Download presentation
Presentation is loading. Please wait.

1
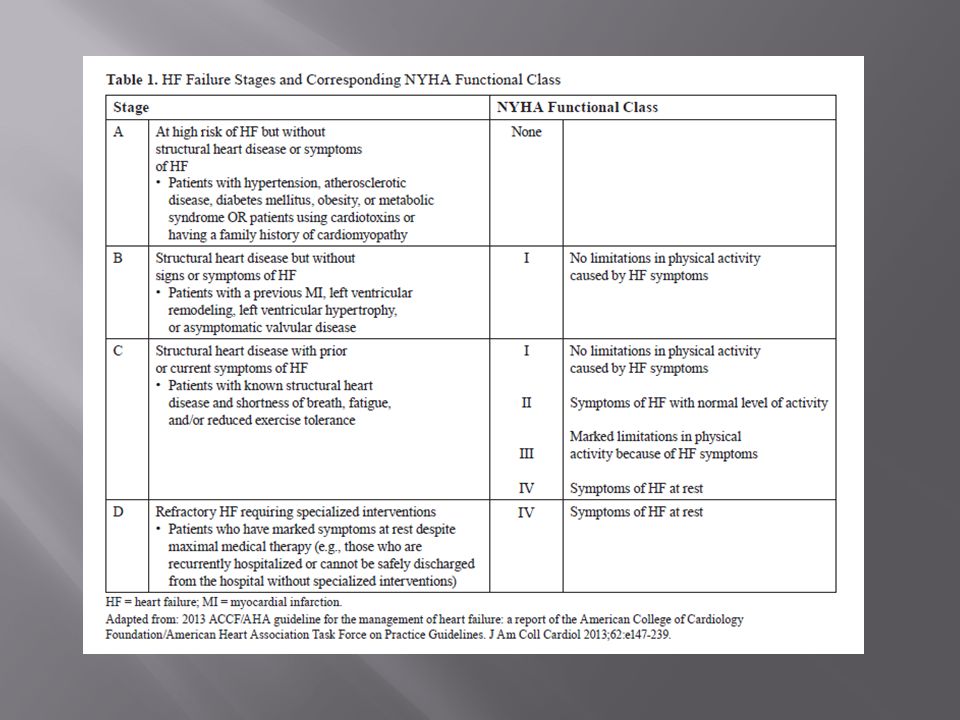
2013 American College of Cardiology American Heart Association

2
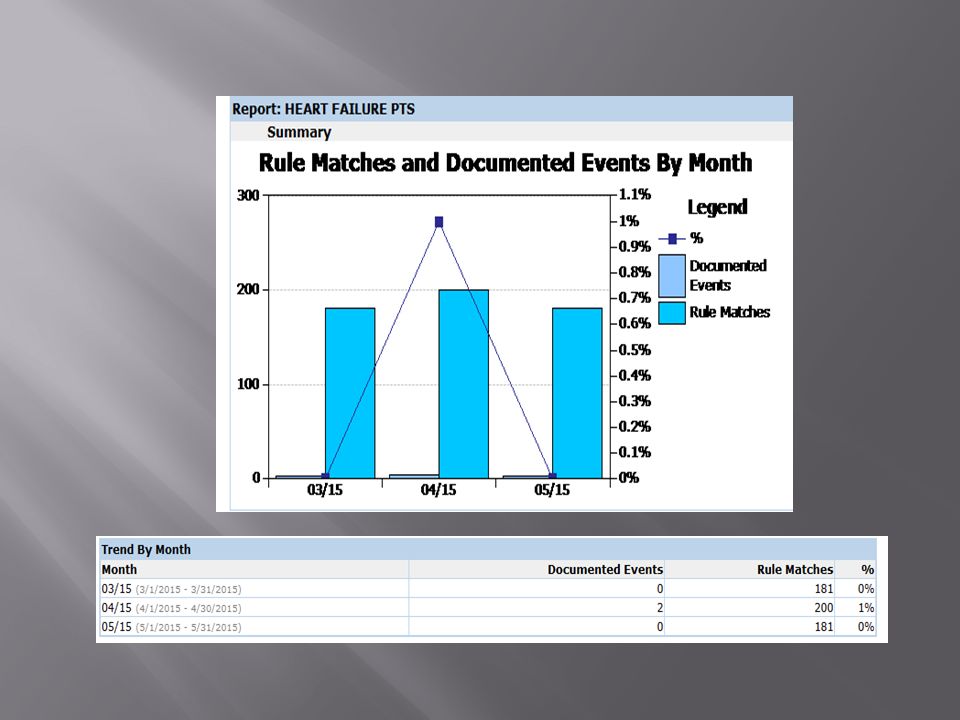
The prevalence of CHF is about 8-10% in the over 65YO population. There is a large incidence of readmissions to hospitals today because the patients key medications are not in use or because other meds are exacerbating their condition.

