Download presentation
Presentation is loading. Please wait.

1
TEMR THE ISRAELI CENTER FOR Limor Aharonson-Daniel, Israel Megan Davies, USA The Center for Trauma and Emergency Medicine Research, Gertner Institute for Epidemiology and Health Policy Research, Israel National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, Atlanta, GA USA The Barell Matrix, Updates; The Composition of TBI Rows Multiple Injury Analysis Using Matrix

2
The Matrix is a tool for classifying injury ICD-9-CM codes by body region and nature of injury. It is useful for standardized retrieval of injury cases for epidemiological, clinical and management oriented analyses What is the Matrix? Matrix Reminder

3
To characterize the patterns of injury Matrix objectives To serve as a standard for casemix comparison To simplify the process of classifying injuries To provide a standard format for reports Matrix Reminder

4
Motivation for building the matrix Sorted by nature of injury Detecting injuries by body region requires collating codes across chapters ICD 9-CM CODES 800-995 Matrix Reminder

5
ICD 9-CM CODES 800-995 Motivation for building the matrix nature of injury body region Matrix Reminder

6
The Matrix structure Nature of injury Body Region ICD-9-CM injury codes Matrix Reminder

7
Anatomic subgroups High Incidence Variability in Outcome Difference in health care utilization Body Region (Rows) are based on : Matrix Reminder Nature of injury (Columns) are based on Sequence of codes in ICD-9-CM codebook
 are based on : Matrix Reminder Nature of injury (Columns) are based on Sequence of codes in ICD-9-CM codebook")
8
Dissemination The Matrix was posted on the net by Lois in October 2001. A paper describing matrix construction will be published in the June 2002 issue of Injury Prevention.

9
“Five digit ICD-9-CM codes will be used where necessary”. “Priority codes will not be used, an “other and unspecified” by body region row will be added in order to minimize loss of information”. April 3, 2001: ICE meeting, Washington DC General Agreements Reached “Instructions on how to collapse rows will be available to ensure a standard collapsed table”.

10
“Spine will be divided to Spinal Cord injury (SCI) and to Vertebral Column injury (VCI) each group will be divided into Cervical, Dorsal, Lumbar, Sacrum and Coccyx”. ICE meeting, Washington DC, 2001 Specific Agreements,

11
“A detailed extremity module needs to be added”. ICE meeting, Washington DC, 2001 Specific Agreements,

12
“Amputations will be separated from open wound”. ICE meeting, Washington DC, 2001 Specific Agreements,

13
“Superficial injuries and contusions will be joined”. ICE meeting, Washington DC, 2001 Specific Agreements,

14
ICE meeting, Washington DC, 2001 Specific Agreements, “The matrix has a row for “system wide conditions” enabling use for non traumatic injuries”.

15
“The presence of Traumatic Brain Injury (TBI) is important. The matrix will have three rows identifying Definite TBI, possible TBI and other head injuries”. ICE meeting, Washington DC, 2001 Specific Agreements, The split of TBI conventional definition into two rows in the matrix brought about discussions with CDC NCIPC, the American Academy of Neurology and others on TBI definition and separation into several levels of TBI.

16
Original TBI definition injury to the head that is documented in a medical record, with one or more of the following conditions attributed to head injury: observed or self-reported decreased level of consciousness, amnesia, skull fracture, objective neurological or neuropsychological abnormality, or diagnosed intracranial lesion; Thurman DJ, Sniezek JE, Johnson D, Greenspan A, Smith SM. Guidelines for Surveillance of Central Nervous System Injury. Atlanta: Centers for Disease Control and Prevention, 1995.

17
Definite TBI Injuries with no mention of intracranial injury or with loss of consciousness of less than one hour. injuries with a specific mention of intracranial injury or loss of consciousness of more than one hour Original Two-row TBI definition (created by Vita Barell) A derivation from CDC definitions: concussions with no or short loss of consciousness were classified as ‘possible TBI’. Possible TBI An addition to the definition: injuries indicating damage to the optic nerve pathways: optic chiasm (950.1) optic pathway (950.2) and visual cortex (950.3)
 A derivation from CDC definitions: concussions with no or short loss of consciousness were classified as ‘possible TBI’. Possible TBI An addition to the definition: injuries indicating damage to the optic nerve pathways: optic chiasm (950.1) optic pathway (950.2) and visual cortex (950.3).")
18
CDC concerns regarding TBI separation 959.01 Concussions with no or short LOC TBI with LOC of unspecified duration TBI with unspecified level of consciousness Shaken baby syndrome Three-row TBI definition

19
Definite TBI Type 1 Injuries with no mention of intracranial injury or with no loss of consciousness Injuries with a recorded evidence of an intracranial injury or a moderate or prolonged loss of consciousness (loc). Possible TBI Three-row TBI definition Definite TBI Type 2 Injuries with no recorded evidence of intracranial injury and loc of less than one hour; loc of unknown duration or unspecified level of consciousness. Concussions.

