Download presentation
Presentation is loading. Please wait.

1
Severe Acute Respiratory Syndrome (SARS)
GP seminars

2
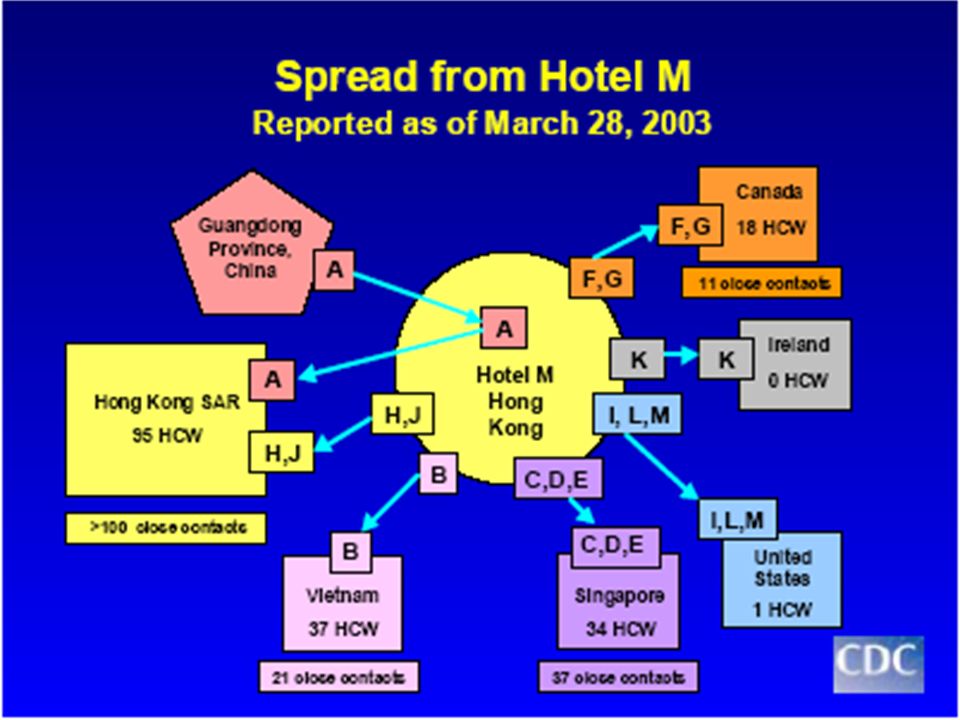
SARS Guangdong Province, China “ outbreak of atypical pneumonia”
Mid November 2002 Guangdong Province, China “ outbreak of atypical pneumonia” 11 February 2003 WHO informed 305 cases (5 deaths) 30% in health care workers July 2003 8,437 probable cases from 32 countries major foci in China, SE Asia and Toronto 4 in UK (none from NI)
 30% in health care workers. July ,437 probable cases from 32 countries. major foci in China, SE Asia and Toronto. 4 in UK (none from NI)")
3
Hasn’t SARS been eliminated?
On 5 July WHO said outbreak was contained. BUT WHO have warned it might return and urged planning for it. Majority of experts think it might return. Planning for it remains a high government priority.

4
Why might it return? Other new and poorly understood viruses (e.g. Ebola and Marburg) periodically surface to cause outbreaks then disappear again. This is a respiratory illness – these are usually worse in winter and disappear in summer. We don’t know how it appeared or where from – so can’t be confident of stopping it from doing so again.

5
It is very important that SARS is taken seriously and that we prepare properly for it. It is a moderately infectious disease with a significant mortality rate and no effective treatment or vaccine. Nevertheless by being adequately prepared and taking proper infection control measures we can ensure that we are well protected and any risk is minimised.

6
It is also important to keep things in perspective, compared to many infectious diseases SARS had a small impact. This obviously shouldn’t lead to complacency – without a rigorous worldwide response the situation could have been a lot worse.

