Download presentation
Presentation is loading. Please wait.

1
GOUT Gout is a true crystal deposition disease, and is defined as the pathological reaction of the joint or periarticular tissues to the presence of monosodium urate monohydrate (MSU) crystals
 crystals")
2
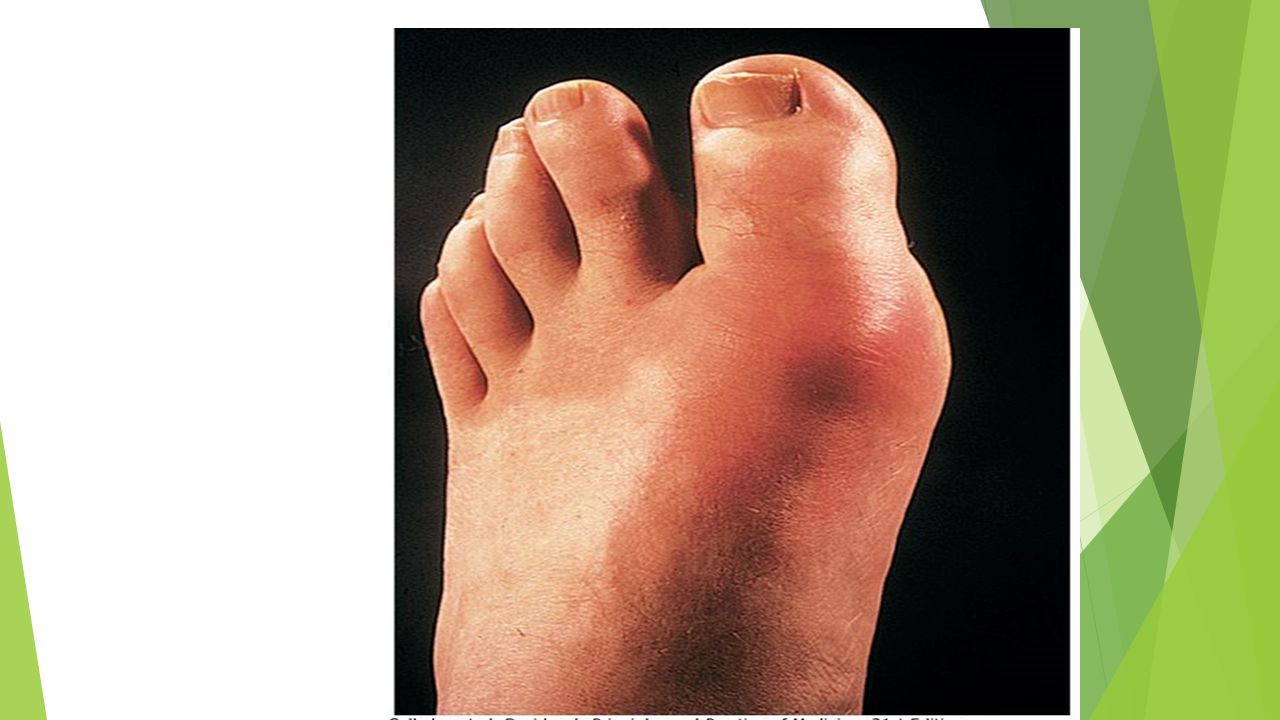
. MSU crystals preferentially deposit in peripheral connective tissues in and around synovial joints, initially favouring lower rather than upper limbs and especially targeting the first MTP joint and small joints of feet and hands.

3
Epidemiology The prevalence of gout varies between populations but is approximately 1-2%, with a strong male predominance (> 5:1). It is the most common inflammatory arthritis in men and in older women.

4
SUA levels are distributed in the community as a continuous variable

5
Levels are higher in men than women they rise from the age of 20 in men and after the menopause in women, positively correlate with obesity and vary according to ethnicity

6
Hyperuricaemia is defined as an SUA level greater than 2 standard deviations above the mean for the population. Only a minority of hyperuricaemic people develop gout, emphasising the importance of tissue factors in crystal formation.

7
Aetiology Primary gout About one-third of the body uric acid pool is derived from dietary sources and two-thirds from endogenous purine metabolism

8
The concentration of uric acid in body fluids depends on the balance between its synthesis and elimination by the kidneys (two-thirds) and gut (one-third). Purine nucleotide synthesis and degradation are regulated by a network of enzyme pathways; xanthine oxidase catalyses the end conversion of hypoxanthine to xanthine and then xanthine to uric acid.