20
Definite TBI Type 1 Injuries with no mention of intracranial injury or with no loss of consciousness Injuries with a recorded evidence of an intracranial injury or a moderate or prolonged loss of consciousness (loc). Possible TBI Three-row TBI definition Definite TBI Type 2 Injuries with no recorded evidence of intracranial injury and loc of less than one hour; loc of unknown duration or unspecified level of consciousness. Concussions. 959.01 854 Concussions with no or short LOC Shaken baby syndrome (995.55) LOC of unspecified duration Unspecified level of consciousness
 LOC of unspecified duration Unspecified level of consciousness.")
21
Possible TBI Probable TBI Plausible TBI Definite TBI type 1 (grade 1) Definite TBI type 2 (grade 2) Definite severe/moderate TBI Definite mild TBI
 Definite TBI type 2 (grade 2) Definite severe/moderate TBI Definite mild TBI")
22
Three-row TBI

23
1997-2000 ITR data Traumatic Brain Injury

24
Megan

25
Multiple injury And the construction of injury profiles The Center for Trauma and Emergency Medicine Research, Gertner Institute for Epidemiology and Health Policy Research, Israel

26
Multiple injury requires timely care by a number of specialists simultaneously. Multiple injury is often associated with greater severity and mortality. ISS takes into account the contribution of multiple injuries to severity, but does not profile the injury. Summarizing multiple injuries Motivation

27
To create a method for presenting aggregated data on injury patterns in populations. To standardize this method to enable the conduct of comparable studies across populations, time, place etc. Summarizing multiple injuries AIMS

28
Adam Jo Fractured ankle Skull fracture, with an intracranial injury Flail chest multiple diagnoses Single diagnosis

30
Summary report

31
Summarizing multiple injury diagnostic data Select one diagnosis first listed/major multiple diagnoses patients single diagnosis patients

32
Difficulty in assigning the principal diagnosis Limitation of using a Single diagnosis For summarizing multiple injuries Adam Distorts the description of the actual injury Skull fracture, with an intracranial injury Flail chest

33
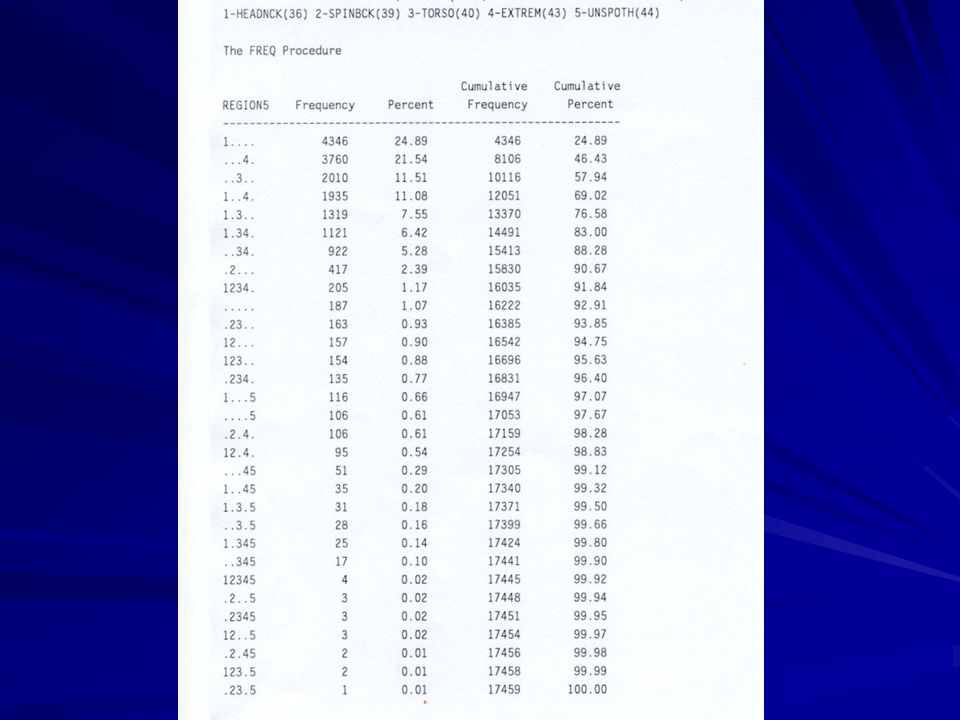
Population: ITR Road Traffic Accidents, 1997-2000, total of 17459 patients Distribution of injuries by body region Single or Multiple?