7
SARS coronavirus (SARS CoV)
New member of coronavirus family found in wild animals in China incubation period 2-7 (max 10) days viral shedding peaks 6-10 days after onset of symptoms droplet spread less infectious than influenza no vaccine available
 days. viral shedding peaks 6-10 days after onset of symptoms. droplet spread. less infectious than influenza. no vaccine available.")
9
SARS CoV - infectivity Most transmission via close contact with a symptomatic person via large respiratory droplets. Transmission by fomites possible. Those severely ill more infectious (attack rate of >50% in some hospital staff) Infectivity increases during second week of illness Transmission from an asymptomatic person unlikely May remain infectious up to 10 days once afebrile
 Infectivity increases during second week of illness. Transmission from an asymptomatic person unlikely. May remain infectious up to 10 days once afebrile.")
11
SARS CoV - infectivity (MMWR 2003:52 (18): )
: )")
12
Clinical symptoms at presentation (in %)
99 28* 69 49 31 2 12 n.a 24 35 94 65* 50 51 64 25 23 27 100 74 62 54 20 10 73 57 61 56 Fever Chills or rigors Cough Myalgia Malaise Runny Nose Sore Throat Shortness of breath Diarrhoea Headache Booth et al. n=144 Donnelly et al. n>1250 Peiris et al. n=50 Lee et al. n=138 * chills

13
Clinical course - triphasic
Week 1 fever, myalgia, systemic symptoms that improve after a few days Week 2 Fever returns, oxygen desaturation, CXR worsens Later 20% get ARDS needing ventilation Peiris - Lancet 2003b; 361:

14
SARS - morbidity Most cases are in healthcare workers caring for SARS patients and close family members of SARS patients overall mortality 15% mortality increases with age (> 65 years - 50% mortality) children seem to develop mild illness
 children seem to develop mild illness.")
15
Clinical case definition
A respiratory illness severe enough for hospitalisation and include a history of: Fever (> 380C) and one or more symptoms of respiratory tract illness (cough, difficulty breathing, SOB) CXR of lung infiltrates consistent with pneumonia or RDS or PM consistent with pneumonia or RDS without an identifiable cause No alternative diagnosis to fully explain the illness CDSC Colindale 15 Aug 03
 and. one or more symptoms of respiratory tract illness (cough, difficulty breathing, SOB) CXR of lung infiltrates consistent with pneumonia or RDS or PM consistent with pneumonia or RDS without an identifiable cause. No alternative diagnosis to fully explain the illness. CDSC Colindale 15 Aug 03.")
16
SARS diagnosis Clinical findings of an atypical pneumonia not attributed to other causes exposure to suspect/probable SARS or exposure to their respiratory secretions or body

17
SARS laboratory diagnosis
PCR positive for SARS CoV using validated methods on at least 2 different clinical specimens Seroconversion (gold standard) (negative antibody test on acute specimen followed by positive test on convalescent sera or > 4 rise in antibody titre between acute and convalescent sera) The gold standard is seroconversion after 21 days. A negative PCR could mean that no virus was in the sample taken, the PCR was insufficiently sensitiveand.or there was no SARS CoV causing this infection. A positive PCR indicates the person has/had recent SARS infection with SARS CoV and this might have been the cause of SARS in this patient. As viral shedding peaks during second week of symptoms if tests are done too soon may not pick up the virus
 (negative antibody test on acute specimen followed by positive test on convalescent sera or > 4 rise in antibody titre between acute and convalescent sera) The gold standard is seroconversion after 21 days. A negative PCR could mean that no virus was in the sample taken, the PCR was insufficiently sensitiveand.or there was no SARS CoV causing this infection. A positive PCR indicates the person has/had recent SARS infection with SARS CoV and this might have been the cause of SARS in this patient. As viral shedding peaks during second week of symptoms if tests are done too soon may not pick up the virus.")
18
SARS - treatment Supportive avoid aerosol inducing interventions
evidence base for anti-viral drugs lacking steroids may be helpful

19
NI SARS contingency plan: levels of response
0: initial preparedness (no active cases in UK/Ireland) 1: (A) sporadic imported case(s) to GB/Ireland 1: (B) sporadic imported case(s) to NI 2: intra hospital transmission and/or limited community transmission within definable groups 3: extensive community transmission 4: post outbreak and de-escalation of outbreak response
 1: (A) sporadic imported case(s) to GB/Ireland. 1: (B) sporadic imported case(s) to NI. 2: intra hospital transmission and/or limited community transmission within definable groups. 3: extensive community transmission. 4: post outbreak and de-escalation of outbreak response.")
20
SARS preparedness NI Taskforce and subgroups Clinical Training
Port Health Training Acute Primary & Community Care Infection control Human Resources

21
Key points in control of any communicable disease
early case detection swift isolation thorough control of infection measures vigorous identification and management of close contacts by home confinement public information for those at risk of infection education of health care professionals