9
In over 90% of patients with primary gout hyperuricaemia results from an inherited defect in fractional uric acid excretion which impairs their ability to increase urate excretion in response to a purine load

10
Risk factors and associations for primary gout include metabolic syndrome, high alcohol intake (predominantly beer which contains guanosine) diets relatively high in red meat fructose relatively low in vitamin C or coffee.
 diets relatively high in red meat fructose relatively low in vitamin C or coffee.")
11
Secondary gout 1 Diminished renal excretion (common Inherited isolated renal tubular defect ('under- excretors') Renal failure Chronic drug therapy Thiazide and loop diuretics Low-dose aspirin Ciclosporin Pyrazinamide
 Renal failure Chronic drug therapy Thiazide and loop diuretics Low-dose aspirin Ciclosporin Pyrazinamide")
12
Lead toxicity Lactic acidosis (alcohol

13
2 Increased production of uric acid

14
Increased purine turnover Chronic myeloproliferative or lymphoproliferative disorders (e.g. polycythaemia, chronic lymphatic leukaemia) Increased de novo synthesis ('over-producers') Unidentified abnormality (most common) Specific enzyme defect (rare) Hypoxanthine-guanine phosphoribosyl transferase deficiency Phosphoribosyl pyrophosphate synthetase over- activity Glucose-6-phosphatase deficiency
 Increased de novo synthesis ( over-producers ) Unidentified abnormality (most common) Specific enzyme defect (rare) Hypoxanthine-guanine phosphoribosyl transferase deficiency Phosphoribosyl pyrophosphate synthetase over- activity Glucose-6-phosphatase deficiency.")
15
In almost all first attacks a single distal joint is affected. The first MTP joint is affected in over 50% of cases-'podagra' ('seizing the foot', Acute gout

16
Other common sites are, in order of decreasing frequency, the ankle, midfoot, knee, small joints of hands, wrist and elbow. The axial skeleton and large proximal joints are rarely involved and never as the first site. Typical attacks have the following characteristics

17
Extremely rapid onset, reaching maximum severity in just 2-6 hours, often waking the patient in the early morning severe pain, often described as the 'worst pain ever'

18
Extreme tenderness: the patient is unable to wear a sock or to let bedding rest on the joint Mswelling with overlying red, shiny skin Self-limiting over 5-14 days, with complete return to normality.

19
There may be accompanying fever, malaise and even confusion, especially if a large joint such as the knee is involved. As the attack subsides, pruritus and desquamation of overlying skin are common.

26
The main differential diagnosis is Septic arthritis, Infective cellulitis Another crystal disease. Sepsis, however, is usually more subacute in onset and progresses in severity until treated

27
Recurrent and chronic gout After an acute attack, some people never have a second episode; in others the next episode occurs after years. In most, however, a second attack occurs within 1 year and the frequency of attacks gradually increases with time.

28
Eventually, continued MSU deposition causes joint damage and chronic pain. The interval between the first attack and the development of chronic symptoms is variable but averages around 10 years

29
Chronic tophaceous gout Large MSU crystal deposits produce irregular firm nodules ('tophi') around extensor surfaces of fingers, hands, forearm, elbows, Achilles tendons and sometimes the helix of the ear. The white colour of MSU crystals may be evident and permits distinction from rheumatoid nodules

34
Renal and urinary tract manifestations Uric acid (not MSU) stones cause renal colic in around 10% of gout patients Progressive renal disease is an important complication confined to untreated severe chronic tophaceous gout. This results from MSU crystal deposition in the interstitium of the medulla and pyramids with consequent chronic inflammation, giant-cell reaction, fibrosis, glomerulosclerosis and secondary pyelonephritis

35
Secondary gout may present with painful, sometimes discharging, tophi without preceding acute attacks. This is particularly seen in older, mainly female patients with nodal OA who develop tophi in and around their osteoarthritic finger joints as a consequence of chronic (> 1-2 years) diuretic therapy
 diuretic therapy.")
37
Investigations Definitive diagnosis requires identification of MSU crystals in the aspirate from a joint, bursa or tophus

38
In acute gout, synovial fluid shows increased turbidity due to the greatly elevated cell count (> 90% neutrophils); chronic gouty fluid is more variable but occasionally appears white due to the high crystal load. Between attacks, aspiration of an asymptomatic first MTP joint or knee may still permit crystal identification.

