Download presentation
Presentation is loading. Please wait.

1
Zareh.F.MD

2
All bleeding during pregnancy should be investigated by examination and imaging studies

3
1/4 of women who bleed at 14-26 w had pp or ap. 1/3 of pregnancy with vag bleeding after 26 w had poor outcome. Unexplained vag.bleeding at term must be considered for delivery.

4
etiologies Placenta previa Placenta abruption Vasa previa Cervical lesions (carcinoma,polyps) Vaginal laceration (trauma,carcinoma) Uterine rupture or dehiscence
 Vaginal laceration (trauma,carcinoma) Uterine rupture or dehiscence")
6
Placenta previa incidece 0.5-1% of all pregnancies Fatal 0.03% of cases Incidence in multipar :1/20 Incidence in nulipar : 1/1500

7
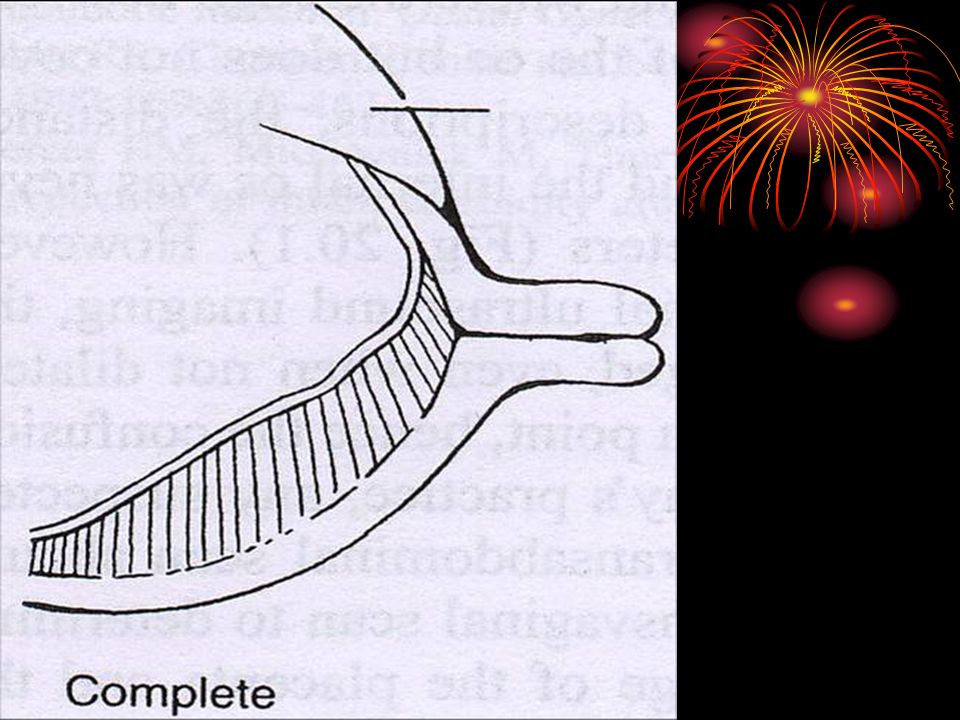
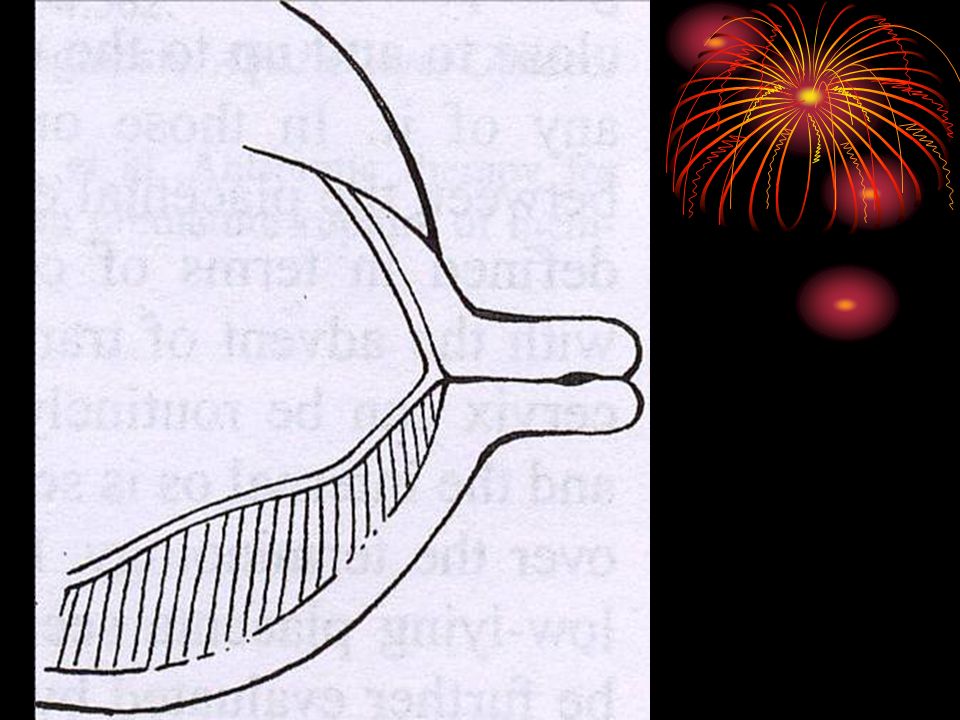
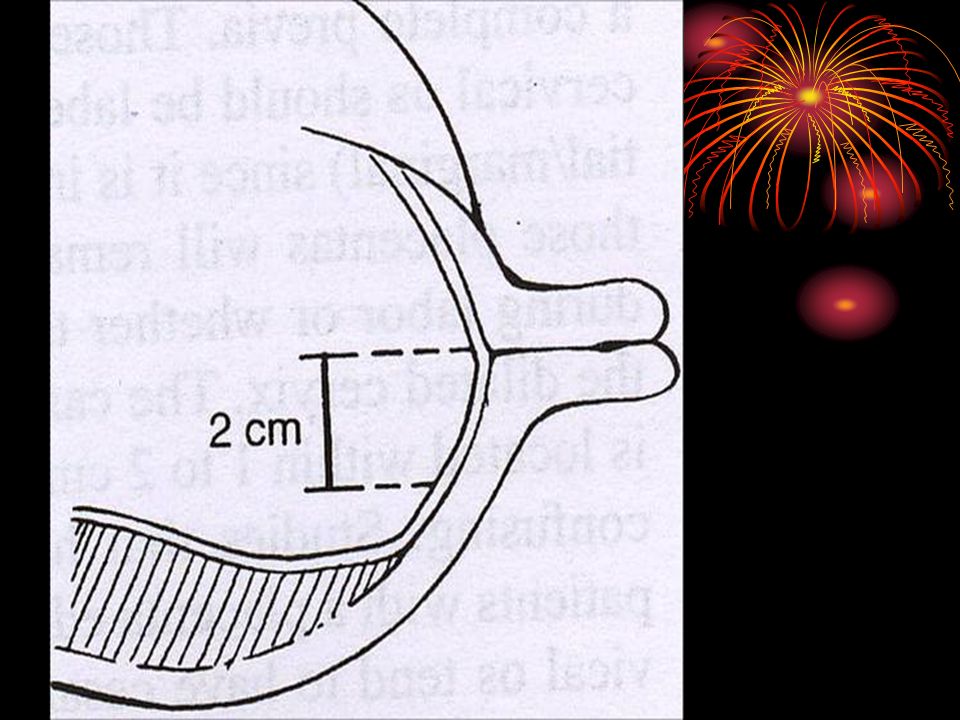
difinition Dillated cervix: complete previa partial previa marginal previa low lying Closed cervix: complete partial / marginal 2 cm from int.os

