED TUBE ADDS TO PROBLEM BY ADDING AIR

24
Additional air makes it impossible to fit back into trachea

25
Shit hits the fan Patient become more agitated Oxygen saturations drop Removed from ventilator bagged by Hand Saturations drop Code called DID NOT RECOGNIZE DISPLACED TUBE ADDS TO PROBLEM BY BAGGING PATIENT

26
Forced ventilation leads to subcutaneous air, pneumothorax Failed exhalation, no inhalation

27
ER doc reaches bedside Patient blue Unresponsive CPR started Sub-cutaneous air in neck and chest Needles placed in chest to treat pneumothorax Tracheotomy tube removed replaced with endotracheal tube - ventilation fails DID NOT RECOGNIZE DISPLACED TUBE ADDS TO PROBLEM BY ADDRESSING CHEST

28
PATIENT DIES FORGOT ABCs

29
NO egress Ties not places or too loose Unrecognized displacement tube too short Poor balloon management Patient fighting vent,coughing, moving, pulling on tubes FORGOT ABCs

34
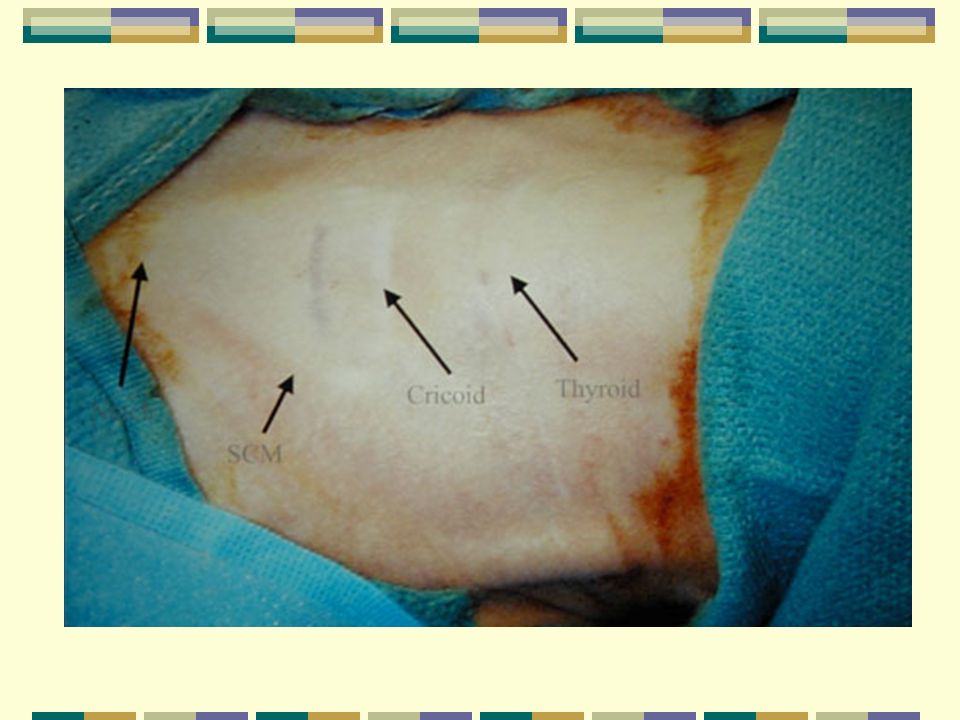
2 cm fat, vessels, thyroid

39
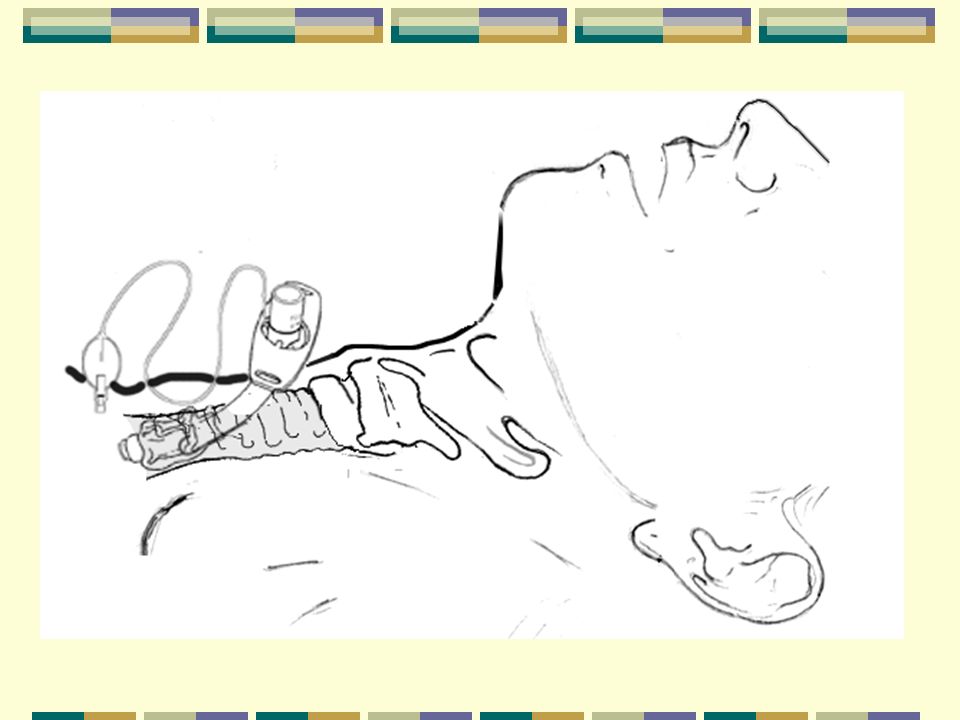
Thoughts when dislodged tube suspected Deflate cuff and advance tube Bag gently and watch for chest rise Fell for resistance Watch for subcutaneous swelling and air. Remove and replace under direct vision Mask patient Unless there is an upper airway problem this should work Air should escape trach site cover with finger.

40
Direct Visualization

41
Fiber optic visualization

42
Replace the tube with something with greater options

43
High Risk Patients Semi-sedated Quadriplegic Restrained Recent unit transfers Obese Poor lung function Cardiac problems Heparinized

44
Other issues Changing Tracheotomy tube Early and Late Tracheotomy site bleeding Granulation tissue, wound edges, major artery bleeds Bleeding post suctioning Balloon leaks and tracheomalacia Chronic high pressure

45
THANK YOU Tim

Similar presentations











 – Oral-tracheal – Naso-tracheal Tracheostomy (trach) 1.>")










 Andrew Brainard 1.>")