39
Measurement of 24-hour urinary uric acid excretion on a low purine diet will identify an over-producer. Assessment of renal function (serum creatinine, urinalysis), hypertension, blood glucose and serum lipid profile should be undertaken.
, hypertension, blood glucose and serum lipid profile should be undertaken..")
40
X-rays can assess the degree of joint damage. In early disease they are usually normal, but changes of OA may develop in affected joints with time, or be present as a predisposing factor in secondary gout.

42
Gouty 'erosions' (bony tophi) are a less common but more specific feature occurring as para-articular 'punched-out' defects with well-delineated borders and retained bone density
 are a less common but more specific feature occurring as para-articular punched-out defects with well-delineated borders and retained bone density")
43
Management The acute attack A fast-acting oral NSAID (plus a PPI) can give effective pain relief and is the standard treatment, together with local ice packs. Patients can keep a supply of an NSAID and take it as soon as the first symptoms occur, continuing until the attack resolves

44
. Oral colchicine (a potent inhibitor of neutrophil microtubular assembly) is also very effective but often causes vomiting and severe diarrhoea at high doses; a low-dose regimen (0.5 mg 6-, 8- or 12-hourly) is therefore recommended
 is also very effective but often causes vomiting and severe diarrhoea at high doses; a low-dose regimen (0.5 mg 6-, 8- or 12-hourly) is therefore recommended.")
45
Joint aspiration can give instant relief and, when combined with an intra-articular steroid injection to prevent fluid reaccumulation, often effectively aborts the attack. For severe oligo- or polyarticular attacks, parenteral corticosteroid is sometimes used.

46
Long-term management Once an acute attack has settled, predisposing factors should be corrected if possible. Weight loss and reduction of excess alcohol intake, especially beer, may significantly reduce hyperuricaemia. Diuretics should be stopped if possible.

47
A very high purine diet (e.g. seafood, red meat, ) should be tempered but there is no need for a highly restrictive diet. Associated comorbidity should be treated appropriately.
 should be tempered but there is no need for a highly restrictive diet. Associated comorbidity should be treated appropriately..")
48
Indications for urate-lowering drugs Recurrent attacks of acute gout Tophi Evidence of bone or joint damage Associated renal disease and/or nephrolithiasis Gout with greatly elevated serum uric acid

49
Allopurinol is the drug of choice. It is a xanthine oxidase inhibitor, which reduces the conversion of hypoxanthine and xanthine to uric acid. The recommended starting dose is 100 mg daily, but 50 mg in older patients or if renal function is impaired.

50
The reduction in tissue uric acid levels that follows initiation of ULT can partially dissolve MSU crystals and trigger acute attacks. The patient should be warned of this and told to continue ULT, even if an attack occurs. The risk can be minimised by using a low starting dose (50-100 mg rather than 300 mg), or by concurrent administration of oral colchicine (0.5 mg 12-hourly) or an NSAID for the first few months.
, or by concurrent administration of oral colchicine (0.5 mg 12-hourly) or an NSAID for the first few months..")
51
Febuxostat is a recently introduced xanthine oxidase inhibitor that is useful in patients in whom allopurinol is not tolerated or contraindicated. It commonly provokes attacks at the recommended starting dose (80 mg daily) so prophylaxis with colchicine or NSAID is advised for the initial 6 months. It undergoes hepatic metabolism and so no dose adjustment is required for renal impairment.
 so prophylaxis with colchicine or NSAID is advised for the initial 6 months. It undergoes hepatic metabolism and so no dose adjustment is required for renal impairment..")
52
Uricosuric drugs such as probenecid or sulfinpyrazone can be effective but require several doses each day and maintenance of a high urine flow to avoid uric acid crystallisation in renal tubules. Salicylates antagonise the uricosuric action of these drugs and should be avoided

53
. Uricosurics are contraindicated in over- producers, in those with renal impairment and in urolithiasis (they increase stone formation). benzbromarone (50-200 mg daily) can be very effective and safe in mild to moderate renal impairment but can rarely causeThe uricosuric hepatotoxicity; availability is limited in most countries
. benzbromarone ( mg daily) can be very effective and safe in mild to moderate renal impairment but can rarely causeThe uricosuric hepatotoxicity; availability is limited in most countries.")
54
Asymptomatic hyperuricaemia Although hyperuricaemia is an independent risk factor for hypertension, vascular disease, renal disease and cardiovascular events, there is no evidence that ULT is effective in the treatment of these diseases.

Similar presentations
















 Purine degradation pathway Fate of uric acid in humans Gout and hyperuricemia: Biochemistry Types Treatment.>")


>")




 Mononucleotides.>")
.>")


 Mononucleotides.>")

