Download presentation
Presentation is loading. Please wait.

1
Dr.Tahsin.N 3 - 2 - 2012

2
ANTIPLATELETS

3
ASPIRIN

4
Meta-analysis of randomized trials of antiplatelet therapy for prevention of death, MI, and stroke in high-risk patients 195 trials and > 143,000 pts 22% ↓ in odds of vascular death, MI, or stroke with antiplatelet therapy across broad spectrum of clinical presentations that included UA/NSTEMI Similar ↓ in odds of vascular events with aspirin doses of 75-1500 mg daily; <75 mg benefit ↓; dose-dependent ↑ bleeding Antiplatelet Trialists’ Collaboration

5
Secondary prevention trials (pts at high average risk): ― Serious vascular events – RR: 0.81; p<0.0001 ― CHD Death – RR: 0.87; p=0.02 ― Any stroke – RR: 0.81; p=0.002 ― Bleeds – RR: 2.69; p=0.01 Meta-analysis Comparing Use of Long-term ASA vs. Control

6
CLOPIDOGREL

7
12,562 patients within 24 h UA/NSTEMI Placebo vs clopidogrel (LD 300 mg → 75 mg qd) Other meds: aspirin ↓ CV death, MI, or stroke, rate of recurrent ischemia & revasc with clopidogrel ↑ Major (non–life-threatening) bleeding with clopidogrel 23% revasc during initial admission Clopidogrel in Unstable angina to prevent Recurrent ischemic Events (CURE)
 Other meds: aspirin ↓ CV death, MI, or stroke, rate of recurrent ischemia & revasc with clopidogrel ↑ Major (non–life-threatening) bleeding with clopidogrel 23% revasc during initial admission Clopidogrel in Unstable angina to prevent Recurrent ischemic Events (CURE)")
12
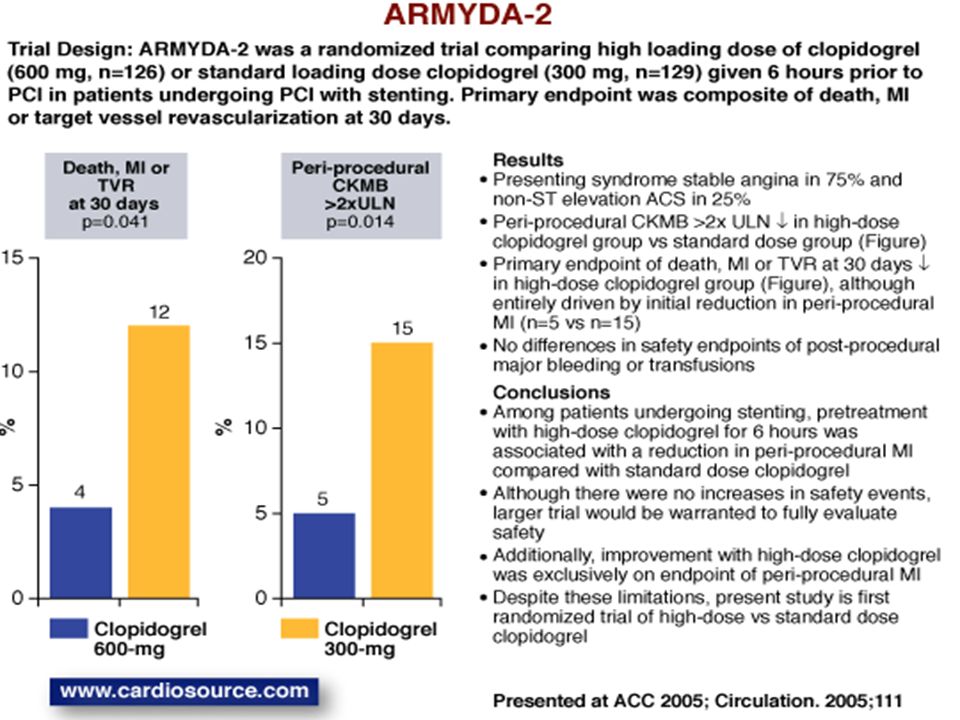
Patients with stable angina or UA/NSTEMI Clopidogrel 600 mg LD (n=126) vs clopidogrel 300 mg LD (n=129) 4 to 8 h before PCI ↓ Death, MI or TVR up to 30 days by 600 mg LD ― Benefit d/t ↓ periprocedural MI Small study of relatively low-risk patients, low use of GP IIb/IIIa Antiplatelet therapy for Reduction of MYocardial Damage during Angioplasty (ARMYDA-2)
 vs clopidogrel 300 mg LD (n=129) 4 to 8 h before PCI ↓ Death, MI or TVR up to 30 days by 600 mg LD ― Benefit d/t ↓ periprocedural MI Small study of relatively low-risk patients, low use of GP IIb/IIIa Antiplatelet therapy for Reduction of MYocardial Damage during Angioplasty (ARMYDA-2)")
14
25,086 pts with ACS, intended PCI, Clopidogrel Double-dose (600 mg d1, 150 mg d2 to 7, then 75 mg daily) vs. standard- dose (300 mg d1, then 75 mg daily) Aspirin High-dose (300 to 325 mg daily) vs. low-dose (75 to 100 mg daily) CURRENT-OASIS 7
 Aspirin High-dose (300 to 325 mg daily) vs. low-dose (75 to 100 mg daily) CURRENT-OASIS 7.")
15
Primary outcome: CV death, MI, or stroke at 30 days – No significant difference in overall trial ― ↑ major bleeding with double-dose clopidogrel vs. standard dose (2.5% vs. 2.0%, HR: 1.24; p=0.012) Primary outcome: CV death, MI, or stroke at 30 days (PCI subgroup) ― ↓ double-dose clopidogrel vs. standard dose, 3.9% vs. 4.5%, p=0.035 ― High-dose and low-dose aspirin did not differ Definite stent thrombosis ↓ with double-dose vs standard dose clopidogrel, 0.7% vs. 1.3%, Adj HR: 0.54; p=0.0001 (PCI subgroup)
 Primary outcome: CV death, MI, or stroke at 30 days (PCI subgroup) ― ↓ double-dose clopidogrel vs. standard dose, 3.9% vs. 4.5%, p=0.035 ― High-dose and low-dose aspirin did not differ Definite stent thrombosis ↓ with double-dose vs standard dose clopidogrel, 0.7% vs. 1.3%, Adj HR: 0.54; p= (PCI subgroup).")
18
Investigated ↓ stent thrombosis with tailored clopidogrel LD 429 PCI pts with low clopidogrel response after 600 mg LD VASP guided pts (up to 3 additional clopidogrel 600 mg LDs) → VASP index <50% VASP guided pts (up to 3 additional clopidogrel 600 mg LDs) → VASP index <50% (vasodilator-stimulated phosphoprotein flow cytometry assays) Stent thrombosis at 1 m significantly ↓ in VASP group vs. control (0.5% vs. 4.2%; p<0.01) MACE higher in control group (8.9% vs. 0.5%; p<0.001) No difference in bleeding rate (2.8% vs 3.7%; p=0.8) Tailored clopidogrel LD according to platelet reactivity monitoring ↓ early stent thrombosis after PCI without ↑ bleeding Tailored Clopidogrel LD According to Platelet Reactivity Monitoring
 MACE higher in control group (8.9% vs. 0.5%; p<0.001) No difference in bleeding rate (2.8% vs 3.7%; p=0.8) Tailored clopidogrel LD according to platelet reactivity monitoring ↓ early stent thrombosis after PCI without ↑ bleeding Tailored Clopidogrel LD According to Platelet Reactivity Monitoring.")
19
RPR measured with VerifyNow P2Y12 assay: clopidogrel non-responsiveness Single 600 mg clopidogrel LD followed by 75 mg of clopidogrel daily (100 to 325 mg ASA daily) 12 m follow-up: 51 ischemic events RPR values ≥240 were significant / independent predictor of: ― CV death (HR: 2.55; p=0.034) ― Nonfatal MI (HR: 3.36; p=0.004) ― No significant association high RPR and TVR RPR to ADP point-of-care assay can detect ACS pts at ↑ risk of CV death and nonfatal MI at 12 m (optimal cutoff value 240 P2Y12 reaction units) Point-of-care Assay: Residual Platelet Reactivity (RPR) to ADP for ACS Patients on DAPT Undergoing PCI/stent
 12 m follow-up: 51 ischemic events RPR values ≥240 were significant / independent predictor of: ― CV death (HR: 2.55; p=0.034) ― Nonfatal MI (HR: 3.36; p=0.004) ― No significant association high RPR and TVR RPR to ADP point-of-care assay can detect ACS pts at ↑ risk of CV death and nonfatal MI at 12 m (optimal cutoff value 240 P2Y12 reaction units) Point-of-care Assay: Residual Platelet Reactivity (RPR) to ADP for ACS Patients on DAPT Undergoing PCI/stent")
20
14 studies, 4,564 CAD pts Residual platelet reactivity (despite clopidogrel treatment) significantly associated with ↑ risk of death and/or thrombotic recurrence (OR: 5.67; p<0.00001) Significant association between residual platelet reactivity and recurrent CV events (clopidogrel non – responsiveness) Meta-analysis: Clopidogrel Non-responsiveness and CV Mortality Post PCI
 significantly associated with ↑ risk of death and/or thrombotic recurrence (OR: 5.67; p< ) Significant association between residual platelet reactivity and recurrent CV events (clopidogrel non – responsiveness) Meta-analysis: Clopidogrel Non-responsiveness and CV Mortality Post PCI")
21
PRASUGREL,CANGRELOR,TICAGRELOR