6
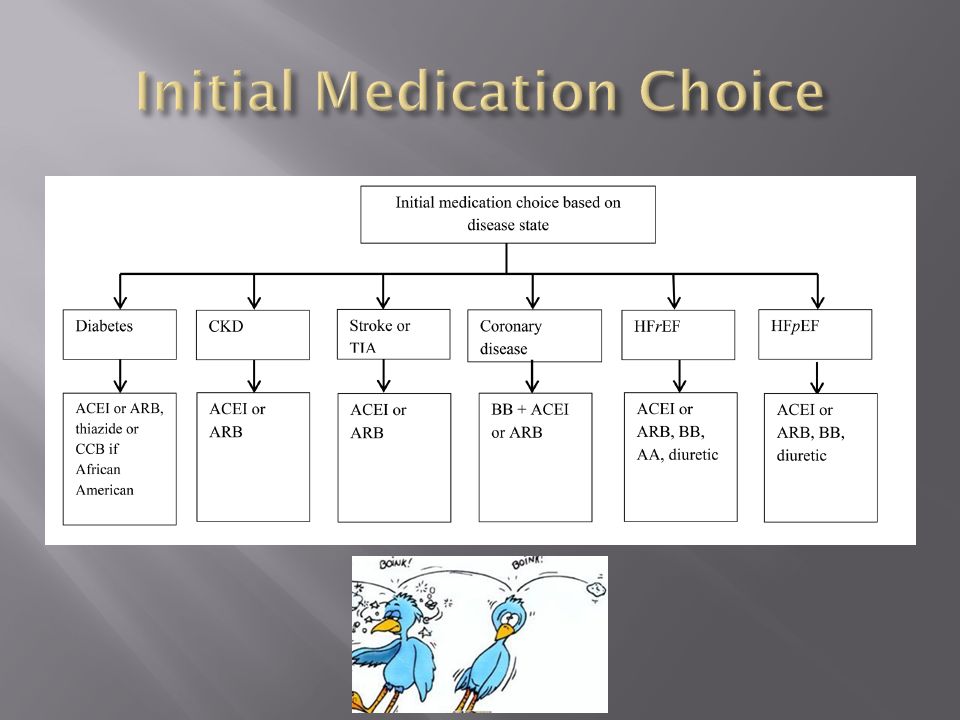
RIGHT-SIDED-DIASTOLICLEFT-SIDED-SYSTOLIC LVEF > 50% Thickened-ventricle 30% of HF pts 60-89% caused by HTN LVEF <= 40% Dilated Ventricle 70% of HR Pts 66% caused by CAD

9
Preserved Left Ventricular Function - Hypertrophic Walls -Coronary Artery Disease -Valvular Stenosis -Congenital Structural Abnormality -Pulmonary Hypertension -Hypertension