34
Enable counting all cases with a specific injury Reflect the actual injury pattern in the individual Often associated with greater severity Identification of common profiles of multiple injuries Reasons for using multiple diagnoses For multiple injury patients Multiple diagnoses injury profiles

35
Select one diagnosis first listed/major Create injury profile multiple diagnoses patients Summarizing multiple injury diagnostic data

36
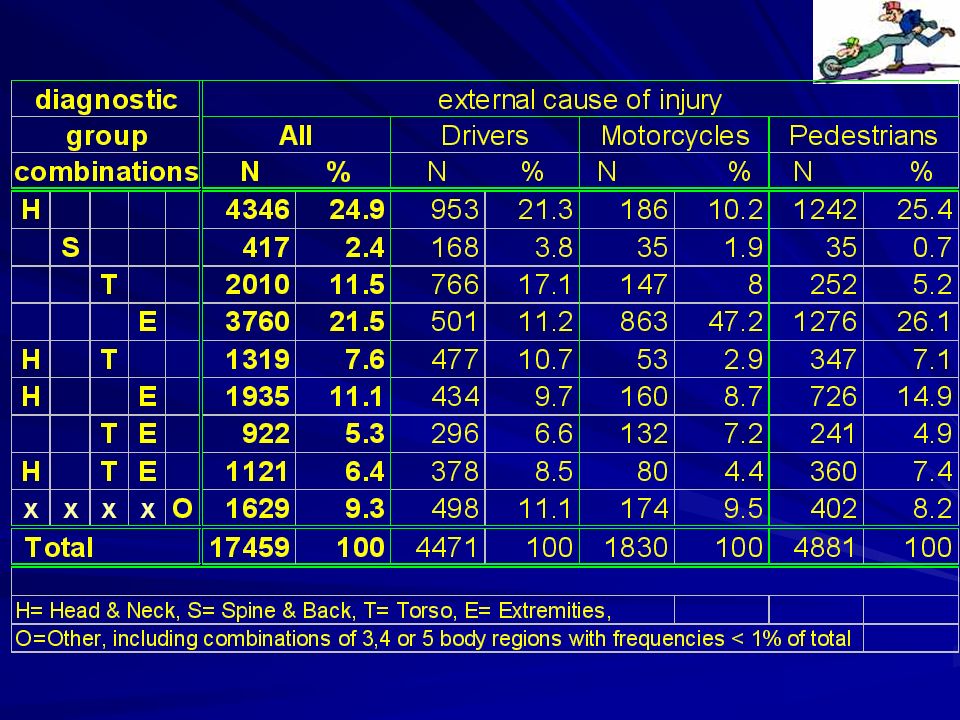
Creating injury profiles Divide body regions into groups Head and Neck H Spine and Back S Torso T Extremities E Other O

38
Legend Head and Neck H Spine and Back S Torso T Extremities E Other multiple O Frequency distribution of groups

39
Characterizing diagnostic groups ISS Inpatient death Duration of inpatient stay External cause of injury etc.

40
Duration of Inpatient stay by diagnostic group combinations Legend Head and Neck H Spine and Back S Torso T Extremities E Other Multiple O Multiple injuriesSingle injuries 75% 25% Median

41
Inpatient death by diagnostic group combinations 4346 1935 2010 922 1319 1121 417 3760 n Multiple injuries Single injuries Inpatient death

43
Summary to date The importance of using multiple injury in describing the injured has been demonstrated. Injury profiles enable standardized comparisons of casemix and outcome between external cause of injury, hospitals and countries. Profiles could also serve for efficient staffing of specialists in multidisciplinary trauma teams. A technique for analyzing multiple injuries was presented using the Barell diagnostic matrix The importance of using multiple injury in describing the injured has been demonstrated. Injury profiles enable standardized comparisons of casemix and outcome between external cause of injury, hospitals and countries. Profiles could also serve for efficient staffing of specialists in multidisciplinary trauma teams.

44
Problems, Limitations and Unresolved issues Definition of multiple Number of combinations Severity measures

Similar presentations









 Guidelines ( )>")








 Version 3.0 Compliant Out-of-Hospital Records Emergency Department Discharge.>")

: Selection of Principal Diagnosis/Additional Diagnoses for Inpatient.>")