23
Moderate / high-risk ACS pts (n=13,608) scheduled for PCI randomized to: ― Prasugrel (60 mg LD and 10 mg daily MD) or ― Clopidogrel (300 mg LD and 75 mg daily MD) for 6 to 15 months Primary end point (CV death, nonfatal MI, nonfatal stroke), 9.9% prasugrel vs 12.1% clopidogrel (HR: 0.81; p<0.001) Prasugrel significant ↓ MI (7.4% vs. 9.7%; p<0.001), urgent TVR (2.5% vs. 3.7%), stent thrombosis (1.1% vs. 2.4%) Prasugrel significantly ↓ ischemic events, including stent thrombosis but ↑ risk major bleeding, including fatal bleeding Overall mortality did not differ significantly between groups TRITON-TIMI 38
, urgent TVR (2.5% vs. 3.7%), stent thrombosis (1.1% vs. 2.4%) Prasugrel significantly ↓ ischemic events, including stent thrombosis but ↑ risk major bleeding, including fatal bleeding Overall mortality did not differ significantly between groups TRITON-TIMI 38.")
24
Cumulative Kaplan–Meier Estimates of the Rates of Key Study End Points during the Follow-up Period

25
Results CV death, MI or stroke ↓ with prasugrel vs clopidogrel (Figure) Stent thrombosis also ↓ with prasugrel (1.1% vs. 2.4%, HR 0.48, p < 0.001) TIMI major non-CABG bleeding ↑ with prasugrel than clopidogrel (Figure), Net clinical benefit endpoint (primary+bleeding) favored prasugrel (12.2% vs. 13.9%, HR 0.87, p = 0.004) Conclusions Among patients undergoing planned PCI for ACS, treatment with novel thienopyridine, prasugrel, was associated with reduction in composite of CV death, MI or stroke compared with clopidogrel As would be expected with greater platelet inhibition, bleeding events were significantly higher in prasugrel group, including life-threatening and fatal bleeding Despite this increase, net clinical benefit endpoint incorporating mortality, ischemic events, and major bleeding events, favored prasugrel TRITON-TIMI 38 % Trial Design: TRITON-TIMI 38 was a randomized, double-blind trial of prasugrel (n = 6,813) compared to clopidogrel (n = 6,795) in patients undergoing planned PCI for an acute coronary syndrome (ACS). Primary endpoint was CV death, MI or stroke with a median follow-up of 14.5 months. Prasugrel Clopidogrel Death, MI, or stroke HR 0.81 p < 0.001 Major Bleeding HR 1.32 p = 0.03
 TIMI major non-CABG bleeding ↑ with prasugrel than clopidogrel (Figure), Net clinical benefit endpoint (primary+bleeding) favored prasugrel (12.2% vs. 13.9%, HR 0.87, p = 0.004) Conclusions Among patients undergoing planned PCI for ACS, treatment with novel thienopyridine, prasugrel, was associated with reduction in composite of CV death, MI or stroke compared with clopidogrel As would be expected with greater platelet inhibition, bleeding events were significantly higher in prasugrel group, including life-threatening and fatal bleeding Despite this increase, net clinical benefit endpoint incorporating mortality, ischemic events, and major bleeding events, favored prasugrel TRITON-TIMI 38 % Trial Design: TRITON-TIMI 38 was a randomized, double-blind trial of prasugrel (n = 6,813) compared to clopidogrel (n = 6,795) in patients undergoing planned PCI for an acute coronary syndrome (ACS). Primary endpoint was CV death, MI or stroke with a median follow-up of 14.5 months. Prasugrel Clopidogrel Death, MI, or stroke HR 0.81 p < Major Bleeding HR 1.32 p =")
27
PLATO Death from vascular cause, MI, stroke lower in ticagrelor arm, including in patients undergoing PCI Mortality, stent thrombosis (p = 0.02) ↓ with ticagrelor; stroke rate similar (p = 0.22) No increase in fatal bleeding or overall major bleeding, but higher rate of non- CABG major bleeding (p = 0.03) Trial design: Patients with ACS were randomized to ticagrelor (180 mg loading dose, 90 mg bid thereafter) or clopidogrel (300 mg loading dose, 75 mg daily thereafter). Patients were followed for 12 months. Results Conclusions Cannon CP, et al. Lancet 2010;375:283-93 (p < 0.001) Ticagrelor (n = 9,333) Clopidogrel (n = 9,291) Primary endpoint Ticagrelor superior to clopidogrel for several outcomes including death, MI, and stent thrombosis in patients presenting with ACS Very promising results; reduction in CV mortality notable in the modern era of ACS 0 10 30 % 9.8 11.7 4.5 5.9 % 0 10 5 All-cause mortality (p < 0.001) 20
 Ticagrelor (n = 9,333) Clopidogrel (n = 9,291) Primary endpoint Ticagrelor superior to clopidogrel for several outcomes including death, MI, and stent thrombosis in patients presenting with ACS Very promising results; reduction in CV mortality notable in the modern era of ACS % % All-cause mortality (p < 0.001) 20.")
28
PLATO

31
No TIMI major bleeds in any group Numerical increase in access bleeds requiring medical attention with higher doses of elinogrel compared with clopidogrel Death, MI, stroke, or revascularization: approximately 2.8% of the elinogrel 150 mg group, 4% of the elinogrel 100 mg group, and 1.5% of the clopidogrel group (p = NS) Dyspnea: 12.1%, 15.4%, and 4.3% INNOVATE PCI Trial design: Patients undergoing nonurgent PCI were randomized to one of four groups prior to PCI: 1) elinogrel 80 mg IV, then 150 mg oral twice daily (n = 207); 2) elinogrel 80 mg IV, then 100 mg oral twice daily (n = 201); 3) elinogrel 80 mg IV, then 50 mg oral twice daily; or 4) clopidogrel 300- 600 mg, then 75 mg daily (n = 208). Results Conclusions Among patients undergoing nonurgent PCI, the use of elinogrel is feasible Access site bleeds were numerically higher with increasing doses of elinogrel Similar to ticagrelor, dyspnea was more common with study drug Presented by Dr. Sunil Raul at ESC 2010 (p = NS) Elinogrel 150 mg Elinogrel 100 mg % Death, MI, stroke, or revascularization 2.8 4.0 1.5 Clopidogrel
 Elinogrel 150 mg Elinogrel 100 mg % Death, MI, stroke, or revascularization Clopidogrel.")
32
100 Cilostazol was associated with a significant ↓ in MPA with 5 and 20 μmol/L ADP compared with high-dose clopidogrel Cilostazol was associated with a higher % platelet inhibition (48.4% vs. 35.7%) Clinical endpoints were not measured ACCEL-RESISTANCE Trial design: Patients undergoing PCI, and with high platelet reactivity 12 hours after loading dose of 300 mg clopidogrel were randomized to receive cilostazol with clopidogrel 75 mg daily or clopidogrel 150 mg daily. Patients were followed for 30 days. Results Jeong YH, et al. J Am Coll Cardiol 2009;53:1101-9 Cilostazol + clopidogrel (n = 30) Cilostazol was associated with greater reduction in platelet activity compared with high-dose clopidogrel in patients with high platelet reactivity Clinical endpoints were not available; long-term outcomes need to be assessed as well 57.2 42.1 % (p < 0.001) Conclusions High-dose clopidogrel (n = 30) MPA reduction with 20 μmol/L ADP % platelet inhibition (p = 0.015) 48.4 35.7 100 0 20 40 60 80 0 % 20 40 60 80
 Clinical endpoints were not measured ACCEL-RESISTANCE Trial design: Patients undergoing PCI, and with high platelet reactivity 12 hours after loading dose of 300 mg clopidogrel were randomized to receive cilostazol with clopidogrel 75 mg daily or clopidogrel 150 mg daily. Patients were followed for 30 days. Results Jeong YH, et al. J Am Coll Cardiol 2009;53: Cilostazol + clopidogrel (n = 30) Cilostazol was associated with greater reduction in platelet activity compared with high-dose clopidogrel in patients with high platelet reactivity Clinical endpoints were not available; long-term outcomes need to be assessed as well % (p < 0.001) Conclusions High-dose clopidogrel (n = 30) MPA reduction with 20 μmol/L ADP % platelet inhibition (p = 0.015) %")
33
GP IIb / IIIa INHIBITORS