12
pathophysiology Abnormal endometrial tissue less favorable location for implantation: poor vascularization thinner myometrium Uterine trauma from c/s (6 fold)
")
13
Risk factors Perior c/s Black, minority Older women >35 y High gravidity & parity Cigarette smoking 2.6-4.4 fold Previous abortion

14
diagnosis Abdominal sonography misdiagnosis : full distended bladder lower ut segment contraction pp in 2nd trimester 90-95% resolved by the 3rd trimester(but no central) 3 dimensional scanning transvaginal scan Transperineal scan Double set up examination MSAFP>2 MoM
 3 dimensional scanning transvaginal scan Transperineal scan Double set up examination MSAFP>2 MoM")
15
Clinical features Asymptomatic Vaginal bleeding variable intermittent red to brownish maternal origin the fetus usually not in jeopardy

16
complication Hospital stay c/s Abruptio placenta Malpresentation Post partum hemorrhage Growth restriction Placenta accreta pp+previous c/s10-35% +multiple c/s 60-65% Coagulation defect

17
Other complications A.T.N Sheehan syndrome Maternal mortality<1% Perinatal mortality <5%

18
outcome IUGR ? Preterm birth Congenital anomaly Respiratory distress syndrome Anemia Recurrence rate 2-3%(6-8 fold)
.")
19
management no bleeding 2nd trimester intercourse avoid usual activity repeat sonography 3rd trimester decrease physical activity travel away from home prolonged bed rest