11
Angiotensin II receptor blockers 13 % Calcium Channel Blockers 11% Angiotensin converting enzymes 10% Diuretics 8% Beta Blockers 6% Digoxin – is not used in Diastolic Heart Failure (non-dihydropyridine CCB ‘only’ should be used.. Goal- increase filling time of ventricles)
.")
12
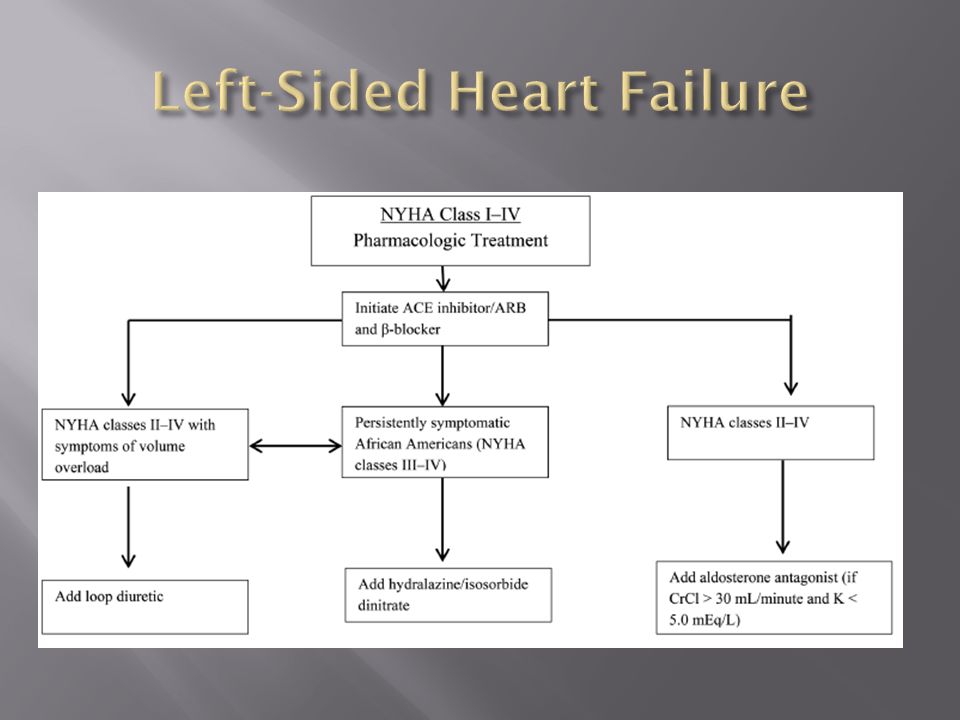
Beta-Blockers- 35% RRR DECREASE IN MORTALITY Ace-Inhibitors- 25-50% DECREASE IN MORTALITY Aldosterone antagonist (or hydralazine Plus a nitrate)- 30% DECREASE IN MORTALITY Diuretics- No decrease in mortality Digoxin- No decrease in mortality
- 30% DECREASE IN MORTALITY Diuretics- No decrease in mortality Digoxin- No decrease in mortality")
14
One year mortality rate: Males= 28% Females= 24% Five year mortality rate: Males= 59% Females= 45%

15
Reduce Mortality Rate by 35% relative risk reduction Reduce Hospitalization by 25% relative risk reduction Symptom improvement Produce greater symptom improvement & risk reduction than ACE inhibitors.

16
Blocks Norepinephrine & other neurotransmitters. Decrease Ventricular arrhythmias Decrease cardiac hypertrophy Decrease Vasoconstriction & HR

17
- First choice of med to implement - Bisoprolol, Carvediol, Metoprolol - Start Low and titrate up. Decreases vasoconstriction, decreases arrythmias, decreases sympathomimetic tone - Goal- HR= 55-60 bpm (<50 if angina persist) - Precautions-Bradycardia, Heart Block, Asthma
 - Precautions-Bradycardia, Heart Block, Asthma.")
20
Use in all pts with Left Sided HF Lowers Vasoconstriction, decreases both pre-load and post-load. - All Ace-Inhibitors are considered equivalent - Start Low and titrate up. - Implement Beta-blocker first

21
Mortality rate for males without ACE= 52% with ACE=36% NYHA class II to III Mortality rate without ACE= 25% with ACE= 18-20% Asymptomatic left ventricular dysfunction Mortality rate in 3 yrs without ACE=39% with ACE=30%

22
Bob is a 68 YO male admitted by Dr. Hilgeford from a NHP for PNA. Patient treated for 2 weeks on Vancomycin, thoracentesis was done and obtained 500ml of clear fluid with no neutrophils. proBNP= 2500, SCr= 1.5 WBC was normal, afebrile. PMH: included Past MI, Edema in LE DM, COPD. Current Meds: carvediol 12.5mg q12hr, Furosemide 80mg iv q12h, Lantus, Novolog, Advair, Spiriva What change would you make?