34
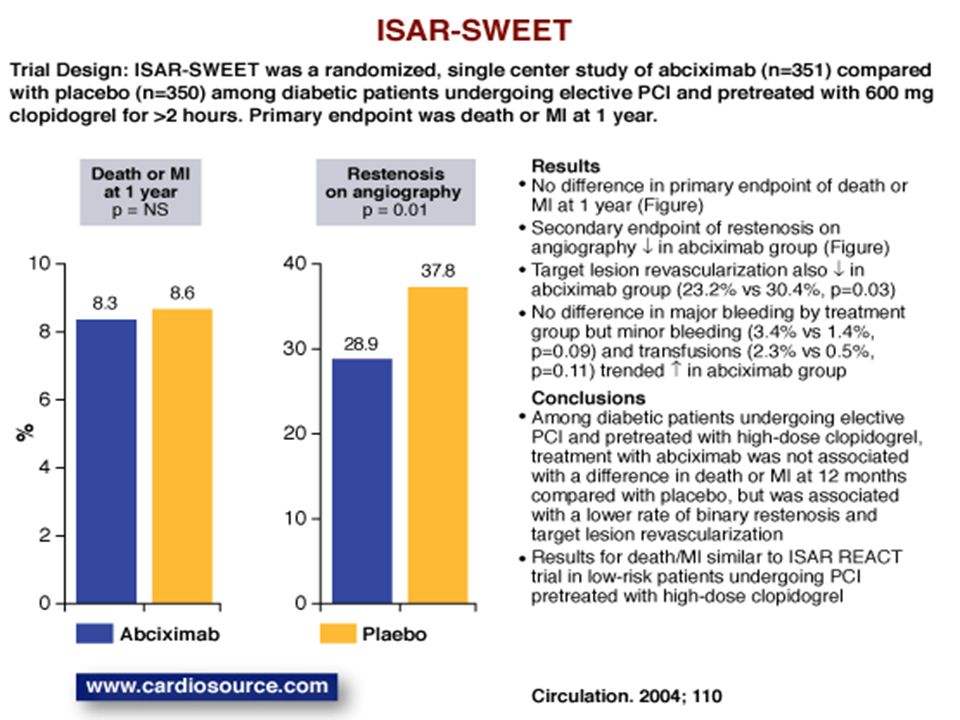
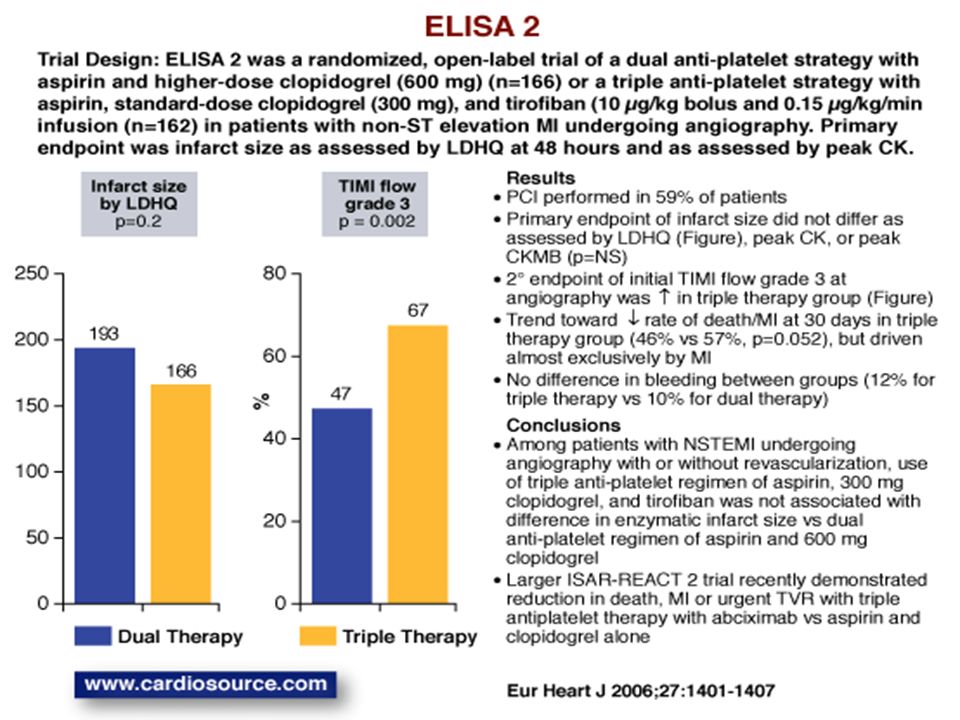
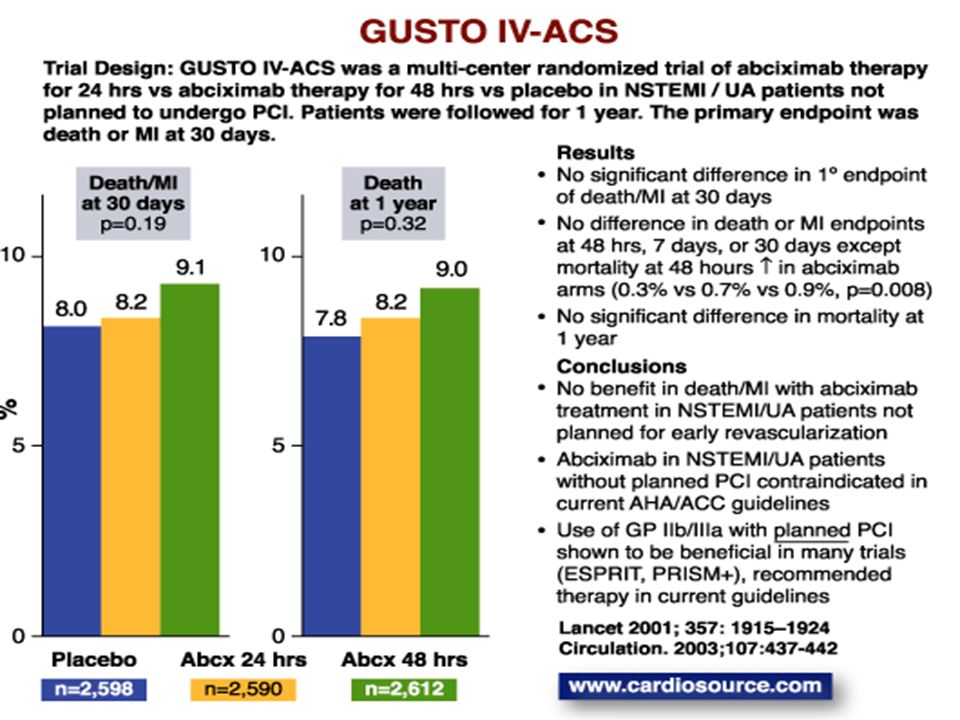
2,022 patients within 48 h high-risk UA/NSTEMI aspirin + clopidogrel + abciximab vs aspirin + clopidogrel + placebo 600 mg LD clopidogrel ≥2 h before PCI → abciximab or placebo ↓ Death, MI, or urgent TVR by 30 d with abciximab - ↓ If cTnT + - no diff if cTnT – No diff major/minor bleeding Recommend: GP IIb/IIIa + clopidogrel if inv strategy used and high risk acs (Class IIa, LOE: B) Intracoronary Stenting and Antithrombotic Regimen– Rapid Early Action for Coronary Treatment (ISAR-REACT)-2
 Intracoronary Stenting and Antithrombotic Regimen– Rapid Early Action for Coronary Treatment (ISAR-REACT)-2")
37
Routine upstream Gp IIb/IIIa inhibitors vs. deferred selective Gp IIb/IIIa use in pts with moderate and high-risk ACS undergoing early, invasive treatment. Composite ischemia at 30 days: 7.1% in upstream vs. 7.9% in deferred (RR: 1.12; p=0.044 for noninferiority; p=0.13 for superiority) 30-day rates of major bleeding: 6.1% in upstream vs. 4.9% in deferred (p<0.001 for noninferiority; p=0.009 for superiority) Net clinical outcomes similar: 11.7% in upstream vs. 11.7% in deferred (p<0.001 for noninferiority; p≤0.93 for superiority) Deferred routine upstream Gp IIb/IIIa inhibitors for selective administration in cath lab only to patients undergoing PCI resulted in ↑ composite ischemia (while not statistically significant), BUT Decreased bleeding risk ACUITY Timing Trial
 30-day rates of major bleeding: 6.1% in upstream vs. 4.9% in deferred (p<0.001 for noninferiority; p=0.009 for superiority) Net clinical outcomes similar: 11.7% in upstream vs. 11.7% in deferred (p<0.001 for noninferiority; p≤0.93 for superiority) Deferred routine upstream Gp IIb/IIIa inhibitors for selective administration in cath lab only to patients undergoing PCI resulted in ↑ composite ischemia (while not statistically significant), BUT Decreased bleeding risk ACUITY Timing Trial.")
38
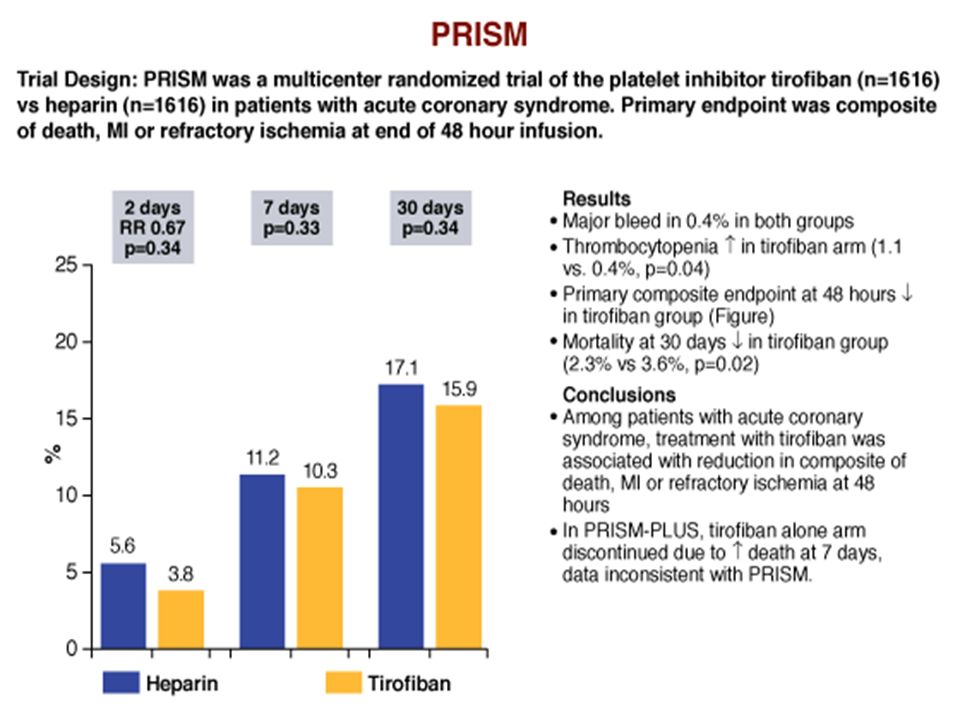
3,232 patients within 24 h UA/NSTEMI Tirofiban vs UFH over 48 h Other meds: aspirin ↓ Death, MI, or refractory ischemia at 48 h & 7 d by tirofiban ― ↓ Death/MI @ 30 d ― No ↑ bleeding; thrombocytopenia ↑ Platelet Receptor Inhibition in Ischemic Syndrome Management (PRISM)
")
40
1,915 patients within 12 h UA/NSTEMI – higher risk Tirofiban alone, UFH alone, or both for 48–108 h. Tirofiban-alone arm discontinued d/t ↑ mortality rate. ↓ Death, MI, or refractory ischemia at 7 d, 30 d & 6 mo by tirofiban + heparin High rate of angio could have contributed to important ↓ in event rates Recommend: Tirofiban + heparin for medical rx or during PCI Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS)
.")
41
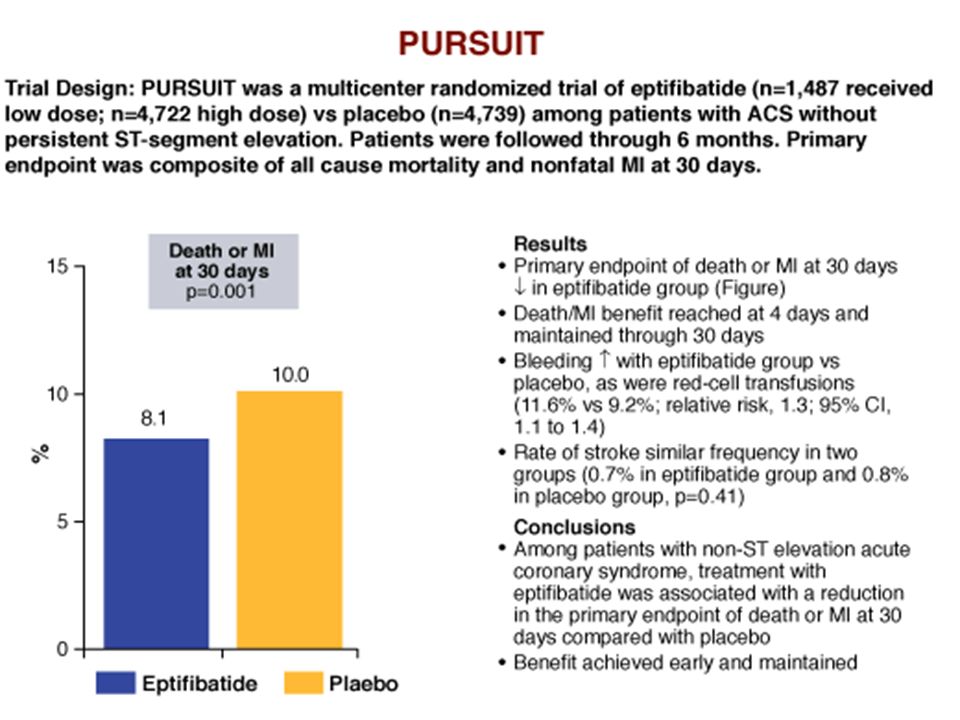
10,948 patients within 24 h UA/NSTEMI Low-dose eptifibatide (n=1,487) vs high-dose eptifibatide (n=4,722) vs placebo (n=4,739) Other meds: aspirin, heparin ↓ Death/MI @ 96 hours, 7 d, 30 d with eptifibatide ― 1.5% ARR 4–30 d ― ↑ major bleeding ― no diff stroke ↑ Event rate in 11% of patients not treated with concomitant heparin Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using InTegrilin (PURSUIT)
 vs high-dose eptifibatide (n=4,722) vs placebo (n=4,739) Other meds: aspirin, heparin ↓ 96 hours, 7 d, 30 d with eptifibatide ― 1.5% ARR 4–30 d ― ↑ major bleeding ― no diff stroke ↑ Event rate in 11% of patients not treated with concomitant heparin Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using InTegrilin (PURSUIT)")
43
9492 patients with NSTEMI ACS Early routine vs. delayed, provisional eptifibatide Primary end point: death, MI, recurrent ischemia requiring urgent revascularization, or thrombotic complication during PCI that required bolus therapy ― 9.3% early eptifibatide vs. 10.0% delayed eptifibatide Early versus Delayed Provisional Eptifibatide in Acute Myocardial Infarction EARLY ACS