20
management with Bleeding Evaluation of the patient Fetal status IV fluid Blood cross match RHoGam if necessary Steroid if 24-34 W Delivery after 34-36W

21
management Severe hemorrhage Medical team for immediate delivery 2 large bore IV line Blood cross match Foley catheter Coagulation panel Continuous Fetal monitoring delivery

23
Premature separation of placenta. 0.5-1% of deliveries Perinatal mortality is 20-25% Preterm birth is 40% Cause of 15% of stillbirth

24
Definition Preplacental or subamniotic

27
retroplacental

28
Risk factors Socioeconomic: High parity low education infertility

29
Risk factors Uterine: ut.malformation ut.septum Myoma

30
Risk factors Medical: Diabete pregestational Hypertension _chronic&gestational PROM with chorioamnionitis

31
Risk factors Thrombophilias Antiphospholipid syndrome Prothrombin 20210A mutation Hyperhomocysteinemia Factor V leiden mutation Activated protein C resistance Protein C and S deficiency dysfibrinogenemia

32
Risk factor iatrogenic Sudden decompression(amniocentesis) External cephalic version Cigarette smoking Cocaine abuse Blant trauma Heavy physical activity
 External cephalic version Cigarette smoking Cocaine abuse Blant trauma Heavy physical activity")
33
pathophysiology Blunt trauma : forceful shearing effort Majority of other case : cell death (apoptosis) induced through ischemia,hypoxia. Thrombophilia : thrombose in decidua basalis Chorioamnionitis: infectious agents (lipopolysacharids & endotoxins) cytokines,superoxide ischemia and hypoixia
 cytokines,superoxide ischemia and hypoixia.")
34
Pathophysiology cont. Nicotine(cigarete) and cocaine vasoconstriction ischemia placental lesions(infarction,oxidative stress,appoptosis and necrosis) Circumvalate placenta(chorion leave don’t insert at the edge of placenta) A.P,IUGR,PROM,preterm labor
 and cocaine vasoconstriction ischemia placental lesions(infarction,oxidative stress,appoptosis and necrosis) Circumvalate placenta(chorion leave don’t insert at the edge of placenta) A.P,IUGR,PROM,preterm labor.")
35
diagnosis Clinically vaginal bleeding Uterine pain tetanic contraction fetal heart abnormality sinusoidal pattern

36
diagnosis Paraclinic Ultrasound MRI Doppler Biochemical test Unexplained elevated of MSAFP AP>10 fold Preterm labor+AFP>2MoM = AP (67%) Preterm labor+AFP>2MoM+bleeding= AP (100%) HCG Inhibin A Fetal Hb
 Preterm labor+AFP>2MoM+bleeding= AP (100%) HCG Inhibin A Fetal Hb")
38
management Marginal Abruptio hospitalize a patient with any bleeding after fetal viability Large retroplacental usually require acute & aggressive management

39
Large bleeding Continues fetal monitoring Foley catheter Frequent maternal v/s Steroid therapy (24-34w, membrane intact) Folic acid 1mg,vit B12,vit B6
 Folic acid 1mg,vit B12,vit B6")
40
discharge Mild bleeding : 2-5 days without any further bleeding Large bleeding :decision is difficult with any bleeding, pain, contraction no discharge

41
Tocolytic use Now become acceptable to consider a short course of tocolytic therapy for: stable patient, limited abruptio, established fetal well being, preterm G.age

42
Which tocolytic B mimetics (terbut,ritod): mask cardiovascular response to volume depletion Ca channel blockers (nifidipine): reduce BP Mgso4 : most acceptable agents
: mask cardiovascular response to volume depletion Ca channel blockers (nifidipine): reduce BP Mgso4 : most acceptable agents")
43
delivery Vaginal or c/s Depending on the: Degree of bleeding Presence or absence of: Active labor Fetal distress

44
complications c/s 50% of case Shock DIC Renal failure Couvelaire uterus Recurrence : 10 fold

45
Fetal outcome Mortality: term babies 25 fold Prematurity: 40%

46
Thrombophilia defects Anticardiolipin antibodies Lupus anticoagulant Pr c, Pr s and antithrombin 3 deficiencies Factor v leiden “activated pr c resistance” Metilentetrahydrofulate reductase gene mutation Prothrombin 20210A gene mutation Congenital dysfibrinogenemia

47
Factor V leiden Activated protein C resistance Most common genetic factor predisposing to thrombosis Most common identifiable causes Substitution of adenine for guanine “ Amino acid arginine for glutamine Increased tendency to form clots

48
hyperhomocysteinemia Methionine metabolise homocysteine damage vascular Remethylate MTHFR endothelium folate vit.B 12, vit. B 6 Methionine

Similar presentations


























>")