24
Hold Ace-Inhibitors if Scr > 30% Hold Ace-Inhibitors if crcl < 30 ml/min Heavy Diuresis Expect some slight rise when giving Ace- Inhibitors.

25
The studies done with B-blocker, Ace, Spironolane inhibitors- were in stabilized Outpts. 1 st get B-blocker on board and titrate it Don’t give ACE when they are being diuresed

26
BPS GUIDELINESMAJOR POINTS

27
Decrease both pre- load and post load on heart Decrease pressure in Kidney (less Proteinuria) Vasodilation with drop in BP.
 Vasodilation with drop in BP.")
28
Consider in all pts with LVEF < 40% Spironolactone 12.5-25 mg/day Eplerenone 25-50mg/day-no gynecomastia Precautions: Hyperkalemia, avoid use if Scr>2.5mg/dl or crcl < 30ml/min

29
ACE Rate discontinue- 23% Hypotension- 4.8% Doubling scr- 1.9% Hyperkalemia- 3.3% Cough- 4.2%-9% Angioedema- 0.3% ARB 24% 1.7% 2% 3.4% 1.1%-3.2% 0.1% Studies: ELITE II, ONTARGET…. ARB may be slightly less beneficial than ACE for HR patients. They are still shown to be beneficial.

33
Decreases coronary vascular resistance & increases coronary blood flow. Negative inotropy.. Nifedipine much more than amlodipine and felodipine Decrease HR (verapamil,diltiazem only) –thus decrease oxygen demand. Contraindcations for non-dihydropyridines: LV dysfunctions (except for amlodipine & felodipine)
 –thus decrease oxygen demand. Contraindcations for non-dihydropyridines: LV dysfunctions (except for amlodipine & felodipine).")
34
Ventricular Premature Beats =70-95% of HR beta blockers, amiodarone, anticoags Renal Failure-- Diuretics,no ace?, Atrial Fib- anticoagulants Strokes/TIAs – anticoags -

35
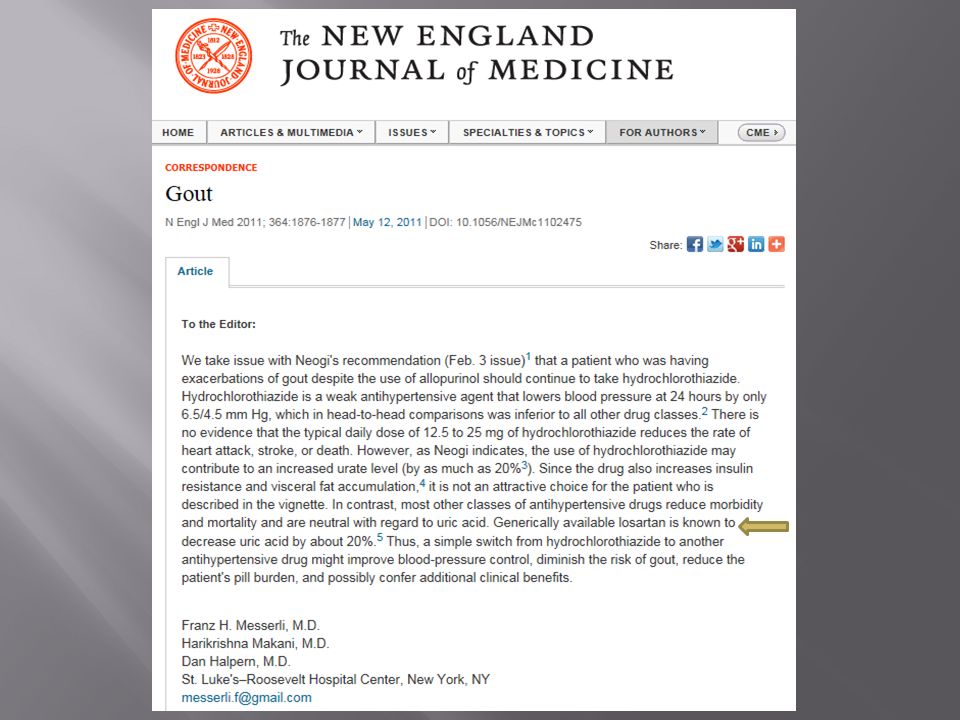
CASE STUDYMEDICATIONS Jason is a 79 YO CHF on Lisinopril, metoprolol, allopurinol, and amlodipine is admitted for CHF exacerbation and flairup of gout. The Physician starts HCTZ 25 mg for CHF and Ibuprofen and Solu- Medrol for gout. What problems would you anticipate? Lisinopril Metoprolol Allopurinol HCTZ Ibuprofen Solu-Medrol