44
Secondary end point: death or MI within first 30 d ― 11.2% early eptifibatide vs. 12.3% delayed eptifibatide Eptifibatide 12 h or more before angiography not superior to provisional use after angiography ― associated risk non-life-threatening bleeding, need for transfusion EARLY ACS

46
Thank you ……to be continued Thank you ……to be continued

47
MCQs

48
Match the trial with drug 1.ISAR REACT 2 2.ISAR CHOICE 3.JUMBO TIMI 26 4.PLATO 5.INNOVATE PCI 6.PRISM 7.PURSUIT a) CLOPIDOGREL b) PRASUGREL c) TICAGRELOR d) ELINOGREL e) ABSCIXIMAB f) EPTIFIBATIDE g) TIROFIBAN
 CLOPIDOGREL b) PRASUGREL c) TICAGRELOR d) ELINOGREL e) ABSCIXIMAB f) EPTIFIBATIDE g) TIROFIBAN")
49
8. Vascular death, MI, or stroke are decreased with antiplatelet therapy by a) 18% b) 22% c) 26% d) 30%
 18% b) 22% c) 26% d) 30%.")
50
9. All the following trials compared 600mg clopidogrel with 300mg except a)CURE b)ISAR CHOICE c)ARMYDA 2 d)CURRENT OASIS 7
CURE b)ISAR CHOICE c)ARMYDA 2 d)CURRENT OASIS 7.")
51
10. Regarding TRITON TIMI38 all the following statements are true EXCEPT a)Prasugrel significant ↓ MI & urgent TVR b)Prasugrel significantly ↓ ischemic events, including stent thrombosis c)Prasugrel ↑ risk of major bleeding, including fatal bleeding d)Prasugrel reduced overall mortality
Prasugrel significant ↓ MI & urgent TVR b)Prasugrel significantly ↓ ischemic events, including stent thrombosis c)Prasugrel ↑ risk of major bleeding, including fatal bleeding d)Prasugrel reduced overall mortality.")
52
11. Regarding PLATO trial all are true EXCEPT Ticagrelor compared to clopidogrel a.Decreased mortality b.Increased overall bleeding c.Caused significant dyspnoae d.Reversible

53
12. Regarding Pursuit trial All are true EXCEPT Eptifibatide Caused a)1.5% Absolute reduction b)↑ major bleeding c)Increased stroke d)One of the largest GP IIb / IIIa trial
1.5% Absolute reduction b)↑ major bleeding c)Increased stroke d)One of the largest GP IIb / IIIa trial.")
54
ANSWERS

55
Match the trial with drug 1.ISAR REACT 2 2.ISAR CHOICE 3.JUMBO TIMI 26 4.PLATO 5.INNOVATE PCI 6.PRISM 7.PURSUIT a) CLOPIDOGREL b) PRASUGREL c) TICAGRELOR d) ELINOGREL e) ABSCIXIMAB f) EPTIFIBATIDE g) TIROFIBAN
 CLOPIDOGREL b) PRASUGREL c) TICAGRELOR d) ELINOGREL e) ABSCIXIMAB f) EPTIFIBATIDE g) TIROFIBAN")
56
8. Vascular death, MI, or stroke are decreased with antiplatelet therapy by a) 18% b) 22% c) 26% d) 30%
 18% b) 22% c) 26% d) 30%.")
57
9. All the following trials compared 600mg clopidogrel with 300mg except a)CURE b)ISAR CHOICE c)ARMYDA 2 d)CURRENT OASIS 7
CURE b)ISAR CHOICE c)ARMYDA 2 d)CURRENT OASIS 7.")
58
10. Regarding TRITON TIMI38 all the following statements are true EXCEPT a)Prasugrel significant ↓ MI & urgent TVR b)Prasugrel significantly ↓ ischemic events, including stent thrombosis c)Prasugrel ↑ risk of major bleeding, including fatal bleeding d)Prasugrel reduced overall mortality
Prasugrel significant ↓ MI & urgent TVR b)Prasugrel significantly ↓ ischemic events, including stent thrombosis c)Prasugrel ↑ risk of major bleeding, including fatal bleeding d)Prasugrel reduced overall mortality.")
59
11. Regarding PLATO trial all are true EXCEPT Ticagrelor compared to clopidogrel a.Decreased mortality b.Increased overall bleeding c.Caused significant dyspnoae d.Reversible

60
12. Regarding PURSUIT trial All are true EXCEPT Eptifibatide Caused a)1.5% Absolute reduction b)↑ major bleeding c)Increased stroke d)One of the largest GP IIb / IIIa trial
1.5% Absolute reduction b)↑ major bleeding c)Increased stroke d)One of the largest GP IIb / IIIa trial.")
61
Dr.Tahsin.N 10 - 2 - 2012

