Download presentation
Presentation is loading. Please wait.

1
Martin Dempster 1, Noleen McCorry 2, Emma Brennan 1, Michael Donnelly 3, Liam Murray 3, Brian Johnston 4 1 School of Psychology, Queen’s University Belfast; 2 Marie Curie Cancer Care, Belfast 3 Centre for Public Health, Queen’s University Belfast; 4 Belfast Health & Social Care Trust Project Funded by Action Cancer Facilitated by the Oesophageal Patients’ Association

3
An approach that is relevant to the psychological needs of people who have received a diagnosis of oesophageal cancer and their carers A therapeutic intervention that is not resource-intensive

4
2014201120102007 -2006 Focus groups Interviews Survey at 2 points in time Publication of findings Development of intervention Testing of intervention

6
Beliefs about Illness / Condition Coping Strategies Appraisal of Outcome

7
Psychological Distress Medical Disease course Treatment Pain Stage / grade Demographic Age Psychiatric history Carer Cognitions Interpersonal Social support Personality Optimism Neuroticism Fatalism

8
Psychological Distress Cognitions

9
Research Aim Beliefs Cause Timeline Control Consequences Coherence Ways of Coping Reflect / relax Positive focus Diversion Planning Interpersonal support Levels of: Anxiety and Depression Illness Perceptions Questionnaire - Revised Cancer Coping Questionnaire Hospital Anxiety and Depression Scale Fear of Recurrence Scale

10
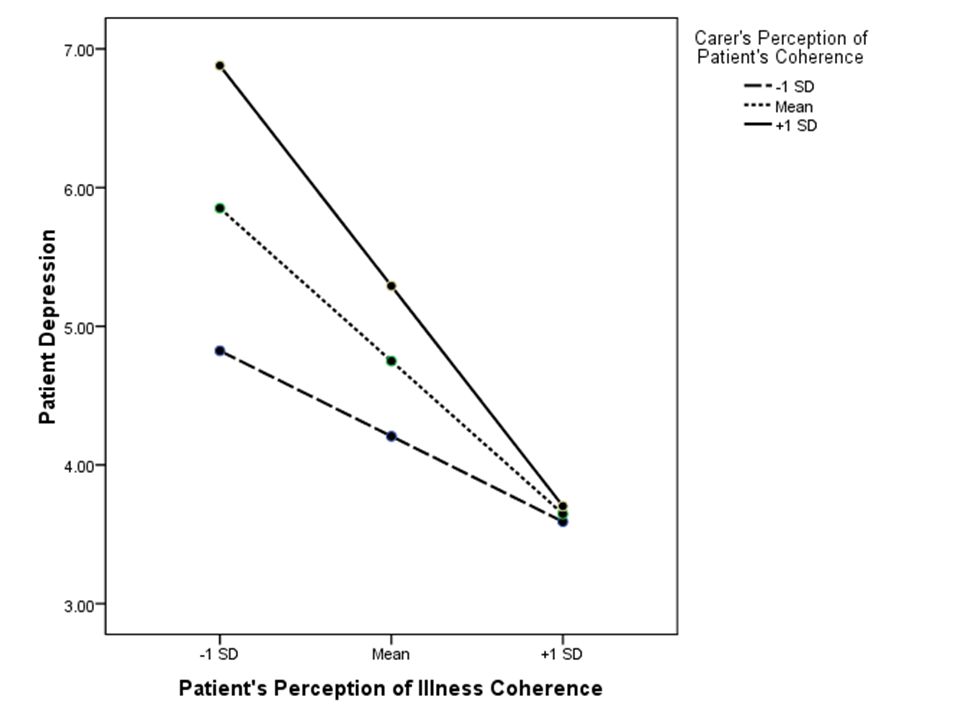
To determine which beliefs / coping strategies are strongest predictors of anxiety/depression among people diagnosed with oesophageal cancer and their carers To determine whether incongruence in carer- patient beliefs is related to distress (i.e. is the relationship between patient beliefs and distress moderated by carer beliefs) To determine whether coping strategies mediate the relationship between beliefs and distress
 To determine whether coping strategies mediate the relationship between beliefs and distress.")
11
Survivors of oesophageal cancer People identified as carers Number458382 Average age6562 Gender66% male75% female 91% were the spouse or partner of the person they cared for

12
Anxiety Depression MildModerateSevere Survivors16%11%8% Carers20%19%11% MildModerateSevere Survivors13%7%3% Carers15%8%2% Similar to head/neck cancer but higher than other cancers

13
Potential Midpoint Survivors Mean (SD) Carers Mean (SD) IPQ Acute/chronic timeline1823.30 (4.68)23.03 (4.80) IPQ Cyclical timeline1412.12 (3.65)12.23 (3.42) IPQ Treatment control1517.17 (3.64)16.77 (3.53) IPQ Emotional cause1512.12 (3.99)12.52 (3.83) IPQ Behavioural cause *1210.43 (3.72)9.98 (3.72) IPQ Externalised cause1214.90 (3.55)15.08 (3.32) IPQ Consequences ***1821.10 (4.82)22.19 (4.66) (for survivor) IPQ Consequences ***1821.10 (4.82)12.65 (3.20) (for self) IPQ Personal control ***1820.05 (4.91)18.90 (4.74) (for survivor) IPQ Personal control ***1820.05 (4.91)16.07 (4.13) (for self) IPQ Illness coherence1519.37 (4.28)19.22 (3.85) (for survivor) IPQ Illness coherence1519.37 (4.28)19.30 (4.04) (for self)
 Carers Mean (SD) IPQ Acute/chronic timeline (4.68)23.03 (4.80) IPQ Cyclical timeline (3.65)12.23 (3.42) IPQ Treatment control (3.64)16.77 (3.53) IPQ Emotional cause (3.99)12.52 (3.83) IPQ Behavioural cause * (3.72)9.98 (3.72) IPQ Externalised cause (3.55)15.08 (3.32) IPQ Consequences *** (4.82)22.19 (4.66) (for survivor) IPQ Consequences *** (4.82)12.65 (3.20) (for self) IPQ Personal control *** (4.91)18.90 (4.74) (for survivor) IPQ Personal control *** (4.91)16.07 (4.13) (for self) IPQ Illness coherence (4.28)19.22 (3.85) (for survivor) IPQ Illness coherence (4.28)19.30 (4.04) (for self)")
14
Anxiety R 2 = 0.57: Medical/demographic variables – 12% Beliefs – 37%; Coping – 7% Depression R 2 = 0.53: Medical/demographic variables – 12% Beliefs – 35%; Coping – 6%

15
Lower Anxiety Older No other illnesses Illness coherence Personal control Positive focus Treatment control (carer) No reflection or diversion ConsequencesInteraction
 No reflection or diversion ConsequencesInteraction")
17
Lower Depression Time since diagnosis No other illnesses No related symptoms Illness coherence Personal control Positive focus Treatment control (carer) No reflection ConsequencesInteraction
 No reflection ConsequencesInteraction")
19
Interventions at the level of the dyad could be useful Focus on consequences, control and understanding of oesophageal cancer and encourage positive focus coping strategies

20
Development of intervention based on these cognitions Possible techniques: normalising the lack of personal control and emotional distress, avoid catastrophising, psychoeducation to improve understanding, positive self-talk Planned feasibility study, leading to trial

Similar presentations














>")
 & Group Therapy Services (GTS)>")