37
NSAIDS Minoxidil Metformin Cilostazol Itraconazole Class I & II Antiarr ( except for amiodarone and dofetilide) Calcium Channel Blockers (except amlodipine & Felodipine) Corticosteroids Thiazolidinediones Amphetamine Pregabalin Hormonal Therapies
 Calcium Channel Blockers (except amlodipine & Felodipine) Corticosteroids Thiazolidinediones Amphetamine Pregabalin Hormonal Therapies")
38
Calcium channel blockers might be expected to have beneficial effects in systolic HF by reducing peripheral vasoconstriction and thereby reducing left ventricular afterload. However, these agents also have negative inotropic activity and several studies demonstrated greater clinical deterioration in patients treated with nifedipine and diltiazem compared to placebo or isosorbide dinitrate [2,3]. As a result, these drugs have generally been avoided in patients with systolic HF, even for the treatment of coexisting angina or hypertension. The second-generation calcium channel blockers amlodipine and felodipine have little or no negative inotropic activity at the usual therapeutic doses, and may be better tolerated than the other calcium channel blockers in patients with HF

39
In patients with HF due to systolic dysfunction, chronic use of oral PDE-3 inhibitors for inotropic therapy have been associated with increased mortality compared to placebo. Cilostazol is a PDE-3 inhibitor approved for the treatment of intermittent claudication. While it is not established that cilostazol impacts mortality in patients with HF, the FDA regards HF of any severity as a contraindication to the use of cilostazol

40
NSAIDS… increase the exacerbation of preexisting HF. Increased risk of rehospitalization was noted with diclofenac and ibuprofen (Naproxen is the only NSAIDS which does not increase risk of MI, stroke, and death. (in doses < 500mg) Aspirin is still recommended for it’s antiplatelet effects. If NSAIDS are employed with aspirin, Naproxen is the recommended choice. NSAIDS are associated with an increased thrombotic even including MI and stroke. Some NSAIDS may potentially interfere with aspirin’s cardioprotective effect. NSAIDS are contraindicated for perioperative pain in CABG CONCLUSION: Avoid NSAIDS in heart failure. Especially with recent MI or ACS
 Aspirin is still recommended for it’s antiplatelet effects. If NSAIDS are employed with aspirin, Naproxen is the recommended choice. NSAIDS are associated with an increased thrombotic even including MI and stroke. Some NSAIDS may potentially interfere with aspirin’s cardioprotective effect. NSAIDS are contraindicated for perioperative pain in CABG CONCLUSION: Avoid NSAIDS in heart failure. Especially with recent MI or ACS.")
41
Gout…. Use of NSAIDS Crohns...Use of Steroids COPD… Use of Steroids RA…….. NSAIDS and some DMARDS PVD…… Cilostazol

Similar presentations













 Garrett J. Gross, Ph.D. Drugs Used In the Treatment of Congestive Heart Failure(Cont) Garrett.>")

, means your heart can't pump enough blood to meet your body's.>")

. CARDIOVASCULAR DISEASE AND DRUGS ► Basic cardiovascular physiology and pathology depends on the control of heart.>")