62
Anticoagulants

63
HEPARIN & LMWH

64
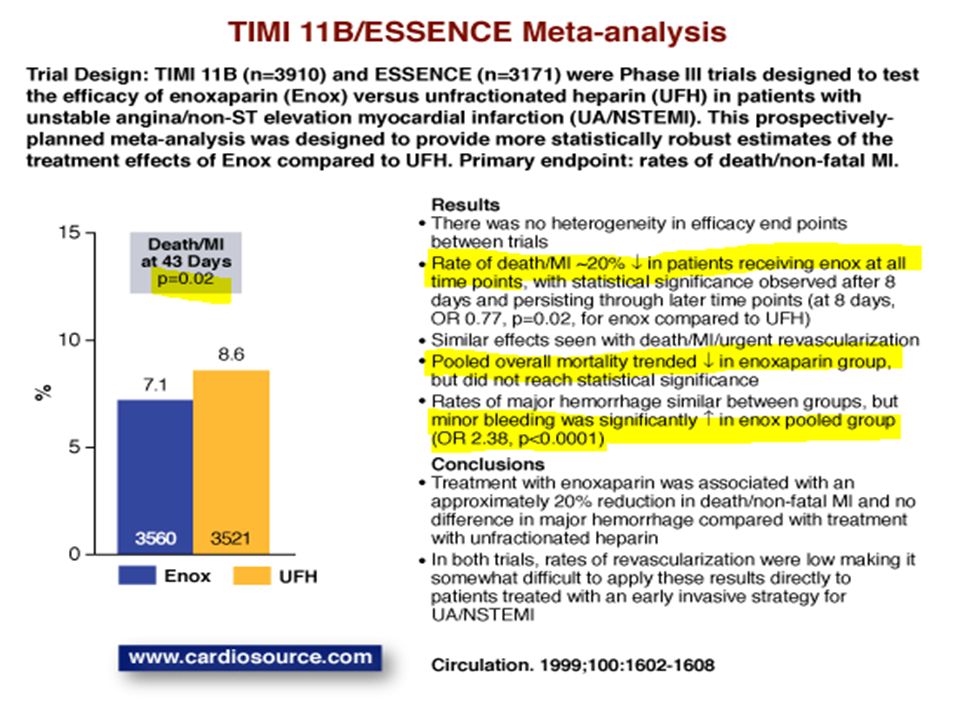
3,171 patients within 24 h UA/NSTEMI Enoxaparin vs UFH Other meds: aspirin ↓ Death, MI or recurrent angina for enox @ 14 d, 30d and 1 y ― minor bleeding ↑ ― major bleeding ↔ Efficacy and Safety of Subcutaneous Enoxaparin in Non-Q-Wave Coronary Events (ESSENCE) trial
 trial")
65
3,910 patients within 24 h UA/NSTEMI Enoxaparin vs UFH Other meds: aspirin ↓ Death, MI or urgent revasc for enox @ 48 h, 8 d, 14 d, & 43 d ↑ major & minor bleeding (inhosp) with enox Thrombolysis In Myocardial Ischemia trial, phase 11B (TIMI 11B)
 with enox Thrombolysis In Myocardial Ischemia trial, phase 11B (TIMI 11B)")
67
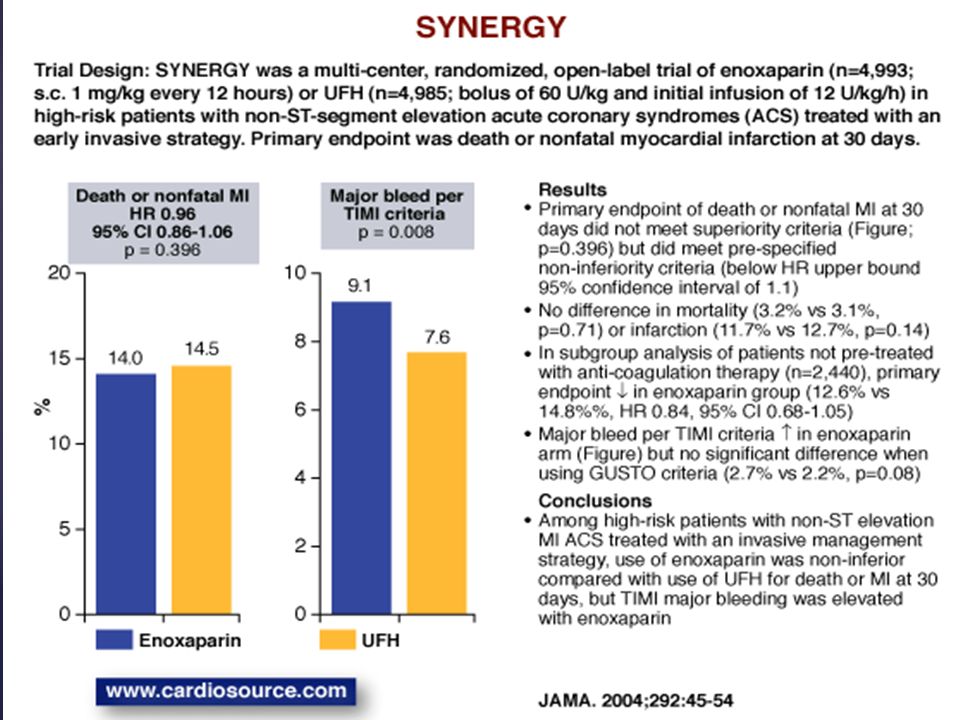
Superior Yield of the New strategy of Enoxaparin, Revascularization and Gp IIb/IIIa Inhibitors (SYNERGY) 9,978 patients within 24 h high-risk UA/NSTEMI Enoxaparin vs UFH → early inv strategy Other meds: aspirin, clopidogrel, GP IIb/IIIa @ physician discretion Enox noninferior for death/MI @ 30 d, 6 mo 1 y ↑ Major bleeding with enox ― ? due to crossover to UFH @ time of PCI

68
SYNERGY Primary Outcomes Absolute Risk Reduction0.5 Hazard Ratio0.96 95% CI0.86–1.06 p0.40 Freedom from Death/MI 0.8 0.85 0.9 0.95 1.0 051015202530 Days from Randomization Kaplan Meier Curve UFH Enoxaparin Reprinted with permission from Ferguson JJ, et al. JAMA 2004;292:45–54.

70
525 patients within 24 h UA/NSTEMI Enoxaparin vs UFH Other meds: aspirin, tirofiban LD 0.4 mcg/kg over 30 min → 0.1 mcg/kg/min No ↓ death/MI during first 30 d ― Trend to lower event rates with enox No ↓ major/minor bleeding Antithrombotic Combination Using Tirofiban and Enoxaparin (ACUTE II)
")
71
3,987 patients within 24 h UA/NSTEMI on aspirin & tirofiban Enoxaparin vs UFH Coronary angio in 60% of pts No ↓ all-cause mortality, MI or refractory ischemia w/in 7 d by enox ― Nonsig trend to ↓ ischemic events with enox ↑ Major bleeding with enox Aggrastat to Zocor (A to Z)
")
72
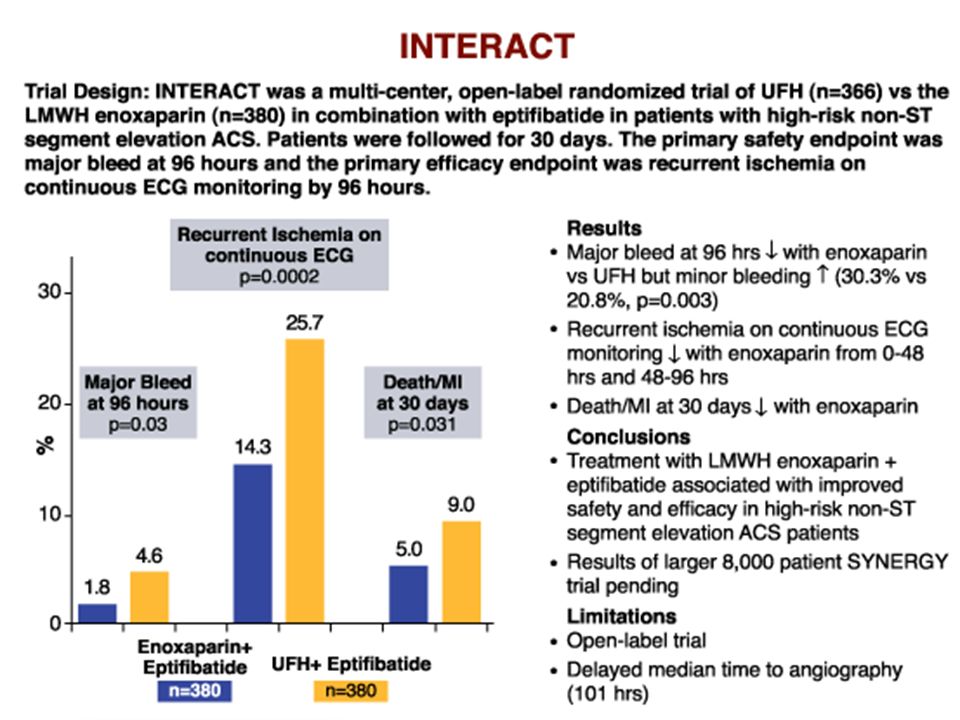
746 patients within 24 h high-risk UA/NSTEMI Enoxaparin vs UFH Other meds: aspirin, eptifibatide 180 mcg/kg IV bolus → 2.0 mcg/kg/min infusion for 48 hours ↓ Death/MI for enox @ 30 d Minor bleeding - ↑ for enox @ 96 h, no diff by 30 d Major bleeding - ↓ for enox @ 96 h (1 o safety endpoint) INTegrilin and Enoxaparin Randomized Assessment of Acute Coronary syndrome Treatment (INTERACT)
 INTegrilin and Enoxaparin Randomized Assessment of Acute Coronary syndrome Treatment (INTERACT)")
74
Patients within 48 h UA/NSTEMI Early inv vs conserv & dalteparin vs placebo 3048 patients → dalteparin for 5–7 d → 2457 continued dalteparin/placebo & received either inv or conserv rx strategy Meds: aspirin, β-blockers unless contraindicated No ↓ death/MI @ 3 mo by dalteparin ↓ Death/MI @ 6 mo, 1 y & 5 y for inv strategy Fragmin during Instability in Coronary Artery Disease (FRISC-2)
")
77
Meta analysis Enoxaparin Vs UFH - DEATH