22
Personal protective equipment
Masks Waterproof long sleeved gowns Gloves Goggles Centrally sourced and distributed

23
Masks and Respirators. Masks
Main purpose – help prevent particles (droplets) being expelled into environment by wearer Resistant to fluids – help protect wearer from splashes of blood or other potentially infected substances Not necessarily designed for filtration efficiency, or to seal tightly to the face Protection to wearer is therefore limited.
 being expelled into environment by wearer. Resistant to fluids – help protect wearer from splashes of blood or other potentially infected substances. Not necessarily designed for filtration efficiency, or to seal tightly to the face. Protection to wearer is therefore limited.")
24
Masks and Respirators. Respirators
Intended to help reduce wearer’s exposure to airborne particles Made to defined standards When worn correctly – seal firmly to face – reducing risk of leakage Some have one way valves – would be useless for putting on infected person

25
What is the correct way to use a mask?
First – How not to do it!

26
Could result in serious injury.

27
Could result in suffocation.

28
Could result in serious injury and suffocation!

29
What is the correct way to use a mask?
Should fit snugly over mouth, nose and chin Coloured side out Metal strip at top – mould to bridge of nose If in healthcare setting dispose of as clinical waste In home – patients should place in plastic bag then in domestic waste Hands must always be washed following removal. (Remove handling straps only – avoid contact with face part)
")
30
What is the correct way to use a respirator?
Each type may differ - So always read the accompanying instructions. Do a fit check or user seal check every time a respirator is put on – Fit is critically important. It must seal tightly to the face – needs clean-shaven skin – beards, long moustaches and stubble may cause leaks. Go to a safe area to change it if: breathing becomes difficult; it becomes damage, distorted, or splashed by body fluids; or a proper face fit cannot be maintained.

31
When should masks or respirators be used?
Healthcare workers should use respirators for any contact with suspected or probable cases of SARS A mask should be used only if a respirator is not available – better than no protection Patients should use a mask while symptomatic whether in hospital, at home or in transit. But wearing a mask or respirator is not a guarantee of protection against SARS.

32
Other aspects of infection control
Hand hygiene – essential Gloves Fluid resistant long sleeve gown Eye protection (visor best) Environmental & equipment decontamination.
 Environmental & equipment decontamination.")
33
Putting on PPE Put on in following order: Respirator Eyewear Gown
Gloves – ensuring wrists of gloves are pulled up over sleeves of gown.

34
Removal of PPE Crucial that PPE is removed without accidental contamination of facial skin or mucous membranes. Remove PPE in following order: Gown Gloves Wash hands Eye protection Mask

35
Importance of Infection Control Procedures
Detailed aspects of infection control are very important e.g. exactly how to remove a gown, correct hand washing technique etc. A video describing all this will be produced and widely distributed – Please make sure you and all relevant colleagues watch it. Correct use of all infection control procedures will provide very good protection against SARS.

36
Likely pathway Sporadic cases GP - A&E - designated SARS facility
Extensive community transmission Home versus hospital management THIS WILL EVOLVE OVER TIME

37
Scenario 1: Unannounced presentation
Isolate patient Mask on patient Assessment – wear your PPE Case definition/ clinical status Refer to A&E Register of staff contacts Report to public health Decontamination

38
Scenario 2: Announced (patient at home)
Triage by telephone Home visit or refer direct to hospital Refer to A&E Report to public health Advise family

39
Implications for primary care
Get prepared now! Develop a practice protocol Develop a patient pathway (receptionist GP) Train all staff Know PPE procedures* Plan decontamination systems (include nebulisers)* Identify a dedicated room. Situation has potential to change rapidly!
 Train all staff. Know PPE procedures* Plan decontamination systems (include nebulisers)* Identify a dedicated room. Situation has potential to change rapidly!")
40
What resources are/ will be available?
Advice on decontamination Referral algorithms (?designated hospitals) Training materials CCDC/ on-call public health Updated DHSSPS communications Websites:
 Training materials. CCDC/ on-call public health. Updated DHSSPS communications. Websites:")
Similar presentations


 in Healthcare Settings>")



 Middle East Respiratory Syndrome (MERS) is viral respiratory illness first reported in Saudi Arabia in 2012.>")


 Quek Boon Har UMMC.>")

 AGENT SUSCEPTIBLE HOST RESERVOIR.>")





 © 2009 International SOS Assistance, Inc.. All rights reserved. Unauthorized copy.>")
 With the spread of Ebola to the U.S., ensuring our employees and communities are safe is the utmost.>")