78
Meta analysis Enoxaparin Vs UFH - MI

79
Meta analysis Enoxaparin Vs UFH – Major bleed

80
FONDAPARINUX

82
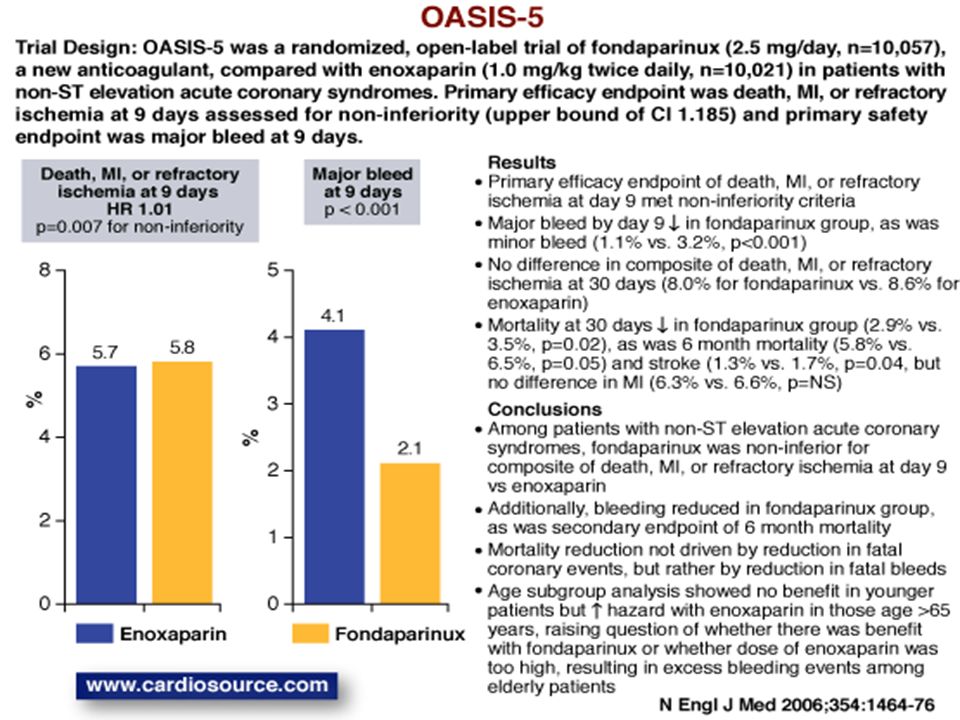
Fondaparinux (2.5 mg/day, n=10,057) vs enoxaparin (1.0 mg/kg BID, n=10,021) in UA/NSTEMI patients ― Enox patients undergoing PCI → UFH if last dose of enox > 6 h before PCI Other meds: aspirin, clopidogrel, GP IIb/IIIa @ investigator discretion No ↓ death, MI or refractory ischemia @ 9 d by fonda ― Non inferiority criteria met ↓ Major bleeding with fonda ↓ Death @ 30 d and 180 d and ↓ death, MI and stroke @ 180 d with fonda ↑ Catheter-assoc thrombus with fonda Organization to Assess Strategies for Ischaemic Syndromes (OASIS-5)
 vs enoxaparin (1.0 mg/kg BID, n=10,021) in UA/NSTEMI patients ― Enox patients undergoing PCI → UFH if last dose of enox > 6 h before PCI Other meds: aspirin, clopidogrel, GP investigator discretion No ↓ death, MI or refractory 9 d by fonda ― Non inferiority criteria met ↓ Major bleeding with fonda ↓ 30 d and 180 d and ↓ death, MI and 180 d with fonda ↑ Catheter-assoc thrombus with fonda Organization to Assess Strategies for Ischaemic Syndromes (OASIS-5)")
83
OASIS 5 Cumulative Risk of Death, MI, or Refractory Ischemia *p for noninferiority; †p for superiority. Yusuf S, et al. N Engl J Med 2006;354:1464–76. 5.7 4.1 9.0 5.8 2.2 7.3 0 1 2 3 4 5 6 7 8 9 10 OASIS 5 Death, MI, or refractory ischemia at 9 days OASIS 5 Major bleeding at 9 days OASIS 5 Composite primary outcome and major bleeding at 9 days Enoxaparin Fondaparinux Absolute Risk Reduction-0.11.91.7 Hazard Ratio1.010.520.81 Confidence Interval0.90–1.130.44–0.610.73–0.89 p0.007*< 0.001†< 0.001†

85
Major bleeds/minor bleeds/vascular access site complications at 48 hours: 4.7% of the low-dose heparin group vs. 5.8% of the standard-dose heparin group (p = 0.27) Death, MI, or revascularization: 4.5% vs. 2.9% (p = 0.06), respectively Stent thrombosis: 1.2% vs. 0.5% (p = 0.11), respectively FUTURA/OASIS-8 Trial design: NSTEMI patients initially treated with fondaparinux 2.5 mg SQ were randomized to unfractionated heparin 50 U/kg regardless of glycoprotein IIb/IIIa inhibitor use (n = 1,024) vs. unfractionated heparin 60 U/kg with glycoprotein IIb/IIIa inhibitor or 85 U/kg without glycoprotein IIb/IIIa inhibitor (n = 1,002). Results Conclusions Among ACS patients initially treated with fondaparinux, PCI can be safely performed with the addition of unfractionated heparin Low-dose and standard-dose heparin had the same frequency of bleeding events Low-dose heparin therapy was associated with a marginally significant increase in ischemic events FUTURA/OASIS-8 Trial Group. JAMA 2010;Aug 31:[Epub] (p = 0.27) Low-dose heparin Standard-dose heparin % Major/minor bleed, or vascular complication 4.7 4.5 5.8 2.9 (p = 0.06) Death, MI, or revascularization
 Death, MI, or revascularization: 4.5% vs. 2.9% (p = 0.06), respectively Stent thrombosis: 1.2% vs. 0.5% (p = 0.11), respectively FUTURA/OASIS-8 Trial design: NSTEMI patients initially treated with fondaparinux 2.5 mg SQ were randomized to unfractionated heparin 50 U/kg regardless of glycoprotein IIb/IIIa inhibitor use (n = 1,024) vs. unfractionated heparin 60 U/kg with glycoprotein IIb/IIIa inhibitor or 85 U/kg without glycoprotein IIb/IIIa inhibitor (n = 1,002). Results Conclusions Among ACS patients initially treated with fondaparinux, PCI can be safely performed with the addition of unfractionated heparin Low-dose and standard-dose heparin had the same frequency of bleeding events Low-dose heparin therapy was associated with a marginally significant increase in ischemic events FUTURA/OASIS-8 Trial Group. JAMA 2010;Aug 31:[Epub] (p = 0.27) Low-dose heparin Standard-dose heparin % Major/minor bleed, or vascular complication (p = 0.06) Death, MI, or revascularization.")
86
BIVALIRUDIN

87
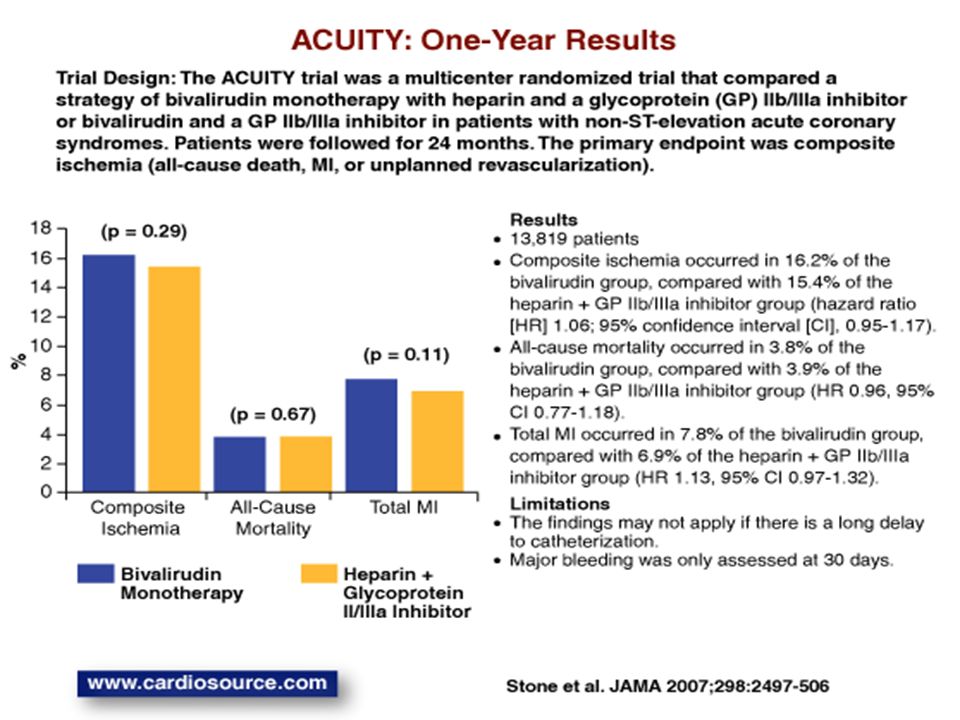
Within 24 h UA/NSTEMI → heparin (enox/UFH) ± upstream GP IIb/IIIa (n=4603) vs bivalirudin (bival) ± upstream GP IIb/IIIa (n=4604) vs bival alone + provisional GP IIb/IIIa (n=4612) Compared to heparin + GP IIb/IIa: ― Bival + GP IIb/IIIa noninferior for composite ischemia, major bleeding & net clinical outcomes @ 30 d ― Bival alone noninferior for composite ischemia; ↓ major bleeding; ↓ net clinical outcomes @ 30 d Acute Catheterization and Urgent Intervention Triage strategY (ACUITY)
 ± upstream GP IIb/IIIa (n=4603) vs bivalirudin (bival) ± upstream GP IIb/IIIa (n=4604) vs bival alone + provisional GP IIb/IIIa (n=4612) Compared to heparin + GP IIb/IIa: ― Bival + GP IIb/IIIa noninferior for composite ischemia, major bleeding & net clinical 30 d ― Bival alone noninferior for composite ischemia; ↓ major bleeding; ↓ net clinical 30 d Acute Catheterization and Urgent Intervention Triage strategY (ACUITY)")
88
7.3 5.7 11.7 7.7 5.3 11.8 0 2 4 6 8 10 12 14 ACUITY Composite ischemia endpoint at 30 days ACUITY Major bleeding at 30 days ACUITY Net clinical outcome at 30 days UFH or Enoxaparin + GP IIb/IIIa Bivalirudin + GP IIb/IIIa ACUITY Clinical Outcomes at 30 d Absolute Risk Reduction-0.40.4 -0.1 Hazard Ratio1.070.93 1.01 95% CI0.92–1.230.78–1.10 0.90–1.12 p0.007*< 0.001* < 0.001*

89
ACUITY Composite Ischemia & Bleeding Outcomes Absolute Risk Reduction-0.50.3-2.0 2.7 Hazard Ratio1.080.971.29 0.53 95% CI0.93–1.240.80–1.171.03–1.63 0.43–0.65 p0.320.054 (for interaction) < 0.001 7.3 7.1 5.7 7.8 7.0 9.1 3.0 0 1 2 3 4 5 6 7 8 9 10 ACUITY Composite ischemia endpoint at 30 days Ischemia endpoint by thienopyridine loading before angiography or PCI YES Ischemia endpoint by thienopyridine loading before angiography or PCI No ACUITY Major bleeding at 30 days UFH + GP IIb/IIIa Bivalirudin alone
 < ACUITY Composite ischemia endpoint at 30 days Ischemia endpoint by thienopyridine loading before angiography or PCI YES Ischemia endpoint by thienopyridine loading before angiography or PCI No ACUITY Major bleeding at 30 days UFH + GP IIb/IIIa Bivalirudin alone")
92
ISAR-REACT 3 Primary endpoint: death, MI, urgent target vessel revascularization, or in-hospital major bleeding was similar between the bivalirudin (8.3%) and UFH (8.7%) arms (p = 0.57) Bleeding significantly ↓ with bivalirudin compared with UFH: major (33%), minor (31%) Trial design: Troponin-negative patients undergoing PCI were randomized to either bivalirudin or unfractionated heparin (UFH), after pretreatment with 600 mg of clopidogrel. Clinical outcomes were evaluated at 30 days. Results Conclusions Bivalirudin is not superior to UFH as adjunct anticoagulation therapy for troponin-negative patients undergoing PCI, who were pretreated with 600 mg of clopidogrel Bleeding was significantly reduced with bivalirudin compared with UFH Presented by Dr. Adnan Kastrati at SCAI-ACC i2 Summit/ACC 2008 (p = 0.57) Bivalirudin (n = 2,289) UFH (n = 2,281) (p = 0.008) Composite endpointMajor bleeding % 0 1 2 4 3.14.6 3 5 1 9 6 0 2 3 4 5 7 8 10 8.38.7 %
 Bivalirudin (n = 2,289) UFH (n = 2,281) (p = 0.008) Composite endpointMajor bleeding % %.")
95
ISAR-REACT 4 Death, large recurrent MI, urgent target vessel revascularization (TVR), or major bleeding: 10.9% of the heparin/abciximab vs. 11.0% of the bivalirudin group (p = 0.94) Death, any MI, or urgent TVR: 12.8% vs. 13.4% (p = 0.76) Major bleeding: 4.6% vs. 2.6% (p = 0.02) Trial design: Patients with NSTEMI undergoing PCI were randomized to unfractionated heparin/abciximab (n = 861) vs. bivalirudin alone (n = 860). Follow-up was 30 days. Results Conclusions Among patients with NSTEMI undergoing PCI, the use of bivalirudin alone results in similar ischemic events and less bleeding compared with unfractionated heparin/abciximab Kastrati A, et al. N Engl J Med 2011;Nov 13:[Epub] (p = 0.94) Unfractionated heparin/abciximab % 10.911.0 Death, large MI, urgent TVR, or major bleeding Bivalirudin alone
 Death, any MI, or urgent TVR: 12.8% vs. 13.4% (p = 0.76) Major bleeding: 4.6% vs. 2.6% (p = 0.02) Trial design: Patients with NSTEMI undergoing PCI were randomized to unfractionated heparin/abciximab (n = 861) vs. bivalirudin alone (n = 860). Follow-up was 30 days. Results Conclusions Among patients with NSTEMI undergoing PCI, the use of bivalirudin alone results in similar ischemic events and less bleeding compared with unfractionated heparin/abciximab Kastrati A, et al. N Engl J Med 2011;Nov 13:[Epub] (p = 0.94) Unfractionated heparin/abciximab % Death, large MI, urgent TVR, or major bleeding Bivalirudin alone.")
96
{

97
ORAL ANTICOAGULANTS

98
Warfarin (INR 2.8-4.2) vs. aspirin (160 mg/day) vs. Warfarin ( INR 2.0 -2.5) and aspirin 75 mg/day for the secondary prevention of myocardial infarction Primary outcome - composite of death, nonfatal MI or thromboembolic stroke Major nonfatal bleeding - significantly higher with warfarin compared to aspirin 0.62% Vs 0.17 % (P<0.001) No Clopidogrel use WARIS-II
 and aspirin 75 mg/day for the secondary prevention of myocardial infarction Primary outcome - composite of death, nonfatal MI or thromboembolic stroke Major nonfatal bleeding - significantly higher with warfarin compared to aspirin 0.62% Vs 0.17 % (P<0.001) No Clopidogrel use WARIS-II.")
99
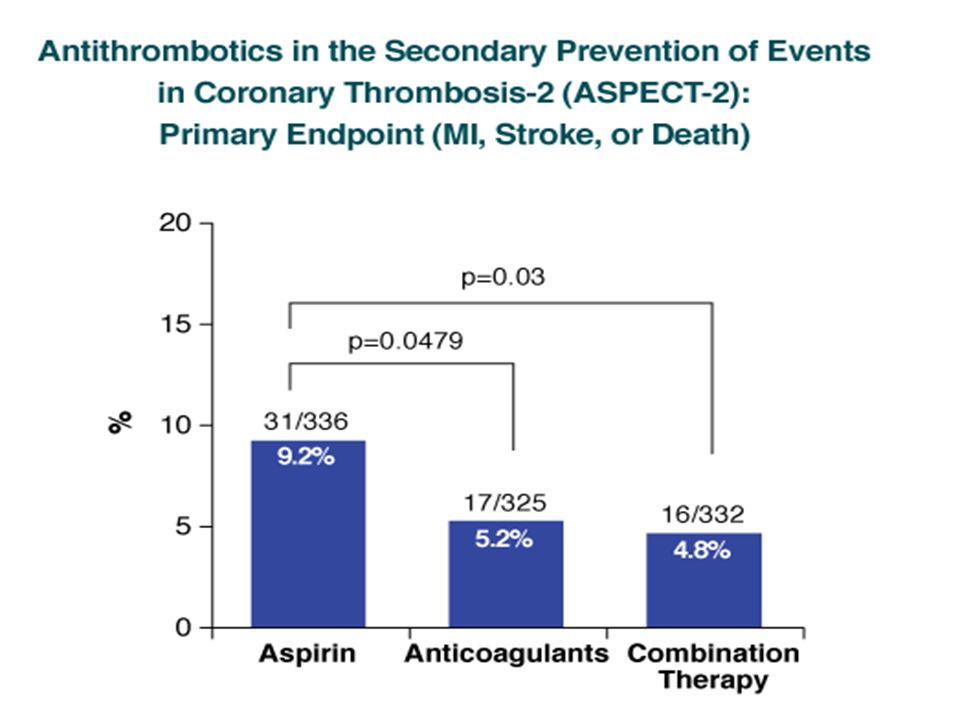
Low-dose aspirin (n=336) Vs High-intensity oral anticoagulation (n=325) INR 3 – 4 Vs Combined low-dose aspirin and moderate intensity oral anticoagulation INR 2 – 2.25 (n=332) 26 months Primary composite endpoint was first occurrence of MI, stroke or death Major bleeding was similar in all three groups (<2%) Minor bleeding was increased in the combination therapy (5% vs. 15%, 3.13 [1.82- 5.37]p=<0.0001) ASPECT-2
 ASPECT-2.")
102
(p < 0.001) 10 4.3 3.5 % Major or clinically significant minor bleeding 0 7.9 7.8 2.2 5 RE-DEEM Major or clinically significant minor bleeding: 3.5% of the 50 mg group, 4.3% of the 75 mg group, 7.9% of the 110 mg group, 7.8% of the 150 mg group, and 2.2% with placebo TIMI major bleeding: 0.3%, 0%, 1.2%, 0.3%, 0.3%, respectively Cardiovascular death, MI, or stroke: 4.6%, 4.9%, 3.0%, 3.5%, and 3.8% (p = NS), respectively Trial design: After STEMI or NSTEMI, patients on dual antiplatelet therapy were randomized to dabigatran twice daily: 50 mg (n = 369), 75 mg (n = 368), 110 mg (n = 406), 150 mg (n = 347), or placebo (n = 371). Follow-up was 6 months. Results Conclusions In this phase II trial of patients with STEMI or NSTEMI, the addition of dabigatran to dual antiplatelet therapy increased the risk of bleeding in a dose-dependent manner Phase III trials are awaited Oldgren J, et al. Eur Heart J 2011;May 7:[Epub] 150 mg 110 mg 50 mg75 mg Placebo

103
APPRAISE ISTH major or CRNM bleeding: 7.9% for 10 mg apixaban, 5.7% for 5 mg apixaban, 3% for placebo Death, MI, recurrent ischemia, or stroke: 6.0%, 7.6%, 8.7% (p = 0.07 for high dose vs. placebo and p = 0.21 for low dose vs. placebo), respectively Trial design: Patients recovering from an ACS were randomized to apixaban 10 mg daily (n = 318), apixaban 2.5 mg twice daily (n = 317), or placebo (n = 611). Study medications were administered for 6 months. Results Conclusions This dose-finding study reveals that bleeding is increased among patients with a recent ACS with higher doses of apixaban compared with placebo Although this study was not powered for efficacy, adverse events appeared to be lowest with 10 mg apixaban APPRAISE Investigators. Circulation 2009;May 26:[Epub] (p = 0.005 for high dose vs. placebo) (p = 0.09 for low dose vs. placebo) Apixaban 10 mg Apixaban 5 mg % Placebo 7.9 5.7 3.0 ISTH major or CRNM bleeding
, respectively Trial design: Patients recovering from an ACS were randomized to apixaban 10 mg daily (n = 318), apixaban 2.5 mg twice daily (n = 317), or placebo (n = 611). Study medications were administered for 6 months. Results Conclusions This dose-finding study reveals that bleeding is increased among patients with a recent ACS with higher doses of apixaban compared with placebo Although this study was not powered for efficacy, adverse events appeared to be lowest with 10 mg apixaban APPRAISE Investigators. Circulation 2009;May 26:[Epub] (p = for high dose vs. placebo) (p = 0.09 for low dose vs. placebo) Apixaban 10 mg Apixaban 5 mg % Placebo ISTH major or CRNM bleeding.")
104
Apixaban with Antiplatelet Therapy after Acute Coronary Syndrome APPRAISE 2 In a randomized trial, patients with an acute coronary syndrome were assigned to receive apixaban or placebo in addition to standard therapy.In a randomized trial, patients with an acute coronary syndrome were assigned to receive apixaban or placebo in addition to standard therapy. The apixaban group had a higher rate of TIMI major bleeding and no significant reduction in recurrent ischemic events.The apixaban group had a higher rate of TIMI major bleeding and no significant reduction in recurrent ischemic events.

105
Rivaroxaban in Patients with a Recent Acute Coronary Syndrome ATLAS ACS TIMI 51 In patients with ACS, low doses of rivaroxaban were effective in reducing the primary end point of death from cardiovascular causes, MI or stroke.In patients with ACS, low doses of rivaroxaban were effective in reducing the primary end point of death from cardiovascular causes, MI or stroke. Rivaroxaban also reduced overall mortality although there was more bleeding.Rivaroxaban also reduced overall mortality although there was more bleeding. Rivaroxaban increased the risk of major bleeding and intracranial hemorrhage but not the risk of fatal bleeding.Rivaroxaban increased the risk of major bleeding and intracranial hemorrhage but not the risk of fatal bleeding.

106
RUBY-1 Primary endpoint (major and clinically relevant non- major bleeding) demonstrated a dose-response relationship for darexaban, with higher bleeding with BID regimens for the same dose (p = 0.009) Composite efficacy outcome noted numerically higher event rates for darexaban as compared with placebo (4.4% for placebo vs. 3.8% vs. 3.8% vs. 6.3% vs. 6.4% vs. 5.9% vs. 7.8%; p > 0.05). Trial design: Patients with recent ACS were randomized to receive in a 1:1:1:1:1:1:1 fashion either placebo or darexaban 5 mg BID, 10 mg QD, 15 mg BID, 30 mg QD, 30 mg BID, or 60 mg QD. Patients were followed for 6 months. Results Conclusions Steg G, et al. Eur Heart J 2011;Aug 30:[Epub] (p = 0.009) In this phase II trial, darexaban, an oral anti-Xa agent, was associated with increased bleeding without an improvement in ischemic outcomes in patients with ACS already on aspirin and clopidogrel Similar results were noted with other anti-Xa agents such as apixaban 3.1 6.8 10 Major and clinically relevant bleeding 0 20 % Placebo n = 319 15 BID n = 159 5 BID n = 159 10 QD n = 159 5.6 7.5 5.6 11.3 7.3 30 BID n = 153 30 QD n = 156 60 QD n = 153
. Trial design: Patients with recent ACS were randomized to receive in a 1:1:1:1:1:1:1 fashion either placebo or darexaban 5 mg BID, 10 mg QD, 15 mg BID, 30 mg QD, 30 mg BID, or 60 mg QD. Patients were followed for 6 months. Results Conclusions Steg G, et al. Eur Heart J 2011;Aug 30:[Epub] (p = 0.009) In this phase II trial, darexaban, an oral anti-Xa agent, was associated with increased bleeding without an improvement in ischemic outcomes in patients with ACS already on aspirin and clopidogrel Similar results were noted with other anti-Xa agents such as apixaban Major and clinically relevant bleeding 0 20 % Placebo n = BID n = BID n = QD n = BID n = QD n = QD n = 153.")
107
Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary Syndromes Vorapaxar was not effective in reducing the primary cardiovascular efficacy end point, and it increased rates of bleeding, including serious bleeding and intracranial hemorrhage.Vorapaxar was not effective in reducing the primary cardiovascular efficacy end point, and it increased rates of bleeding, including serious bleeding and intracranial hemorrhage.

108
Placebo n = 5176 ASA + Thieno, n = 4821 ASA, n = 355 Recent ACS: STEMI, NSTEMI, UA No increased bleeding risk, no warfarin, no ICH, no prior stroke if on ASA + thienopyridine Stabilized 1-7 days after index event PRIMARY ENDPOINT: EFFICACY: CV death, MI, stroke* SAFETY: TIMI major bleeding not associated with CABG Event-driven trial of 1002 events in 15,342 patients RIVAROXABAN 5.0 mg BID n = 5176 ASA + Thieno, n = 4827 ASA, n = 349 Stratified by thienopyridine use at MD discretion + ASA 75 to 100 mg/day RIVAROXABAN 2.5 mg BID n = 5174 ASA + Thieno, n = 4825 ASA, n = 349 ATLAS ACS 2-TIMI 51: Design

109
HR, 0.84 (95% CI, 0.74-0.96) P =.002 Pooled 2.5 mg and 5.0 mg BID doses Placebo Pooled rivaroxaban CV Death, MI, Stroke (%) ATLAS ACS 2-TIMI 51: Efficacy Endpoint Placebo
 P =.002 Pooled 2.5 mg and 5.0 mg BID doses Placebo Pooled rivaroxaban CV Death, MI, Stroke (%) ATLAS ACS 2-TIMI 51: Efficacy Endpoint Placebo")
110
P =.002 NNT = 63 P =.002 NNT = 71 Proportion of Population (%) P =.002 NNT = 63 ATLAS ACS 2-TIMI 51: 2.5 mg BID
 P =.002 NNT = 63 ATLAS ACS 2-TIMI 51: 2.5 mg BID")
111
ATLAS ACS-TIMI 51: Stent Thrombosis Stent Thrombosis (%) 47/5115 ARC = Academic Research Consortium
 47/5115 ARC = Academic Research Consortium")
112
P <.001 Population (%) ATLAS ACS 2-TIMI 51: Bleeding P =.009 P =.66 P values for both doses vs placebo
 ATLAS ACS 2-TIMI 51: Bleeding P =.009 P =.66 P values for both doses vs placebo")
113
Diagnosis of UA/NSTEMI is Likely or Definite ASA (Class I, LOE: A) Clopidogrel if ASA intolerant (Class I, LOE: B) Select Management Strategy Initial Conservative Strategy or UnknownInvasive Strategy† Initiate anticoagulant therapy (Class I, LOE: A) Acceptable options include Enoxaparin or UFH (Class I, LOE: A) Fondaparinux (Class I, LOE: B)* Enoxaparin or fondaparinux preferred over UFH (Class IIa, LOE: B) Initiate clopidogrel (Class I, LOE: B) Initiate anticoagulant therapy (Class I, LOE: A)* Acceptable options include Enoxaparin or UFH (Class I, LOE: A) Bivalirudin (Class I, LOE: B) CABG: Maintenance ASA (Class I, LOE: A) Medical Therapy: D/C GP IIb/IIIa inhibitors if begun and give clopidogrel per conservative strategy Precatheterization: Add second antiplatelet agent (Class I, LOE: A)‡ Clopidogrel (Class I, LOE: B) or GP IIb/IIIa inhibitor (Class I, LOE: A) (IV eptifibatide or tirofiban preferred) Next step per triage decision at angiography PCI: Class I: Clopidogrel (if not begun precatheterization) (LOE: A) or Prasugrel (LOE: B) or Selectively, a GP IIb/IIIa inhibitor (if not begun precatheterization) (LOE: A) Wright RS, et al. J Am Coll Cardiol. 2011;57(19):1920-59. *If fondaparinux is used with an invasive strategy (Class I, LOE: B), it must be coadministered with another anticoagulant with Factor IIa activity, i.e., UFH.) †Timing of invasive strategy generally is assumed to be 4 to 48 hours. If immediate angiography is selected, see STEMI guidelines. ‡Precatheterization triple antiplatelet therapy (ASA, clopidogrel, GP inhibitors) is a Class IIb, LOE: B rec for selected high-risk patients.
: *If fondaparinux is used with an invasive strategy (Class I, LOE: B), it must be coadministered with another anticoagulant with Factor IIa activity, i.e., UFH.) †Timing of invasive strategy generally is assumed to be 4 to 48 hours. If immediate angiography is selected, see STEMI guidelines. ‡Precatheterization triple antiplatelet therapy (ASA, clopidogrel, GP inhibitors) is a Class IIb, LOE: B rec for selected high-risk patients..")
114
THANK YOU

Similar presentations













 Trial Comparison of the safety and efficacy of unfractionated heparin versus enoxaparin in combination.>")


















